10 Laser Therapy: Principles and Applications in Skin Diseases Abstract The term laser is an acronym for light amplification by stimulated emission of radiation. Lasers deliver monochromatic, coherent, collimated, and high-intensity beams of light. In contrast, intense pulsed light devices are filtered flashlamps that emit polychromatic, noncoherent light in a broad range of wavelengths, being less powerful than lasers. The theory of selective photothermolysis, which states that the laser energy can be absorbed by a defined target chromophore, leading to its controlled destruction without significant damage to the surrounding tissue, is one of the most important concepts to understand why laser light can be used for targeted therapeutic purposes. Wavelength, pulse duration, energy density, chromophores of the skin (oxyhemoglobin, melanin, and water), fluence, irradiance, and spot size are laser parameters that influence clinical outcomes in the use of lasers for the treatment of different skin diseases, including vascular lesions, pigmentation disorders, melanocytic lesions, and skin resurfacing. These parameters have to be accurately taken into account for preventing undesirable effects, such as scarring, hypo-/hyperpigmentation, or alopecia. There are different modes of how laser light can be delivered: in a continuous wave (CW), such as the CW CO2 and older argon technology; quasi-CW, including the potassium-titanylphosphate, copper vapor, copper bromide, krypton, and argon-pumped tunable dye lasers; or a pulsed wave mode, such as long pulse-duration pulsed-dye laser and Q-switched ruby, alexandrite, or neodymium:yttrium-aluminum-garnet lasers (nanosecond pulse durations). The choice of laser should be made on the basis of the individual absorption characteristics of the target chromophore. Keywords: laser, selective photothermolysis, skin disorders, vascular, pigment, hair, resurfacing The term laser is an acronym for light amplification by stimulated emission of radiation. Laser light represents a part of the electromagnetic spectrum of energy and has several properties that are different from other light sources. Lasers deliver monochromatic, coherent, collimated, and high-intensity beams of light. In contrast to sunlight, which encompasses a wide spectrum of wavelengths, laser light is monochromatic, which means that it emits light of only one clearly defined single wavelength of a very narrow band of wavelengths. Laser light waves are in phase with respect to space and time (coherence). A laser beam has a defined narrow beam diameter with no divergence, which virtually does not increase even with increasing distance (collimation). Finally, these light sources can emit light with very high intensity. In contrast, intense pulsed light (IPL) devices are filtered flashlamps that emit polychromatic, noncoherent light in a broad range of wavelengths. Thus IPL devices are dimmer and less powerful than lasers. Most lasers used in dermatology generate light within the visible (400–760 nm), near-infrared (760–1400 nm), mid-infrared (1,400–3,000 nm), and infrared (> 3000 nm) range but rarely in the ultraviolet range (200–400 nm) of the electromagnetic spectrum. All laser systems are composed of the laser medium, the optical cavity, and a power source. The laser medium, which can be a solid (e.g., ruby, neodymium:yttrium-aluminum-garnet [Nd:YAG], or alexandrite), a liquid (e.g., dye), or a gas (e.g., argon, krypton, or carbon dioxide), determines the wavelength of the emitted light. The optical cavity, which contains the laser medium, serves as a resonator in which the laser process occurs. When laser light reaches the skin, it may interact with the tissue in four different ways: it can be absorbed, reflected, scattered, or transmitted. Only light that is absorbed will exert a detectable clinical effect. The amount of light that penetrates deeply into the skin is dependent upon light scattering and absorption by chromophores, which are the specific light-absorbing targets. The three main chromophores in the skin are melanin, (oxy)hemoglobin, and water. Tattoo ink is the main external chromophore of importance in laser dermatology. The amount of light that is absorbed by the specific chromophore depends on the wavelength used and whether it corresponds to the specific absorption spectrum of the respective chromophore. When choosing a laser for a certain indication, not only the absorption maximum of the target chromophore needs to be taken into account, but also the depth of penetration of the chosen laser wavelength in order to actually be able to