18 Burns Abstract Burns are one of the most devastating traumatic injuries, mainly affecting the most vulnerable population groups (children, women, and elderly) living in the poorest social conditions. Thermal injuries occur by an increase in temperature able to cause tissue damage. The most frequent etiologic agent is fire/flames, closely followed by scalds. Aside from local destruction (coagulative necrosis), when burn injuries involve > 20% of the total body surface area the systemic inflammatory response puts life at risk: the shock in the acute phase and the sepsis for the rest of the evolution are the leading causes of death. Inhalation injury in the context of a fire/flame burn dramatically worsens the prognosis. Primary assessment of the burned patient must follow the Advanced Trauma Life Support guidelines, and major burns demand transfer to a burn unit. Accurate diagnosis of burn depth is the main challenge because early and definitive coverage with skin grafts remains the gold standard definitive treatment. Other traumatic agents, such as electricity, chemicals, and cold, can also cause tissue damage that resembles a thermal injury. Although an increase in temperature may coexist in some circumstances, the main injurious mechanisms of these other agents are different, and they are classified as nonthermal injuries. Keywords: burn, chemical injury, cold injury, electrical injury, nonthermal injury, thermal injury Thermal injury can be defined as a traumatic injury caused by a temperature increase beyond a threshold able to cause tissue damage. Etiologic factors are contact with hot elements (solids, liquids or scalds, gases), thermal radiation (fire/flames, sun, infrared lamps, etc.), and mechanical friction. Other nonthermal traumatic agents, such as electricity, chemicals, and cold, can also cause tissue damage with an appearance and behavior reminiscent of a burn injury; however, they have a singular pathophysiology, clinical presentation, and treatment. According to the latest estimates, 973 million people suffered some kind of traumatic injury that required medical care in 2013. Of these, 31 million were injured by fire/flames, heat, and hot substances (337 injured/100,000 inhabitants), resulting in 12.3 million years of disability-adjusted life years (DALYs). Even though the global rate of DALYs has fallen by 33% since 1990, in regions like sub-Saharan Africa, Oceania, eastern Europe, and the Caribbean this figure remains relatively unchanged. The population distribution of thermal injuries is one of the most unjust among traumatic injuries, with the most vulnerable population groups being children, the elderly, and women. Over 95% of deaths from fire/flames burns are concentrated in lowand middle-income countries, and in high-income countries, they affect the poorest social sectors. According to the 2015 National Burn Repository of the American Burn Association the most frequent etiologic burn agent is fire/flames (43%), followed by scalds (34%), contact with hot objects (9%), electrical injuries (4%), and chemical injuries (3%). While electrical and chemical etiologies occur mainly in work-related industrial settings, the rest of the agents are more common outside the workplace. Of note, high-voltage electrical injuries have been related to illegal sales of copper in times of economic crisis. Most adults suffer burns by fire/flames followed by scalds, men commonly at the workplace and in outdoor accidents, whereas women and the elderly usually at home. Children sustain burns mainly by scalds at home, followed by contact with hot objects in younger than 2 years and fire/flames in older than 2 years. Described risk factors for burns are poverty, unemployment, illiteracy, overcrowding, nonwhite race, toxic habits (tobacco, alcohol, and drugs), epilepsy, sensory deficits (blindness, deafness, neuropathy), motor deficits (arthritis, paraplegia), and mental and psychiatric deficits. Particular risk factors in children include the presence of preexisting impairments, lapses in child supervision, storage of flammable substances at home, and low maternal education level. Cold injuries are a well-documented problem in countries with extreme temperatures and frequent among military personnel during wartime, alpinists, and the homeless, and following occupational accidents with refrigerants and propellants (Freon gas, liquid nitrogen, carbon dioxide). About 3–10% of burn injuries are intentional in the context of suicide and aggression. Suicide has an overall mortality rate of 65% worldwide, with flame and chemicals being the most frequent causal agents. Risk factors include psychiatric conditions, drug addictions, and gender violence. Children < 2 years are at greater risk of aggression, mainly by immersion in hot liquids and contact with cigarettes or hot objects. Total days of acute hospital stay approximately equals the burn size expressed as the percent of total body surface area (TBSA), except in the group with burns 50–80% TBSA where hospital stay increases. Fire/flame burns have the highest complication and mortality rates, followed by electrical injuries. Regardless of the cause, the maximal rate of complications occurs in infants and the elderly and increases progressively with age. Associated inhalation injury increases mortality, though it is less evident for burns > 60% TBSA because these already bear a poor prognosis. Although most burn injuries are not fatal, those who survive do so with varying functional and aesthetic sequelae, which may cause psychological distress and generate a cascade of personal, family, social, and labor repercussions. Finally, prevention through strategies like regulation of electrical systems, smoke detectors, temperature limiters in running water heaters, and use of fireproof clothes and construction materials have proven effective in reducing morbidity, mortality, and the economic burden of burns in developed countries. Remember Burns mainly affect the poorest and the most vulnerable people. Temperature is a measurement of the average kinetic energy resulting from the random movement of molecules constituting a physical element. In theory, temperature can range from absolute zero (no molecular movement) to infinite. A rise in tissue temperature occurs when energy is transferred. Conceptually, the energy that originates from a thermal source is called heat, and the energy that originates from a nonthermal source is called work. Heat can be transferred by conduction, convection, or radiation, with the first two involving direct physical contact with the energy source. In conduction, the energy source remains static, as when one is touching an incandescent material or dipping a hand in a bowl of hot water. In convection, the contact is established with a fluid in motion as with running water or steam causing a continuous turnover of molecules at the source–tissue interface, which prevents the system from reaching thermal equilibrium. Radiation requires no contact and can be emitted by any physical element with temperature other than absolute zero in the form of electromagnetic waves (0.1–100 μm). Examples include sunlight and infrared lamps. The surface of living organisms behaves as a dark body that easily absorbs radiation. Work implies not only a physical force that causes displacement but also opposition forces that interfere with it. Friction is the opposition force involved in burns. Energy transferred as heat or generating friction increases random molecular movement in tissue at the interaction point, elevating its temperature. The energy is then transmitted from the surface to the deep tissues by conduction. Biological tissues are poor conductors of heat; the less their water content, the poorer their conduction capacity. The effects of temperature in living tissues are conditioned by the value of maximum temperature reached and the length of exposure. When exposed to high temperatures, tissues undergo several changes in their physical properties, including tissue dilation, increased pressure, and decreased electrical resistance. In addition, biological effects are possible ( Moderately high temperatures have beneficial effects and are used as thermotherapy in physical rehabilitation within a narrow temperature range (40–45°C) for short periods of time (5–30 minutes). Beyond that range injury becomes a possibility. Due to skin’s resilience to temperature increase and its poor conductivity, it takes a considerable amount of time both to heat it up and to cool it down, which is why burn management requires not only the re moval of the energy source but also cooling down the skin surface to prevent progression of injury. Table 18.1 Biological effects of temperature on living tissues
18.1 Introduction
18.2 Epidemiology

18.3 Thermal Injury
18.3.1 Basic Science
![]() Table 18.1).
