7 Implants and Biomaterials Abstract Biomaterials are materials intended to be physically, chemically, and functionally compatible with the biological system where they are implanted. For centuries, medicine and science have tried to replace and improve body parts through the implantation of foreign materials, from gold, glass, or wood to modern ceramics or even biological implants, with varying degrees of success. Although the perfect biomaterial is yet to be developed, any product implanted in the human body should fulfill a list of criteria ranging from biocompatibility to being noncarcinogenic, and it should have a mechanical resistance that suits the part that is being replaced. We are witnessing remarkable developments and advances in the production of synthetic materials as well as biological matrices, and with this a growing body of alternatives for a range of reconstructive and aesthetic needs. Although completely artificial products are still the mainstay of biomaterials, the current trend is progressively shifting toward the development of tissue-engineered substitutes, whereby biological scaffolds are seeded with cells to promote tissue and organ (re)generation to achieve complex functional structures. Injectable substances form an important part of the biomaterial field. Resorbable and permanent materials have been and continue to be used frequently for reconstructive and aesthetic purposes; therefore a thorough understanding of their composition, indications, and potential complications is paramount to any plastic surgeon to ensure their correct and safe use. This chapter describes the different classes of biomaterials and implants and outlines the main factors affecting the outcome of implantation. Keywords: alloplastic, biomaterials, foreign body, implants, injectables, silicone Biomaterials and implants in modern times have a story, albeit a short one. Yet, in human history there have been many attempts to use synthetic materials to replace parts and functions of the human body. In fact, it is possible to go back to the Mayan civilization (500 BC) to find some examples of dental implants with seashells achieving some degree of bone integration. Moreover, basic suturing has been a well-assumed concept since the time of the early Egyptians. Sutures and dental replacements have been the two most investigated fields through the centuries. Despite the lack of knowledge about biology and materials, sutures were commonly used with a great deal of success for thousands of years. Regarding materials, gold, glass, and even wood were commonly used 2,000 years ago by the Roman, Chinese, and Aztec civilizations. In the last 2 centuries, invention of new materials (e.g., plastics) has given rise to many experiments, but given the lack of concepts of biocompatibility, the results were frustrating. Modern history spans the two world wars, when polymethyl methacrylate (PMMA), Dacron, nylon, polyethylene, and high-molecular-weight steel were used for the first time in vascular and orthopaedic surgery. The word biomaterial was introduced in the late 1960s and led to the formation of the Society for Biomaterials in 1975. Since then, not only pioneering physicians but also researchers in all scientific fields have been conducting experiments and investigations to explore new materials and their compatibility with the human body. This chapter describes the different classes of biomaterials and implants and their clinical application for successful implantation. By definition, a biomaterial is any material engineered to be physically, chemically, or functionally similar to a biological material made to interact with a biological system. The purely artificial materials can also be considered biomimetic materials. Biomaterials are usually classified as follows: • Autograft: living tissue derived from a host • Allograft: nonliving tissue derived from the same species (e.g., cadaveric tissues) • Xenograft: nonliving tissue from different species (e.g., porcine or bovine tissue) • Alloplast: synthetic material This chapter does not discuss autografts. Some of these characteristics, such as chemical and inflammatory responses, are relative features that may be modulated according to a specific need. Even the most biocompatible materials elicit a reaction from the host, which may eventually lead to implant failure or the development of a harmful, potentially lethal, outcome. Any biomaterial may thus trigger one or more of several responses, including inflammation and foreign body reaction, immunologic response, toxicity, thrombosis, cell migration, infection, and carcinogenesis. Inflammation, defined as the reaction of a vascularized living tissue to injury, is the basic response toward any implant. Depending on the time span of activity it can be acute or chronic and eventually lead to a variable degree of fibrosis and the formation of a fibrous capsule as a result of foreign body reaction and isolation. The biocompatibility of a certain material is usually defined by the lowest possible inflammatory response that is limited in time and does not become chronic. The immune response serves to protect the body from any agent (biological or synthetic) that is sensed as “nonself” and can be broadly divided into cellular and humoral. A humoral response with complement activation is largely involved in biomaterial reactions, with the complement mediating a local inflammatory response to the foreign body. When the cascade is abnormally activated, clinically relevant side effects ensue. Any material with low activation of the complement cascade is thus ideal for implantation. As a consequence of excessive inflammation due to artificial surface exposition, an imbalance between proand anticoagulation factors can occur at the site of implantation, leading to thrombus formation. Lastly, implanted foreign materials might produce malignant neoplasia through either a direct cellular stimulation or secondary to chronic inflammation. Most cancers induced by implants are late sarcomas with rapid and local growth adjacent to the implant itself, with large surface materials likely posing a greater likelihood to develop this kind of tumor. Conversely, resorbable materials represent a minor risk. In any case, the incidence and rarity of these lesions together with the improvement of materials knowledge render prosthetic materials worthy of use, with more benefits than real risks. Metals are among the materials most tolerated by the human body; thus they have been used for a long time, since the age of ancient Greece, long before modern research scientifically proved their safety. Alloys are composed of