Case 4 Frontal Sinus Fractures
4.1 Description
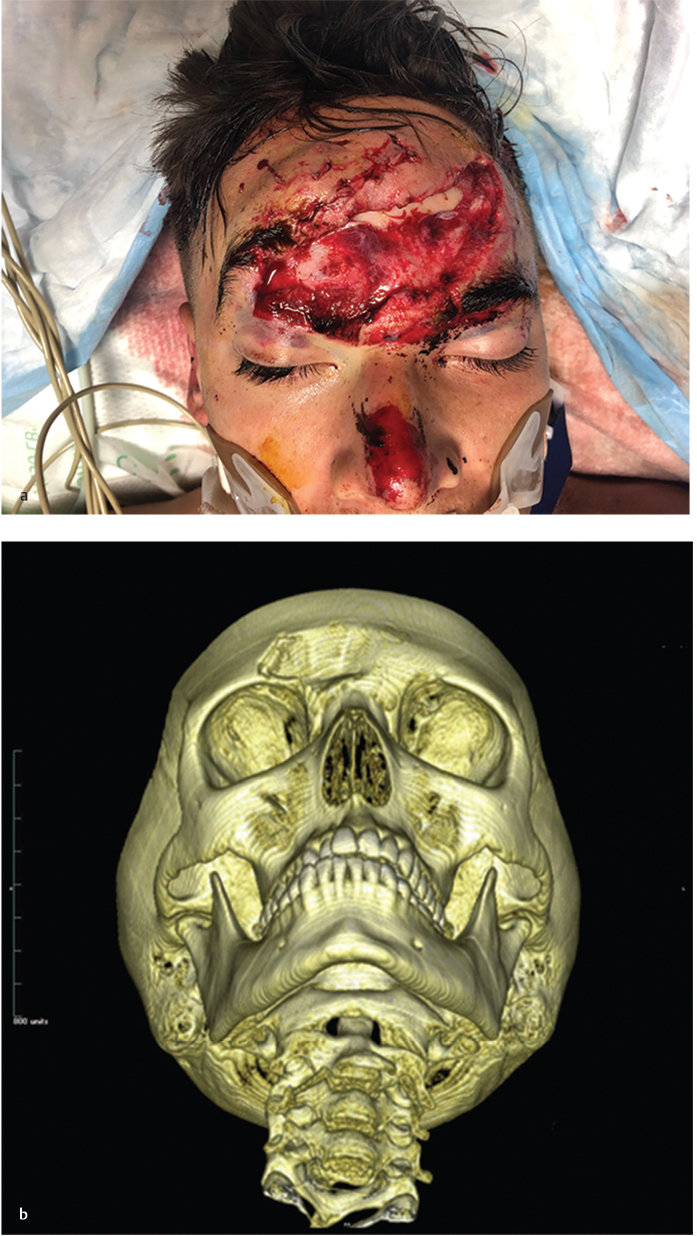
Large avulsion of the forehead involving the brow
Computed tomography (CT) demonstrates depression of the anterior table of the frontal sinus
Status of the posterior table of the frontal sinus and nasofrontal outflow tract is unknown and must be elucidated
4.2 Work-Up
4.2.1 History
Mechanism of injury
Blunt versus sharp
High energy of impact raises concern for additional injuries
Change in vision, loss of vision, or double vision
Must rule out orbital injuries prior to considering operative intervention
Numbness of forehead: Injury to V1 distribution
Rhinorrhea: Concern for dural injury and cerebrospinal fluid (CSF) leak
4.2.2 Physical Examination
ABCs and primary survey: Identify any potentially life-threatening conditions
Greater suspicion depending on mechanism and greater force of injury
Identify lacerations over the forehead, glabella, or supraorbital ridge
May be utilized for direct access in repair
Palpate for step-offs and/or depressions in the frontal area
Edema often masks contour deformities
Evaluate for sensory changes in supraorbital/supratrochlear nerves
Test function of frontalis and corrugator muscles of forehead
Examine for nasal drainage: Must rule out CSF rhinorrhea
Ring test at the bedside: CSF will separate on filter paper and create a double ring or halo sign
Beta-2 transferrin is the definitive test for CSF, but it may take several days to obtain the results
4.2.3 Pertinent Imaging or Diagnostic Studies
High resolution maxillofacial CT scan of both axial and coronal planes
Evaluate for injury to anterior and posterior tables; determine degree of comminution/displacement
Evaluate nasofrontal outflow tract for ability to drain the frontal sinus
Identify intracranial injuries (e.g., pneumocephalus, etc.) and other facial fractures
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