Table 18.1).
Temperature (°C) | Biological effects |
40–45 | Analgesic, anti-inflammatory, antispasmodic, sedative Improves elongation of collagen fibers |
45–60 | Pain Protein denaturation |
60 | Protein coagulation and cell death |
100 | Tissue vaporization and thermal ablation |
200 | Tissue carbonization |
300 | Tissue fusion (solid to liquid physical state) |
The first signs of cellular injury begin to appear at temperatures > 45°C when proteins and nucleic acids denature, leading to metabolic and structural dysfunction. The most remarkable histological feature is cell edema due to failure of the sodium-potassium adenosine triphosphatase (Na+/K+-ATPase) pump. Denaturation may be slowly reversed by cooling down. With temperatures > 60 °C, proteins and nucleic acids precipitate and cells die. It is an irreversible phenomenon whose histological expression is the coagulative necrosis. Macroscopically, tissues appear desiccated and mummified with a yellow-gray or blackish hue (eschar tissue), whereas microscopically the original histological architecture remains identifiable. Burns destroy skin and its appendages, dermal vascular plexus, and sensitive cutaneous nerves impairing its protective function as a physical and biological barrier, as well as its other functions, such as thermoregulation, synthesis of vitamin D, and sensation, all of which are essential for our adaptation to the external environment and social interaction. Cell destruction releases electrolytes, enzymes, and other cytoplasmic proteins that serve as injury markers (K+, myoglobin, creatine phosphokinase [CPK], L-lactate dehydrogenase).
18.3.2 Histological Zones of Thermal Injury
Jackson identified three zones of thermal injury: coagu lation, stasis, and hyperemia. In the coagulation zone, injury is maximal and irreversible, featuring coagulative necrosis. The stasis zone surrounds the area of coagulation and is characterized by protein denaturation, cell dysfunction, and blood stasis. The outermost is the hyperemia zone, which shows minimal cell injury and intense local vasodilation. It is important to note that final extension of the necrosis zone depends on the evolution over time of the other two zones. Additional cell death can be explained by the onset of immediate autophagy and delayed cellular apoptosis as well as by the addition of factors that hinder healing in the areas of stasis and hyperemia, such as hypoxemia, deficient blood supply, interstitial edema, desiccation, and local infection.
Remember 
Coagulative necrosis is the histological lesion of a thermal injury.
18.3.3 Physiopathology
Local Changes
The repair of any wound, including burn wounds, comprises three successive and partially overlapping phases.
The inflammatory phase takes place during the first week and begins with the release of primary mediators of cellular origin (histamine, serotonin, platelet-activating factor, and arachidonic acid metabolites) and plasmatic origin (coagulation factors, complement and kynin pathways components). They cause changes in the local microcirculation with primary vasoconstriction followed by vasodilation, increased endothelial permeability with interstitial edema, circulatory stasis, and microthrombosis. These mediators also stimulate the homing of other inflammatory cells in charge of removing debris and releasing cytokines that modulate and amplify the inflammatory response as secondary mediators.
The proliferative phase starts approximately 4 days after injury and lasts 3 weeks. Key features of this phase include a high rate of collagen production by fibroblasts, formation of new blood vessels from preexisting ones (angiogenesis), and the start of epithelialization.
The remodeling phase starts at week 3 and lasts up to a year. During this phase equilibrium between collagen synthesis and breakdown is reached, the normal 4:1 ratio of collagen I to collagen III is restored, and the wound gradually regains its tensile strength to a maximum of 80% of unwounded skin.
Systemic Changes
When burn injuries involve > 20% TBSA, the inflammatory response mediated by cytokines becomes systemic and may last for several months.
Acute Phase
The most prominent features of the acute phase are the abrupt increase in endothelial and cell membrane permeability and cellular dysfunction. The increase in permeability causes a rapid shift of protein-rich fluid into the interstitial space and subsequent interstitial and cellular edema. As a response to the hypovolemic shock, peripheral and splanchnic vasoconstriction occurs to ensure perfusion of vital organs.