different metals or a metal and another element. Given their stiffness, biocompatibility, radiotransparency, and resistance to stress various alloys (chromium-cobalt, steel, titanium) are used for bone fixation, joint prostheses, or sutures and staples. Outside the field of plastic and reconstructive surgery, alloys are used in the fabrication of complex devices, such as pacemakers and stents. Stainless steel (an alloy of iron, molybdenum, nickel, silicone, manganese, and chromium) was developed at the beginning of 20th century and proved to be reliable and flexible but rigid enough for plate fixation. Steel was later substituted by Vitallium (an alloy of cobalt, chromium, and molybdenum), developed in 1932 by Albert W. Merrick for the Austenal Laboratories, for its resistance to corrosion compared to steel. The resistance to corrosion was a sign of great progress because metal’s erosion causes the release of toxic ions and possible mechanical failure, and it promotes inflammation. This alloy has also the rare feature of being compatible with magnetic resonance, though not to the same level as titanium. Gold and platinum are resistant to corrosion but have limited mechanical features. On the other hand, their high atomic number make them heavy enough to produce small heavy implants, such as those used for eyelid closure in facial palsy patients. In addition, their ability to osseointegrate makes metals a very good material for dental implants and prosthetic limbs. The structure of polymers, as the name itself indicates, is constituted of a theoretically endless chain of a certain repeated molecule, which can have variable molecular weights, from low to high, and different properties according to specific features ( The most popular of polymers, silicone, is a synthetic material made of repeating units of siloxane, which is formed by a chain of alternating silicon and oxygen atoms combined with carbon and/or hydrogen. First described by Kipping in 1904, the amazing chemical properties of silicone allows it to be used in various forms: fluid, emulsion, compound, resin, and elastomer. Silicone has a number of applications in medicine. In the 1940s, its hydrophobicity was employed to coat needles, syringes, and tubes to prevent coagulation of blood samples. The first published report of a silicone implant was in 1946, when Dr. Frank H. Lahey used a silicone elastomer for bile duct repair. Table 7.1 Polymer characteristics
7.1 Introduction
7.1.1 Basic Science
7.1.2 Body Reaction to Biomaterials
7.2 Materials
7.2.1 Metals
7.2.2 Polymers
![]() Table 7.1). In addition, depending on their porosity, polymers interact differently with the surrounding tissues, in fact, macroporous polymers allow incorporation and encapsulation while nonporous polymers do not allow such phenomena.
Table 7.1). In addition, depending on their porosity, polymers interact differently with the surrounding tissues, in fact, macroporous polymers allow incorporation and encapsulation while nonporous polymers do not allow such phenomena.
Silicone
Factors that influence polymer properties |
Chemical composition • Ester and amide links permit enzymatic degradation • Cross linking increases viscosity |
Length of chain • Short chain: liquid • Mid chain: gel • Long chain: elastomer/solid |
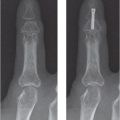
Examples of the use of silicone in hand surgery include the Swanson implants for metacarpophalangeal and interphalangeal joint arthroplasty and Silastic rods (Dow Corning) for tendon repair.
Liquid silicone has been used in the past for soft tissue augmentation, particularly in the field of cosmetic surgery; however, in 1992 the U.S. Food and Drug Administration banned this form of silicone for medical purposes, and its use should be condemned due to its severe adverse reactions, including inflammation, induration, discoloration, ulceration, migration, and granuloma formation.
In plastic surgery, silicone is widely used for manufacturing breast implants and other types of implants (e.g., gluteal, calf, pectoral). In 1962 Cornin and Gerow were the first to use silicone implants for breast reconstruction, and its use quickly expanded and popularized, in part due to the advantages of these implants compared to the foam-based implants available at that time. Initially, silicone implants were vacuum-molded, round-shaped implants with the anterior and posterior surfaces sealed together and a loop of Dacron mesh on the posterior aspect for fixation to the chest wall at the implantation site. Since their introduction, however, breast implants have undergone a number of changes. The first implants were made of liquid silicone encased within a silicone shell that frequently led to rupture and dispersion of silicone into the surrounding tissues. Implants are now made of cohesive silicone gel that has a consistency more similar to that of native breast tissue, with the important advantage that, if ruptured, the gel stays in place and no dissemination occurs. Cohesive silicone gel is used as filler for breast and gluteal implants, whereas the solid form is used for chin, malar, nasal, chest, and calf augmentation devices.
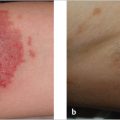
One of the most common complications associated with the use of implants for breast augmentation or reconstruction is capsular contracture, which refers to the thickening and contraction of the physiological fibrous layer of tissue that the body forms around the implant as part of the normal foreign-body reaction elicited by the device. The etiology of capsular contracture is multifactorial and not fully elucidated; nevertheless, in its most severe forms it can lead to breast deformation and pain (![]() Fig. 7.1), requiring implant removal/replacement and excision of the capsule (e.g., capsulectomy) (
Fig. 7.1), requiring implant removal/replacement and excision of the capsule (e.g., capsulectomy) (![]() Fig. 7.2). It is worth noting that some studies have shown a lower incidence of capsular contracture when using polyurethane-coated implants. Another important concern regarding the use of breast implants is the possible association with the development of anaplastic large cell lymphoma. Common clinical findings include delayed onset (e.g., > 12 months following implantation) of fluid collection, the presence of a mass, and pathological lymph nodes. Patients with suspected breast implant–associated anaplastic large cell lymphoma should be should be managed within multidisciplinary teams to allow early diagnosis and treatment, which is frequently based on removal of the implant and complete excision of the tumor, capsule, and affected lymph nodes.
