Fig. 44.1
Raffaello Sanzio “the Three Graces”

Fig. 44.2
The Bushman woman
This constant augmentation of requests for treatment of the gluteus area has brought us to create and perfect an intervention combining liposuction and lipostructure with the concept of modeling the profile of the patient’s body while modifying and correcting the convexity and concaveness of the body, which is not a straight line but simply superficial curves that are concave or convex but rarely flat (Fig. 44.3).

Fig. 44.3
Correct shape of the buttocks
The philosophy of this treatment acquires increased value from the fact that it does not require the use of any type of prosthetic material. It is an intervention with permanent results and always combines the improvement of the buttocks area with reduction of all areas of lipoaccumulation. The patients to whom this type of treatment is proposed generally accept with a great deal of enthusiasm and are especially attracted by the results demonstrated in pre- and post-intervention photos of patients.
44.2 Normal Anatomy
The gluteus area is essentially formed by four structures: bone, muscles, skin, and under-skin tissues (Fig. 44.4). Above all, there is a basic characteristic shape of the buttocks that is different among the two sexes and the various races. Typically, a woman tends to accumulate adipose tissue in a gynoid manner, with progressive accumulation of adipose tissue in the external thigh area and in the hips. Often the accumulation is in the sacrum area. The gluteus itself, beneath the dermis, is subject to the phenomenon of lipoaccumulation, panniculopathy, and the formation of stretch marks. Only from this we can attribute the steatopygia of Bushman women to the cases of the development of adipose tissue under the skin (Fig. 44.5).


Fig. 44.4
Anatomy composites
Fig. 44.5
Venus from the 1,800 s
Men, differently, do not experience significant variations of volume subcutaneously. However, they may have defects of the form and trophism of the skin. These modifications are also related to the differences in weight which a patient experiences during a lifetime.
Effectively, in the aging process, the only structures which do not undergo appreciable changes are the bones, while the muscles can undergo variations of trophism both in men and in women. The subcutaneous fat layer can undergo variations of both form and substance directly correlated to the variations of the trophism of the overlying skin. In time, the anatomical structures under the skin and the skin itself are subjected to the force of gravity, and, thus, ptosis of the buttocks is inexorable.
The gluteus zone is convex and rounded in all its extensions, thus representing a hemispheric shape that is unique to the human species. This is due to the evolution of the human species’ capability to stand erect, and, in fact, the large muscles of the gluteus are responsible for straightening the pelvis on the thighs to arrive at a vertical position.
There are some anatomical classifications that determine gluteus aesthetics [1–4], which include four main forms [3]: A, V, round, and square shapes (Fig. 44.6). The authors arrived at this classification considering the line which is achieved by connecting the point A, which is the most external point of the upper area of the gluteus, in relation to the external area of the hips, corresponding to the most external area of the hips, to the point B, the inferior section of the gluteus, which is the external thigh (Fig. 44.7). This classification evaluates the point C, as a central lateral point of the gluteus, which approximately corresponds to the middle point between A and B (Fig. 44.8).

