Case 3 Mandibular Fractures
3.1 Description
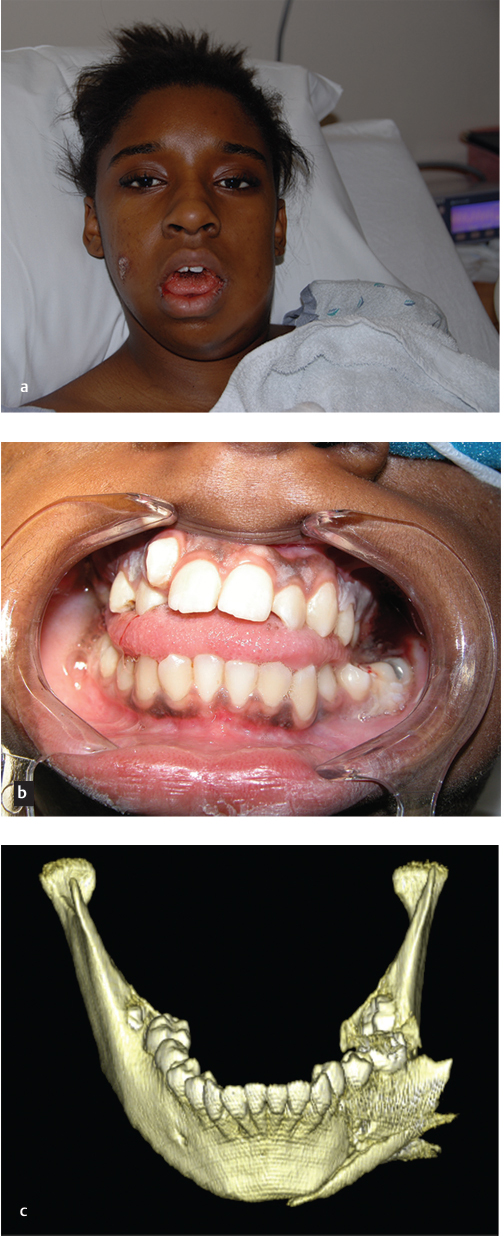
Bullet hole in right cheek, exit site presumed to be IN left jaw
Displaced, comminuted body and angle fracture of the mandible with large butterfly fragment and malocclusion on examination
Unclear facial nerve function or evidence of parotid injury
3.2 Work-Up
3.2.1 Initial Assessment
ABCs: Attention to patency of the airway given multiple mandibular fractures. Intubation may be necessary if the patient cannot protect the airway.
Cervical spine precautions: This is mandatory in the setting of high energy injuries until the spine is cleared both clinically and radiographically.
Concomitant injuries: Manage any potentially life-threatening injuries first. The repair of mandibular fractures is not emergent and can be performed on an elective basis (generally within 14 days of injury).
3.2.2 History
Mechanism of injury, presence/location of pain, loss of sensation, presence of loose or missing teeth, use of dentures, assessment of occlusion
Relevant medical history (prior mandibular or facial fractures), surgical history (prior facial surgery), social history (alcohol, smoking, drug use)
3.2.3 Physical Examination
Palpate bony structures in a systematic fashion to identify areas of tenderness, deformity, step-off, and instability.
Assess mobility (ability to open/close mouth, deviation of mandible on movement) and occlusion (may be evaluated based on wear facets of teeth)
State of dentition: Edentulous mandibles will require more aggressive procedures to rigidly fixate bone segments due to decreased bone stock.
Evidence of intraoral lacerations (exposed bone), loose or absent teeth, identification and removal of prosthetics (dentures), sublingual hematoma, or foreign bodies
Neurologic examination: The mental/inferior alveolar nerve provides sensation to the lower lip. The marginal mandibular branch of the facial nerve innervates the depressors of the lower lip and is rarely injured.
In gunshot wounds, must consider all structures in path of bullet, including parotid, facial nerve, muscle, tongue, and other intraoral injuries.
Assess presence of concomitant midfacial fractures (may alter occlusion).
3.2.4 Pertinent Imaging or Diagnostic Studies
High-resolution maxillofacial computed tomography (CT): Gold standard for imaging. Three-dimensional reconstructions may assist in further evaluating injury.
When CT is unavailable, X-ray studies may be useful.
Option 1: Panorex. Visualization of entire mandible and dentition. Limited evaluation at symphysis and condyles. Additional Towne’s view improves evaluation of subcondylar regions.
Option 2: Mandible series (anteroposterior”. lateral, and bilateral oblique views)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