The origin of cellular dysfunction is multifactorial and not only explained by tissue hypoxia. There is a tendency toward hypothermia, and basal metabolism is depressed in the acute phase. In addition, there is low cardiac output secondary to a reduced preload and the negative effect of cytokines in heart contractility, with a characteristic poor response to vasoactive drugs (cardiogenic shock). Renal function is affected by reduced blood volume, and there is renal tubular dysfunction due to hypoperfusion and tubular obstruction by cell debris. Mesenteric hypoperfusion causes mucosal edema and paralytic ileus. Leukocytosis with neutrophilia is prominent due to intravascular displacement and depletion of bone marrow reserves. In addition, destruction of red blood cells within the cutaneous vascular plexus leads to anemia and coagulation. Coagulation is affected by the loss of coagulation factors to the interstitial space, direct platelet destruction by temperature, and consumption of both from intravascular thrombosis.
Remember 
The burn shock is primarily hypovolemic but also distributive and cardiogenic.
Subacute Phase (> 48–72 Hours)
Restoration of permeability follows a downwardsloping exponential curve. It is already evi dent at 8–12 hours and normalizes from 48 hours onward, allowing reversal of the hypovolemic shock and edema reabsorption with transient polyuria.
During this phase, the stress state from burn injury generates a nonspecific clinical picture known as the systemic inflammatory response syndrome (SIRS), which sets in motion a hypermetabolic, hyperdynamic, and inflammatory response.
The hypermetabolic response is aimed at generating enough energy to withstand the inflammatory response and cope with subsequent tissue repair. It correlates with burn size, doubling the basal metabolism with burns > 40% TBSA, and may take up to 2 years to return to preinjury values. Thyroid function is inhibited, and basal metabolism becomes regulated by stress response hormones (cortisol, catecholamines, and glucagon). Because the use of sugars and fats is partially blocked, proteins represent the primary source of energy in this phase. Although gluconeogenesis is stimulated and the release of insulin is increased, there is peripheral insulin resistance that limits cellular intake of glucose, leading to hyperglycemia. Fortunately, uptake of sugar by the central nervous system, red blood cells, and wound bed works independently of the action of insulin. Hyperinsulinism blocks ketogenesis from fatty acids, and hyperglycemia promotes their hepatic reesterification back into triglycerides. Because the synthesis of transport lipoproteins is also insufficient, triglycerides cannot return to the fatty tissue and thus remain in the liver (steatosis), producing hepatomegaly.
The generation of energy from protein breakdown has a severe impact, with skeletal muscle being the most affected tissue because of its high protein content. Additionally, there is a rearrangement of liver protein synthesis, with acute phase proteins taking over visceral ones. The net result is weight loss and reduction in lean body mass with weakened muscle (known as self-cannibalism), all of which compromise inflammatory response, wound healing, and growth of pediatric patients. Laboratory workup will show a low serum protein level, a negative nitrogen balance, increased blood and urine urea, elevated C-reactive protein, and reduction of protein synthesis markers (albumin, prealbumin, and transferrin).
In order to withstand the hypermetabolic response, a hyperdynamic state ensues, with in creased cardiac output, tachycardia, tachypnea, and peripheral vasodilation, the latter being more evident after the first week.
Although initially beneficial, a SIRS prolonged in time can overcome the compensatory mechanisms and cause multiple organ dysfunction syndrome (MODS) and death by exhaustion.
Remember 
The leading causes of burn mortality are renal failure in the acute phase and sepsis and MODS in the subacute phase.
18.3.4 Classification of Burns
Skin burns are classified into three degrees according to the injured histological layer (![]() Table 18.2 and
Table 18.2 and ![]() Fig. 18.1,
Fig. 18.1, ![]() Fig. 18.2,
Fig. 18.2, ![]() Fig. 18.3,
Fig. 18.3, ![]() Fig. 18.4,
Fig. 18.4, ![]() Fig. 18.5). The fourth degree involves subcutaneous and deeper injuries.
Fig. 18.5). The fourth degree involves subcutaneous and deeper injuries.
Given that energy transference is rarely homogeneous, different depths within the same lesion are frequently found. Occasionally a gradient of injury is clearly recognized (![]() Fig. 18.6). On other occasions, a patchy geographic distribution may be seen.
Fig. 18.6). On other occasions, a patchy geographic distribution may be seen.
Finally, because the zone of necrosis can progress depending on the evolution of stasis and hyperemic zones, it may take several days for the lesion to fully demarcate and an accurate diagnosis to be made.
Remember 
Thermal damage is heterogeneous in its spatial distribution and can change over time due to necrosis progression into the stasis and hyperemic zones.
18.3.5 Inhalation Injury
Inhalation injury is the leading cause of death during a fire, and a significant worsening factor when associated with a burn injury.
Local effects of inhalation are irritant (physical stimulus of mechanical receptors by solid particles in suspension), thermal (hot gases that burn the mucosal layer), and, most important, toxic, which is dependent on the chemical nature of combustion products. Irritant and toxic effects can freely affect the entire airway, whereas burns rarely cause injury beyond the glottis because the upper airway absorbs most of the heat of inspired air. The reflex response is immediate and involves sneezing, mucous hypersecretion, cough with carbonaceous sputum, and laryngeal and bronchial spasms. The clinical features of mucosal injury present later following a typical temporal sequence and are secondary to inflammation, loss of cilia function and alveolar surfactant, and necrosis. Edema develops within the first hours after injury and may be silent or present with hoarseness, dysphonia, and glottis obstruction. ARDS and atelectasis usually appear on day 3–5, followed by lower airway infection after the first week.
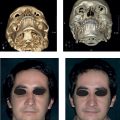
Inhalation injury should be ruled out in cases in which there is a history of fire exposure, especially when it occurs in a closed space and if the victim is found unconscious; in the presence of the clinical features just described; and in burns affecting the face, neck, nasal, and oropharynx mucosa, particularly those showing adhered carbonaceous particles (![]() Fig. 18.7).