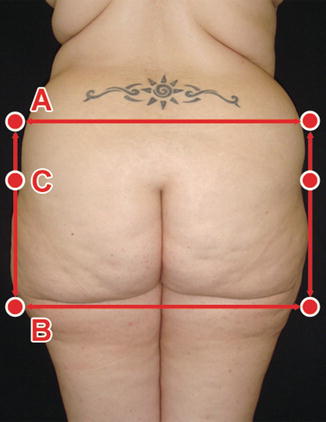
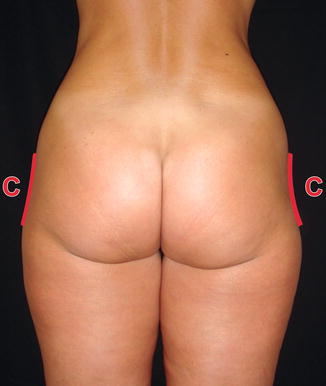
Fig. 44.6
Main form of the gluteus. (a) A shape. (b) Round shape. (c) Square shape. (d) V shape
Fig. 44.7
Point B
Fig. 44.8
Point C
The gluteus area is situated in the posterior of the hip under the ileum-costal area, between the sacrum-coccyx area in the back and the femoral region in front. Its upper boundary is indicated by the curved form of the iliac crest, which is evident to the touch via the integument. The lower limit corresponds to the gluteus-femur fold, due to the adherence of the skin to the fascia; generally the lateral margin corresponds to the intergluteus furrow on the lower part and the sacrum-coccyx column on the upper area (Fig. 44.9). Laterally, the boundary corresponds to the vertical line which connects the most external part of the iliac spine (point A) to the most external point of the trochanteric area (point B).
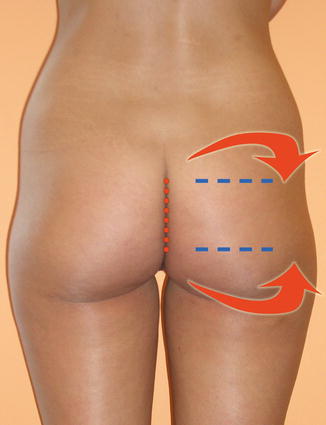
Fig. 44.9
The lateral margin corresponds to the intergluteus furrow on the lower part and the sacrum-coccyx column on the upper area
The skin of the gluteus area is thick, as is the subcutaneous adipose tissue, which forms a sort of elastic cushion to protect it from external pressure. There is also a cushion of adipose tissue situated deep to the large gluteus muscle and called the under-gluteus adipose layer. This is not relevant to the augmentation of gluteus volume in women due to lipoaccumulation.
The muscular component is formed by two planes, one superficial and one deep. The superficial layer consists of two muscles: lower and central is the large gluteus muscle and high and lateral is the middle gluteus. The large gluteus muscle is a quadrilateral, 6–7 cm deep that extends from the pelvic area to the upper lateral portion of the femur. The medial gluteus is as large as an open fan, positioned below the large gluteus muscle that, however, emerges higher and further in front. It is inserted laterally at the iliac crest in its three upper back quarters and with a thick tendon that is inserted at the lateral strip of the large trochanter.
The deep muscle layer, instead, is formed of muscles that (from high to low) consist of the small gluteus, the pyriformis, the upper gemellus, the internal shutter, the lower gemellus, the external shutter, the femur quadrant, and finally the upper extremity of the femur biceps, semi-tendon-like and semi-membrane-like. The large trochanter is wide and supports the majority of the gluteus mass. The pelvic bones, however, also consist of the sacrum and the coccyx, which are strictly united by sacrum-tuberous and sacrum-spinous ligaments (Fig. 44.10). Different from the stable bone structure that is not susceptible to modifications, the relationship between height and width of the large gluteus muscle influences the aesthetics of this area. In the front to back and, above all, in the side visual, this relationship can be clearly evaluated. This evaluation is important before deciding where to implement the remodeling of the gluteus.
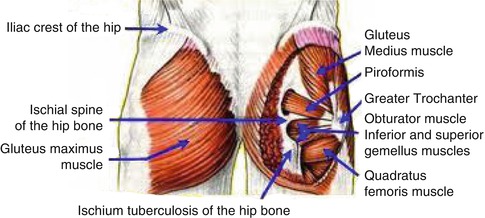
Fig. 44.10
Gluteus anatomy
The sacral area must always be well defined and thus treated with a very aggressive liposuction so as to create a depression in this area, in all cases concerning deposits of adipose tissue. For cases in which the adipose tissue is scarce, the area which will see greatest improvement from lipostructure is the upper margins of the gluteus. This permits better definition of the large gluteus muscle, with its insertion in a semicircular form along the iliac crest.
Another variable to consider is the site of the insertion of the large gluteus muscle along the entire iliac crest, which depending on the highest or lowest level of insertion creates a proportion which might vary between 0.5:1 and 1:1 in the presacral area and L5–S1 in the large gluteus muscle (Fig. 44.11). This also signifies an analysis of the ideal length of the intragluteus fold, which should be always major than the presacral region length (Fig. 44.12).
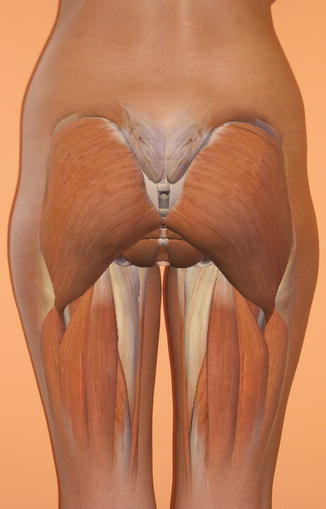
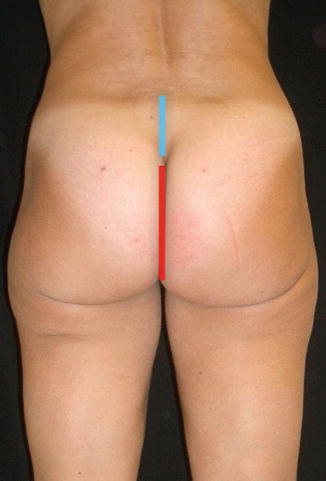
Fig. 44.11
Gluteus muscle insertion
Fig. 44.12
Ideal length of the intragluteus fold (red line). Pelvic rim to intragluteal fold (blue line)
Regarding the vascular system, the subcutaneous layer contains only superficial arteries of minor importance and underneath houses three branches of the internal iliac vascular system which serves only the gluteus. The upper gluteus artery is divided into two branches, one between muscles of the large and medium gluteus and the other deeper, between the medium gluteus muscle and the small gluteus muscle. The lower gluteus artery exits from the pelvis through the sciatic furrow, directs downward, and divides into two branches: the rear branch for the large gluteus muscle and the skin which covers it and the lower branch for the rear tissue of the thigh. The internal pudendal artery also exits from the pelvis through the large sciatic furrow and provides a vascular system for the perineum area. The veins of the gluteus area are divided into superficial and deep. The first ones form a thick subcutaneous network connected to the thigh and abdomen. The veins, instead, accompany the gluteus and the internal pudendal arteries, with two for each one.
The nerves are divided into superficial cutaneous and deep, in four trunks consisting of the upper gluteus nerve that passes next to the upper gluteus artery and serves the medium and the small gluteus muscles, terminating in the tensor of the lateral fascia. The small sciatic nerve serves the large gluteus muscle and the skin above it and terminates in the perineum to the scrotum. The sciatic nerve passes the sciatic spine and then runs lower covered by the large gluteus muscle at the back portion of the thigh.
44.3 Technique (Figs. 44.13 and 44.14)