reach the target within the tissue. The theory of selective photothermolysis, proposed by Anderson and Parrish in 1983, is one of the most important concepts to explain laser–tissue interactions and why laser light can be used for targeted therapeutic purposes. It states that the laser energy can be absorbed by a defined target chromophore, leading to its controlled destruction without significant damage to the surrounding tissue. To achieve this, a number of principles concerning wavelength, pulse duration, energy density, and chromophores of the skin need to be applied. The wavelength of the laser light needs to correspond to the absorption maximum or lie within the absorption spectrum of the respective target chromophore. Moreover, it should be of sufficient length to penetrate to the depth of the target. The pulse duration (PD) of the laser heavily affects the likelihood of achieving the desired clinical effect. The PD of the laser beam must be equal to or shorter than the thermal relaxation time (TRT) of the target chromophore. TRT is defined as the time required for 90% of an object to cool to 50% of the temperature achieved immediately after the laser exposure without conducting heat to the surrounding tissue. The TRT is heavily influenced by the size of the target. Large objects lose heat much more slowly than small objects. Different blood vessels have different TRTs: capillaries have a TRT of tens of microseconds, port-wine stain (PWS) venules have a TRT of tens of milliseconds, and leg veins of hundreds of milliseconds ( Table 10.1 Thermal relaxation times of important laser targets
10.1 Introduction
10.2 Basic Science
10.2.1 Laser–skin Interactions
10.2.2 Selective Photothermolysis
Wavelength
Pulse Duration
![]() Table 10.1). Small pigmented targets (e.g., melanosomes within pigmented melanocytes in a nevus of Ota) are best treated with short (submicrosecond) pulses, whereas larger pigmented targets (e.g., hair follicles) have longer TRTs and are best treated with longer (millisecond) pulses.
Table 10.1). Small pigmented targets (e.g., melanosomes within pigmented melanocytes in a nevus of Ota) are best treated with short (submicrosecond) pulses, whereas larger pigmented targets (e.g., hair follicles) have longer TRTs and are best treated with longer (millisecond) pulses.
Structure | Size (µm) | TRT (approx.) |
Tattoo ink particle | 0.5–4 | 10 ns |
Melanosome | 0.5–1 | 250 ns |
Blood vessels | 50 | 1 ms |
100 | 5 ms | |
200 | 20 ms | |
Hair follicle | 200 | 10–100 ms |
If a structure is heated for a period equal to or shorter than its relaxation time, the resultant damage is confined to the target object alone, reducing the risk of scarring. Conversely, if an object is heated for longer than its thermal relaxation time, thermal diffusion leads to heating of surrounding structures.
Note
If a structure is heated for a period equal to or shorter than its relaxation time, the resultant damage is confined to the target object alone, reducing the risk of scarring.
Energy Density
The energy density delivered by the laser beam, also referred to as fluence, must be high enough to actually destroy the target chromophore within the defined pulse duration but should also be at a level that minimizes collateral tissue damage. Energy density is measured in joules per centimeter squared (J/cm2).
Chromophores of the Skin
The three main endogenous chromophores in the skin are melanin, hemoglobin, and water. Each of these chromophores has its own absorption spectrum and absorption peak.
Water shows increasing absorption, starting at mid-infrared and increasing toward the infrared portion of the electromagnetic spectrum.
10.3 Therapeutic Parameters
Wavelength and pulse duration are the most important laser settings that govern the effects of laser light on skin. Fluence, irradiance, and spot size are additional laser parameters that influence clinical outcomes.
10.3.1 Fluence
Fluence is a measurement of the amount of light energy delivered per unit area. For most pulsed lasers used to treat vascular lesions, the fluences range from 3 to 15 J/cm2. For IPL in vascular lesions, higher fluences are required, ranging from 15 to 30 J/cm2. The destruction of very large structures, such as hair follicles, requires high fluences (20–50 J/cm2) due to the amount of tissue that has to be heated. The 1,064 nm Nd:YAG laser in vascular lesions also requires the use of high fluences (> 100 J/cm2). The target chromophore in telangiectasias (oxyhemoglobin) has low affinity for this wavelength, and delivery of high amounts of energy is necessary to heat the target tissue.