Fig. 18.7).
Systemically, inhalation leads to hypoxia that can cause death in a few minutes. Hypoxia depends on oxygen consumption by the combustion and the eventual production of asphyxiant gases that interfere with cell respiration, namely carbon monoxide (CO) and hydrogen cyanide (HCN).
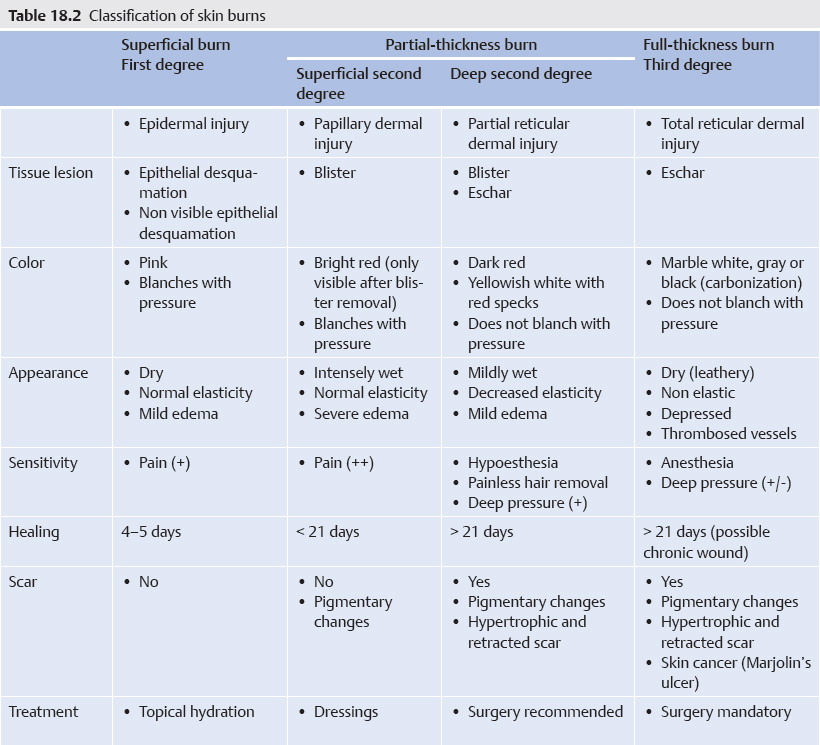

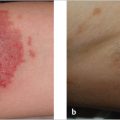
Fig. 18.1 First-degree burn (sunburn).


Fig. 18.3 Deep second-degree burn (flame).

Fig. 18.4 Third-degree burn (hot solid contact).

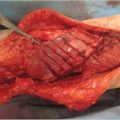
Fig. 18.5 Fourth-degree burn (flame).

Fig. 18.6 Flame burn on buttocks with a clearly identifiable gradient of injury.

Fig. 18.7 Flame burn on face with adhered carbonaceous particles around nostrils suggesting inhalation injury.
CO results from incomplete combustion of carbon-based compounds. It is a colorless, odorless, insipid, and nonirritating gas, all of which make its inhalation unnoticeable. It can be eliminated only by respiration and has a half-life of 3–4 hours when one is breathing ambient air. It competes with O2 for the heme groups in hemoglobin (whose affinity for CO is 240 times that of O2), myoglobin (whose affinity for CO is 40 times that of O2), and cytochrome C mitochondrial oxidase. It also shifts the hemoglobin (Hb) dissociation curve to the left, hindering the delivery of O2 to tissues. Clinical presentation is nonspecific and conditioned by hypoxia and a direct toxic effect of CO. It has been related to the levels of carboxyhemoglobin (COHb) (![]() Table 18.3). The first neurological sign is usually headache caused by vasodilation, followed by disorientation, irritability, weakness, as well as visual, hearing, and balance alterations, and ultimately obnubilation, seizures, and coma. CO depresses myocardial contractility (cardiogenic shock) and causes arrhythmias (the most common cause of death in CO intoxication). An acute coronary syndrome may develop from the combination of reduced perfusion and hypoxia. Respiratory features include dyspnea, tachypnea, Cheyne–Stokes breathing caused by lactic acidosis, ARDS, and pulmonary hemorrhage in severe cases. Skin may show a cherry red hue secondary to vasodilation and high O2 content of venous blood. Children usually present gastrointestinal symptoms, such as nausea, vomiting, and diarrhea. Surviving patients may experience a late-onset syndrome featuring neurologic, cognitive, and psychiatric alterations, which is why follow-up is recommended. Of note, in pregnant patients CO intoxication is always worse in the fetus than in the mother.
Table 18.3). The first neurological sign is usually headache caused by vasodilation, followed by disorientation, irritability, weakness, as well as visual, hearing, and balance alterations, and ultimately obnubilation, seizures, and coma. CO depresses myocardial contractility (cardiogenic shock) and causes arrhythmias (the most common cause of death in CO intoxication). An acute coronary syndrome may develop from the combination of reduced perfusion and hypoxia. Respiratory features include dyspnea, tachypnea, Cheyne–Stokes breathing caused by lactic acidosis, ARDS, and pulmonary hemorrhage in severe cases. Skin may show a cherry red hue secondary to vasodilation and high O2 content of venous blood. Children usually present gastrointestinal symptoms, such as nausea, vomiting, and diarrhea. Surviving patients may experience a late-onset syndrome featuring neurologic, cognitive, and psychiatric alterations, which is why follow-up is recommended. Of note, in pregnant patients CO intoxication is always worse in the fetus than in the mother.