Fig. 7.2). It is worth noting that some studies have shown a lower incidence of capsular contracture when using polyurethane-coated implants. Another important concern regarding the use of breast implants is the possible association with the development of anaplastic large cell lymphoma. Common clinical findings include delayed onset (e.g., > 12 months following implantation) of fluid collection, the presence of a mass, and pathological lymph nodes. Patients with suspected breast implant–associated anaplastic large cell lymphoma should be should be managed within multidisciplinary teams to allow early diagnosis and treatment, which is frequently based on removal of the implant and complete excision of the tumor, capsule, and affected lymph nodes.

Fig. 7.1 Bilateral capsular contracture (Baker IV) in a patient with a previous breast augmentation.
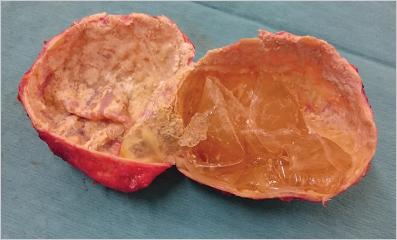
Fig. 7.2 Calcified capsules after removal. The wall was stone hard and required total excision.
Polyethylene
Polyethylene is a nonresorbable, synthetic, relatively inert low-molecular-weight molecule prepared in forms of increasing strength and stiffness according to its density. Its porous and woven forms allow fibrovascular ingrowth and certain integration with the tissues. At the same time, this feature renders removal of the implant more difficult. Common applications of polyethylene in plastic surgery include the use of Medpor (Porex Surgical) for facial implants and orbital floor support (with or without an associated titanium mesh) and Marlex (Bard Davol Inc) for chest wall reconstruction.
Polypropylene
This polymer is made of a carbon backbone and side chains of hydrogen and methyl groups. Widely known by its commercial name, Prolene (Ethicon), polypropylene is mainly used for the fabrication of mesh for hernia repair and nonresorbable sutures.
Polyesters
Polyesters are polymers that contain the ester functional group in their chain. Mersilene (Ethicon) is a polyester mesh used for abdominal herniorrhaphy as well as chest wall reconstruction; Dacron, another polyester is used for vascular grafts and suture material. Polyester prostheses reinforced with polyurethane (Xomed, Medtronic) are also used for craniofacial reconstruction. Aliphatic polyesters are used for the fabrication of several sutures, including polyglycolic acid (Dexon, Covidien), polyglactin 910 (Vicryl, Ethicon), poliglecaprone 25 (Monocryl, Ethicon), and polyglyconate (Maxon, Medtronic), among others.
Polytetrafluoroethylene
Polytetrafluoroethylene (PTFE) is also known as Teflon, whereas expanded polytetrafluoroethylene (ePTFE) is more commonly known by its commercial name Gore-Tex and is a nonresorbable, inert, nonadhesive, and nonporous polymer. ePTFE is used for a number of clinical applications, including abdominal wall mesh, facial augmentation implants, slings for facial paralysis, suture coating, and vascular grafts, among others. Gore-Tex temporomandibular joint implants were withdrawn from the U.S. market due to their high complication rates, including extrusion and infection.
Polymethyl Methacrylate
PMMA is a hard, noncolored, nonresorbable, inert resin commonly used to replace missing bone. It is made intraoperatively by mixing a liquid methylmethacrylate monomer with a powdered methylmethacrylate polymer to form the resin, which is easily malleable to the desired shape; however, it produces an exothermic reaction reaching up to 80°C that lasts for approximately 10 minutes; therefore surrounding bone and soft tissues need to be irrigated to avoid damage. PMMA is most frequently used for craniofacial reconstruction, and its porosity allows bony ingrowth and slow antibiotic release. Its use as a permanent soft tissue filler has been fraught with complications as explained later in this chapter.
Polyacrylamide
This polymer is formed by repeating units of acrylamide and is most commonly known by the commercial names Aquamid and Bio-Alcamid. They are permanent soft tissue fillers used for facial or body augmentation that have the ability to attract and retain a great amount of water, mimicking human soft tissue consistency. Nevertheless, their use has been seriously questioned due to foreign body reactions and extrusion problems, which may appear years after injection.
Polyurethane
Polyurethane is made by the combination of urethane/polyether segments with different consistencies. It has become popular as a coating for breast implants, with some studies suggesting a lower incidence of capsular contracture. Conversely, its use has raised concern about potential toxicity and carcinogenesis, although cancer associated with their use has yet to be demonstrated.
Note
Depending on porosity, polymers interact differently with the surrounding tissues, ranging from cellular and vascular ingrowth to no incorporation and encapsulation.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