Fig. 44.13
Serdev suture suspension lift

Fig. 44.14
Serdev needles
With this technique, the authors wants to link simplicity and rapidity of execution to the lifting of the gluteus. This new treatment is the method of scarless “Serdev suture suspension lift” utilized to correct falling and flaccidity of the tissues of the face and other areas of the body. In the face, it is possible to treat the temple area, the malar area, the eyebrows, the projection of the chin without implants, and the tip of the nose, while in the body, it is possible to treat the gluteus. This method, which uses elastic sutures without incisions, substitutes in some cases the lifting with incision of the face and the dermalipectomy of the body, creating a lifting of the skin in one direction only.
It is a mini-invasive intervention, with minimum trauma to the tissues, and does not involve scarring, but instead only transitory puncturing of the skin. It is performed in day surgery with local anesthetic and normally with a little swelling and ecchymosis. It permits a more rapid return to normal activities. The indication for the correction of the gluteus is ptosis. The intervention consists in the realization of a loop with a permanent and resistant elastic suture, which passes from the superior margin of the large trochanter and then runs in the deep layer of subcutaneous tissue, passing first below the intergluteus fold to then be tied at the upper margin of the large trochanter and embedding the point below the skin. Being a loop, it results in a suspension and a cone-like projection of the gluteus, for an attractive lifting and outward shape (Fig. 44.15).
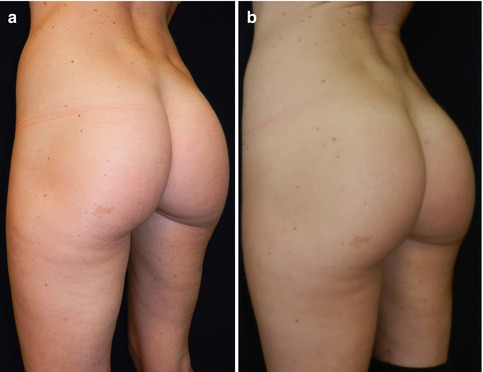
Fig. 44.15
Serdev suture suspension lift. (a) Preoperative. (b) Postoperative
44.4 The Gluteoplasty
The first enlargement of the gluteus was performed in 1969, by Bartels et al. [5] who used a pair of normal mammary prostheses. In 1991, Gonzalez-Ulloa [6] published a report detailing 10 years of experience with gluteoplasty with prostheses.
Although it has been practiced for many years, gluteoplasty with prostheses has not reached an ample diffusion in the world of aesthetic surgery, and there are few surgeons who perform it. In 2002, in the 1,620,502 interventions of aesthetic surgery performed in the United States by physicians specialized in plastic surgery, the number of gluteoplasty was only 614. Among the reasons for this limited diffusion, we must certainly consider the newness of the procedure, still unknown to many but above the risk of complications following the implantation of gluteus prostheses, which is not to be ignored. The implantation of gluteus prostheses does not have a positive reputation among aesthetic surgeons, both for a rather high frequency of complications and also because it was performed for a long time only in countries with scarce control of the medical profession and a low level of protection for the patients. Only recently, with the increased number of requests for this type of surgery, it has been possible to have controlled statistics which do not seem to confirm the bad reputation of gluteoplasty with prostheses. Perhaps this will result in a greater diffusion of this technique in the near future.
The implantation of gluteus prostheses is indicated in patients with a good muscle mass and a small adipose component who desire to augment the dimension of the gluteus and who at the same time are too thin to offer sufficient adipose accumulation for the enlargement with the lipofilling technique. Good muscle tone, along with elastic and good thickness skin, is requested (Fig. 44.16).

Fig. 44.16
Gluteus prostheses
Related posts:
 Stem Cell Applications: An Overview
Stem Cell Applications: An Overview
 The Adipose Organ: Morphological Perspectives of Adipose Tissues
The Adipose Organ: Morphological Perspectives of Adipose Tissues
 The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
 Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
 Hand Rejuvenation with Stem Cell Fat Transfer
Hand Rejuvenation with Stem Cell Fat Transfer
 Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