Table 18.3 Clinical signs and symptoms related to carboxyhemoglobin levels
% COHb | Clinical finding |
< 10% | Asymptomatic |
10–20% | Headache, cutaneous vasodilatation, arterial hypotension Nausea and vomiting, especially in children |
20–30% | Dyspnea, tachycardia, acute coronary syndrome |
30–40% | Weakness, visual and hearing impairment, dizziness, drowsiness |
40–50% | Cardiogenic shock |
50–60% | Cheyne–Stokes breathing, seizures, coma |
> 60% | Cardiorespiratory arrest, death |
HCN in its pure state is a colorless liquid or gas. Its gaseous form is generated in large quantities by the combustion of nitrogen materials of domestic (plastic, wool, silk, polyurethane) or industrial origin. Its absorption is immediate and travels mainly bound to plasma proteins with a half-life of 4–8 hours. Most of it is cleared renally after being transformed into thiocyanide in the liver. HCN inhibits different metabolic pathways, such as the cytochrome C mitochondrial oxidase pathway. Its clinical features are also nonspecific, derived from cellular hypoxia, and include peripheral vasodilation, low blood pressure, and neurologic symptoms, such as headache, lethargy, and coma. Survivors may show permanent neurologic disabilities. The smell of sour almonds is noticeable in < 40% of patients.
Clinical Workup and Treatment of Inhalation Injury
Low values of oxygen saturation (SaO2) and oxygen partial pressure (pO2) are always present in severe cases of inhalation injury but their normal values do not rule out it. Among asphyxiant gases only CO diminishes the capacity of blood to transport O2 but the usual pulse oximeters do not differentiate between carboxyhemoglobin (COHb) and oxyhemoglobin (O2Hb), displaying a mistaken normal SaO2.
Direct visualization of the mucosa using indirect laryngoscopy and bronchoscopy helps to identify local airway injuries and confirm a diagnosis of inhalation; however, in cases of pure intoxication with asphyxiant gases, the airway might be normal. Chest X-ray is of little use initially and only shows positive signs within a few days once respiratory complications appear. Chest computed tomography, radionuclide imaging with 133-xenon, and pulmonary function testing are not routinely used.
Diagnosis of CO intoxication requires COHb > 10% (normal values are< 5% in nonsmokers and 5–10% in smokers); however, if enough time has elapsed or oxygen has been applied to favor CO clearance, normal values may be observed. HCN plasma levels can also be measured but this test is not readily available and is time consuming, making it of little value in common clinical practice. If an anoxic encephalopathy is suspected, a full neurologic assessment is mandatory, and as soon as the patient’s state allows, a cranial computed tomographic (CT) scan should be performed.
Treatment should be aggressive and start immediately at the slightest suspicion. Although management of inhalation injury is mainly symptomatic, specific therapies exist for asphyxiant gas intoxication.
If CO intoxication is suspected, administering 100% O2 reduces CO half-life to 80–100 minutes. In pregnant women O2 therapy should continue for a period of time after COHb normalization due to the different fetal pathophysiology. Hyperbaric O2 should be considered when COHb is > 20%, but its application in patients with severe burns is limited due to logistical difficulties.
When HCN intoxication is suspected, treatment should favor its metabolism. The first choice is intravenous hydroxycobalamin (70 mg/kg), which combines with HCN rending cyanocobalamin to be eliminated by secretions producing a reddish hue in the skin, mucosa, and urine for several days. Sodium thiosulfate (150 mg/kg) forms thiocyanide when combined with HCN, but it is a second choice because of its delayed onset of action. In severe cases, a slow perfusion of sodium nitrate (5 mg/kg) can be used, which generates methemoglobin (MHb) that binds to HCN to create cyano-MHb, favoring HCN transport to the liver for its final metabolism. Levels of MHb > 40% should be avoided in order to prevent further hypoxia.
18.3.6 Treatment
Every burned patient should be considered a trauma patient and treated accordingly until proven otherwise. The burn can be a distracting factor that diverts the attention from other coexisting injuries that might result to be more deleterious.
Prehospital Care
Primary Assessment and Intubation Criteria
Primary assessment must identify and treat immediate life-threatening injuries, following the ABCDE algorithm of the Advanced Trauma Life Support guidelines.
Airway: Burns can block airway due to edema and/or laryngeal spasm. Orotracheal intubation (OTI) should be performed whenever a patent upper airway cannot be secured.
Breathing: It may be impaired by burns restricting ventilation (deep circumferential burns affecting the thorax and abdomen) and by inhalation injury. As a general rule, high flow (15 L/min), 100% oxygen should be administered, ideally with a reservoir mask, to ensure maximum fraction of inspired oxygen. If intoxication by asphyxiant gases is suspected act accordingly. Failure to maintain respiratory function requires OTI and mechanical ventilation.
Prophylactic OTI use should be considered in cases where respiratory failure is foreseen (![]() Table 18.4). Its indication should be precise, weighing risks and benefits.
Table 18.4). Its indication should be precise, weighing risks and benefits.
Circulation: A good cardiocirculatory function must be ensured. All traumatic patients require immediate fluid resuscitation using 0.9% normal saline (NS) or Ringer’s lactate (RL). In stable patients, 500 mL of fluid (10 mL/kg in children) should be administered in 30 minutes, whereas unstable patients require a bolus of 1,000 mL (20 mL/kg in children) and reassessment according to response. Intoxication by asphyxiant gases should be suspected in hemodynamically unstable patients who do not respond to adequate fluid resuscitation. OTI should be performed in cases of refractory shock.
Table 18.4 Indications for orotracheal intubation
Absolute | Prophylactic |
• A (airway): a patent upper airway cannot be secured • B (breathing): acute respiratory insufficiency • C (circulation): refractory shock • D (disability): Glasgow Coma Scale score ≤ 8 | • Extensive facial and cervical burns (especially in children) • Suspected inhalation • Incipient signs of upper airway compromise: dysphonia, hoarseness, laryngeal stridor • Transport related limitations: delayed evacuation, long-distance transfer, limited health care resources, helicopter transportation |
Disability: A basic neurologic status assessment is performed including the Glasgow Coma Scale (GCS). Burn injuries rarely affect neurologic status, with the exception of asphyxiant gas intoxication. GCS ≤ 8 is an indication for OTI.
Exposure: All clothing and accessories should be removed. It allows primary assessment, eliminates any retained heat source, and prevents compartment syndrome as a consequence of subsequent edema. The patient should be covered immediately after to reduce the risk of hypothermia.
Secondary Assessment
Secondary assessment should be performed only on stable patients, with continuous monitoring of vital functions. The priority for unstable patients is their transport to a hospital facility.
Four questions characterize the accident: when (“hour 0”), what (the injurious agent), how (injury mechanisms and circumstances of the incident; accidental or intentional), and where (indoor or outdoor; domestic or work-related). A general physical examination must be performed quickly and in an orderly fashion from head to toe, always ruling out associated injuries. Physical examination of the burn injury should define its extent, location, and depth. The percentage of TBSA must not include first-degree injuries, because these are not considered when calculating fluid resuscitation. For extensive wounds, an approximate approach is Wallace’s “rule of nines”. In children percentages of head and lower legs must be adapted due to their different body proportions (![]() Fig. 18.8). Small extensions should be calculated using the patient’s hand and it is applicable for adults and children: the palm including all fingers represents approximately 1% TBSA. It is advisable to identify burns in areas of particular functional or aesthetic interest, such as the face (particularly the eyes), neck, breasts, genitals, perineal area, hands and feet, major joints and flexure areas, and nasal and oropharyngeal mucosa. Deep circumferential burns affecting the neck, trunk, extremities, and penis should also be ruled out.
Fig. 18.8). Small extensions should be calculated using the patient’s hand and it is applicable for adults and children: the palm including all fingers represents approximately 1% TBSA. It is advisable to identify burns in areas of particular functional or aesthetic interest, such as the face (particularly the eyes), neck, breasts, genitals, perineal area, hands and feet, major joints and flexure areas, and nasal and oropharyngeal mucosa. Deep circumferential burns affecting the neck, trunk, extremities, and penis should also be ruled out.
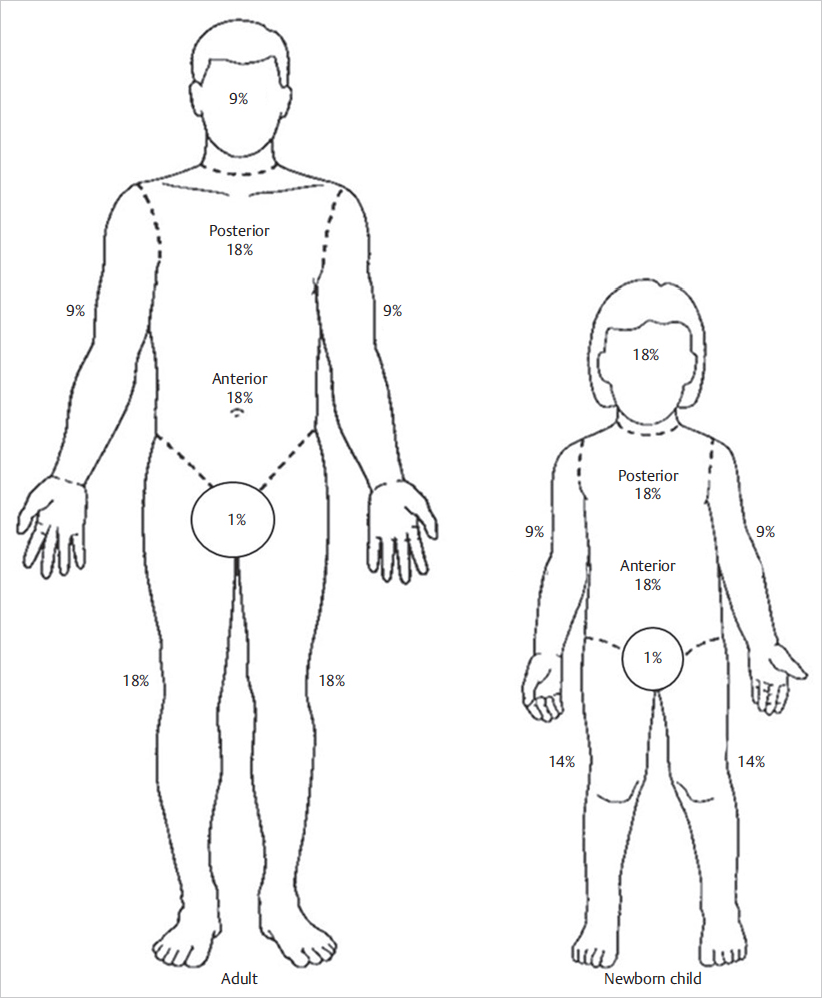
Fig. 18.8 The “rule of nines” for adults and children.
Initial Care
Burns should be cooled down by means of irrigation or immersion in tap water or 0.9% NS at room temperature (12–18°C) for 15–20 minutes, which also provides an analgesic effect, though it is discouraged for adult burns > 15% TBSA and for children burns due to the risk of hypothermia. An alternative is hydrogel dressings, which provide a refreshing sensation without increasing the risk of hypothermia. Debridement of blisters and applying wound dressing that might interfere with definitive hospital assessment should be postponed. Burns should be covered with sterile drapes or clean dry linen to avoid contamination and reduce painful stimuli. Finally the patient should be covered with a thermal blanket, keeping affected areas elevated.
Superficial second-degree burns are the most painful. Topical treatment provides some analgesic effects, but it is often insufficient and systemic analgesia is necessary. When conventional analgesia is inadequate, intravenous opioids are the treatment of choice.
A strict indication for nothing by mouth should be made before hospital admittance. If paralytic ileus is suspected, gastric decompression should be considered especially when the patient is to be transported by means of unpressurized air cabins (helicopter).
Early fluid resuscitation is indicated in adult burns > 15% TBSA and children burns > 10% TBSA. Multiple empirical formulas have been described to calculate fluid reposition (![]() Table 18.5), with Parkland’s being the most widely accepted. Children’s formulas are specific for them and their accuracy increases when body surface is used instead of weight, as Carvajal’s formula. RL is the fluid of choice because it is an isotonic crystalloid with an electrolyte composition similar to plasma, and contains lactate, which counteracts the initial shock’s metabolic acidosis. Hourly diuresis remains the single most useful indicator for tissue perfusion monitoring. The goal is 0.5 mL/kg/h in adults (1 mL/kg/h in children < 30 kg, and 2 mL/kg/h in lactants). Except in cases where rapid hospital arrival is secured, a permanent urinary catheter must be placed for precise quantification.
Table 18.5), with Parkland’s being the most widely accepted. Children’s formulas are specific for them and their accuracy increases when body surface is used instead of weight, as Carvajal’s formula. RL is the fluid of choice because it is an isotonic crystalloid with an electrolyte composition similar to plasma, and contains lactate, which counteracts the initial shock’s metabolic acidosis. Hourly diuresis remains the single most useful indicator for tissue perfusion monitoring. The goal is 0.5 mL/kg/h in adults (1 mL/kg/h in children < 30 kg, and 2 mL/kg/h in lactants). Except in cases where rapid hospital arrival is secured, a permanent urinary catheter must be placed for precise quantification.
Table 18.5 Fluid resuscitation formulas for adult burn patientsa
Name | First 24 hours | Next 24 hours |
Evansb | NS: 1 mL/kg/%TBSA burn C: 1 mL/kg/%TBSA burn D5W: 2,000 mL | NS: 0.5 mL/kg/% TBSA burn C: 0.5 mL/kg/%TBSA burn D5W: 2,000 mL |
Brookeb | RL: 1.5 mL/kg/%TBSA burn C: 0.5 mL/kg/%TBSA burn D5W: 2,000 mL | RL: 0.5 mL/kg/% TBSA burn C: 0.25 mL/kg/% TBSA burn D5W: 2,000 mL |
Parkland | RL: 4 mL/kg/%TBSA burn C: No D5W: No | RL: No C: 20–60% of estimated plasma volume D5W: to maintain diuresis |
Modified Brooke | RL: 2 mL/kg/%TBSA burn C: No D5W: No | RL: No C: 0.3–0.5mL/kg/%TBSA burn D5W: to maintain diuresis |
Modified Parkland | RL: 4 mL/kg/%TBSA burn C: No D5W: No | RL: No C: 0.3–1 mL Alb 5%/kg/%TBSA burn/16 per hour D5W: to maintain diuresis |
Abbreviations: Alb, human albumin; C, colloid solution; D5W, 5% dextrose in water; NS, 0.9% normal saline; RL, Ringer’s lactate; TBSA, total body surface area. | ||
Remember 
Resuscitation formulas are only an initial guide. The goal is 0.5 mL/kg/h in adult patients, that is, 30–50 mL/h (no more, no less).
Referral Criteria
Referral criteria are established based on burn injury categorization (![]() Table 18.6). Firstand su perficial second-degree burns < 5% TBSA, without affecting compromised areas or aggravating factors can be referred to primary care facilities and derived to a specialist only if healing is not achieved in a period of 15 days. Major burns, including burns > 15% TBSA (> 10% TBSA in children and elderly patients), third-degree burns ≥ 5% TBSA, and burns affecting compromised areas or with aggravating factors should always be referred to a hospital facility and the more complex ones taken directly to a burn care unit.
Table 18.6). Firstand su perficial second-degree burns < 5% TBSA, without affecting compromised areas or aggravating factors can be referred to primary care facilities and derived to a specialist only if healing is not achieved in a period of 15 days. Major burns, including burns > 15% TBSA (> 10% TBSA in children and elderly patients), third-degree burns ≥ 5% TBSA, and burns affecting compromised areas or with aggravating factors should always be referred to a hospital facility and the more complex ones taken directly to a burn care unit.
Table 18.6 Burn injury categorization
Burn severity | Aggravating factors |
• Extension (% TBSA) • Deep: ○ First-degree ○ Superficial second-degree ○ Deep second-degree ○ Third-degree • Location: ○ Uncompromised areas ○ Compromised areas | • Trauma related: ○ Inhalation injury ○ Other associated injuries ○ Suspected aggression • Patient related: ○ Illnesses prone to worsen with stress caused by burn injury ○ Pregnancy ○ Unfavorable social conditions |
Hospital Care
Initial Assessment
On arrival to the burn unit, the ABCDE algorithm is reassessed and continuing monitoring of vital signs is maintained. Intubation criteria should be reviewed and indirect laryngoscopy or bronchoscopy performed if airway injury is suspected.
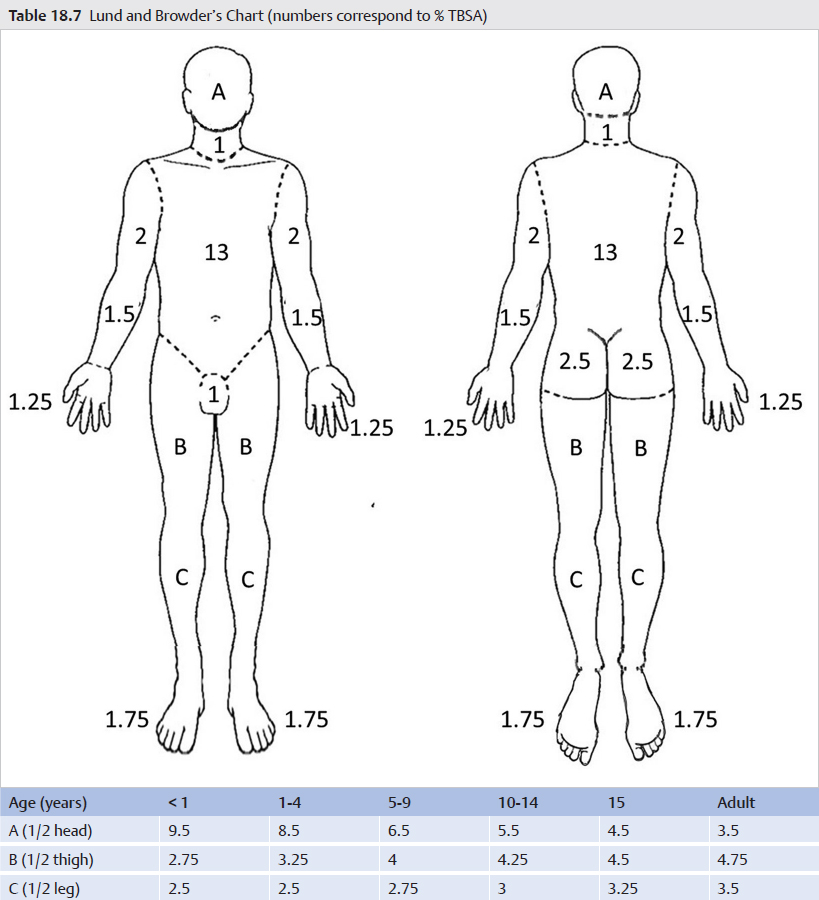
Burns are then washed with 0.9% NS and neutral soap or diluted chlorhexidine soapy solution, debriding all blisters, although small ones in painful areas such as the palms can be initially preserved. Location and depth of lesions is reassessed, and extension is calculated using the Lund and Browder’s chart (![]() Table 18.7).
Table 18.7).
A basic laboratory workup is done and additional tests added depending on each particular situation (![]() Table 18.8). As a general guideline, laboratory tests should be performed every 8 hours during the acute phase.
Table 18.8). As a general guideline, laboratory tests should be performed every 8 hours during the acute phase.
Escharotomy
This is the only urgent surgical treatment and is indicated in deep circumferential burns. There should be a low threshold to perform an escharotomy because the consequences of not doing so may be devastating. Because eschar tissue is insensitive, escharotomies may be performed in an emergency room without anesthesia with a scalpel, although using an electric cautery allows for improved hemostasis. The incision must run along the entire eschar and traverse its full depth up to unaffected underlying tissue (commonly subcutaneous).
Thoracoabdominal escharotomies are the only justifiable surgical therapy in prehospital care when ventilation is compromised. Thoracic escharotomy follows the anterior axillary lines to meet at the subcostal level (![]() Fig. 18.9), whereas abdominal escharotomy can be performed drawing a quadrant pattern (
Fig. 18.9), whereas abdominal escharotomy can be performed drawing a quadrant pattern (![]() Fig. 18.10). Neck escharotomy should follow the sternocleidomastoid muscle, avoiding the trachea and major blood vessels. Extremity escharotomies are done on the medial and lateral borders, avoiding superficial neurovascular structures, whereas on the dorsum of the hand they should follow intermetacarpal spaces, thus preserving the extensor tendons. Finger escharotomy must follow the dorsal and palmar skin juncture to preserve digital neurovascular bundles, with incisions ideally placed on the nondominant side (radial side on the thumb and fifth finger and cubital side on the others) (
Fig. 18.10). Neck escharotomy should follow the sternocleidomastoid muscle, avoiding the trachea and major blood vessels. Extremity escharotomies are done on the medial and lateral borders, avoiding superficial neurovascular structures, whereas on the dorsum of the hand they should follow intermetacarpal spaces, thus preserving the extensor tendons. Finger escharotomy must follow the dorsal and palmar skin juncture to preserve digital neurovascular bundles, with incisions ideally placed on the nondominant side (radial side on the thumb and fifth finger and cubital side on the others) (![]() Fig. 18.11).
Fig. 18.11).
Topical Treatment
The goal of topical agents is to maximize epithelialization and reduce bacterial colonization. Since its introduction in 1968, the most widely accepted topical treatment is 1% silver sulfadiazine, applied every 12–24 hours as a thick layer (2 mm). This hydrophobic cream keeps the wound bed moist; is painless and easy to apply; has wide antimicrobial action that includes gram-positive cocci, gram-negative bacilli, and fungi; but penetrates the eschar poorly. It adheres to the wound bed forming a whitish layer (pseudoeschar) that sloughs as the burn reepithelializes; however, it might impair proper assessment of burn depth. Leukopenia is a common finding in the first few days after its use, but it reverses spontaneously without having to halt treatment. Allergic reactions are infrequent. Its use in pregnant or lactating women and newborns is not advisable due to its sulfamide content. Deep burns benefit from adding cerium nitrate at 2.2% to 1% silver sulfadizine, which increases its bacteriostatic potency, dries and hardens the eschar, and allows for delay in the surgical treatment of unstable patients. Extensive descriptions of other topical treatments can be found in other texts. Finally, restrictive bandages must be avoided and the affected areas kept elevated.