10.3.2 Spot Size
Spot size is the diameter of the beam of light emitted from the laser that hits the skin. In general, the depth of penetration of laser energy increases with wavelength until the mid-infrared region of the electromagnetic spectrum. Scattering of light occurs to a greater degree with small spot sizes. Thus the energy that enters the target tissue is attenuated far more rapidly with the use of small spot sizes than with the use of large spot sizes. Spot size is most important when targeting structures in the mid to deep dermis with long pulsed lasers. For targets in the epidermis or upper dermis, spot size is less important.
10.3.3 Other Considerations
Skin Cooling
Epidermal melanin is an undesired chromophore when treating dermal targets. Excessive heating of the epidermis can lead to epidermal damage, resulting in hypopigmentation or hyperpigmentation. Epidermal damage can be minimized through the use of skin cooling, and this is especially important with darkly pigmented skin. There are three basic types of skin cooling: precooling, parallel cooling, and postcooling, which correspond to extracting heat from the skin before, during, and after the laser exposure, respectively.
All cooling methods extract heat at the skin surface via a cooling agent (gas, liquid, or solid). For spray cooling, a cold liquid is used (e.g., liquid fluorocarbon is sprayed on the skin). Solid contact cooling often consists of a cold sapphire window held against the skin, through which laser or IPL energy is delivered.
Safety
Laser safety is a significant concern for the patient, physician, and clinical staff. Eye injuries and blindness may occur rapidly and painlessly. Blindness can occur even if only 1% of the beam is reflected into the eye from shiny metal, glass, or plastic surfaces. The highest risk occurs with near-infrared Q-switched lasers. Lasers and IPL sources used for hair removal can target the retina and uveal tract. Anterior eye injury from lasers or IPL sources usually occurs with treatment of the lower eyebrow or vascular lesions near the eye (without an eye shield properly in place). An opaque laser eye shield covering the patient’s cornea will not prevent damage if the laser or IPL directly impacts exposed sclera. Long-pulse, near-infrared laser light can penetrate through the eyelid and damage the eye. Proper use of laser-protective eyewear (including eye shields) is mandatory in laser surgery. Wraparound glasses and goggles are rated by optical density (OD) at specific wavelengths. For dermatological lasers, proper protection is an OD ≥ 4 at the wavelength of the laser being used. Color of the goggles is not an indicator of level of protection.
Fire and explosions may occur when lasers are in use. Drapes, clothing, dry hair, and plastic materials, including endotracheal tubes, can be ignited, especially when oxygen is in use. The greatest risk is with the CO2 and erbium:YAG lasers used for skin resurfacing and ablative fractional treatments. To prevent fire, it is highly recommended that any hair near the treatment field be moistened and makeup removed when one is working around eyelids. Alcohol, acetone, or other flammable skin-cleaning solutions must be allowed to completely dry before laser use. Intraoperative oxygen concentration should be reduced to < 40%. A fire extinguisher and water should be readily available.
Laser-generated “plume materials” may be inhaled, particularly with resurfacing or vaporization of hair during its removal. To avoid laser plume biohazards smoke evacuators and good ventilation are the most effective measures. Submicrometer surgical filter masks provide some protection when worn properly.
10.4 Types of Laser
Laser light can be delivered by either a continuous wave or a pulsed wave. The continuous-wave (CW) light is emitted over an uninterrupted period of time with a constant beam of light. CW lasers, such as the CW CO2 and older argon technology, emit a constant beam of light with long exposure durations that can result in nonselective tissue injury.
Quasi-CW mode lasers, including the potassium-titanyl-phosphate (KTP), copper vapor, copper bromide, krypton, and argon-pumped tunable dye lasers, shutter the CW beam into short segments, producing interrupted emissions of constant laser energy. These lasers may be associated with higher incidences of hypertrophic scarring and textural changes.
Truly pulsed lasers can be either very short pulsed, with nanosecond pulse durations (as in Q-switched ruby, alexandrite, or Nd:YAG lasers), or long pulsed, with pulse durations within the millisecond range (e.g., the pulsed-dye laser [PDL]). The short pulse durations limit the thermal spread of the heat and therefore decrease the likelihood of scarring.
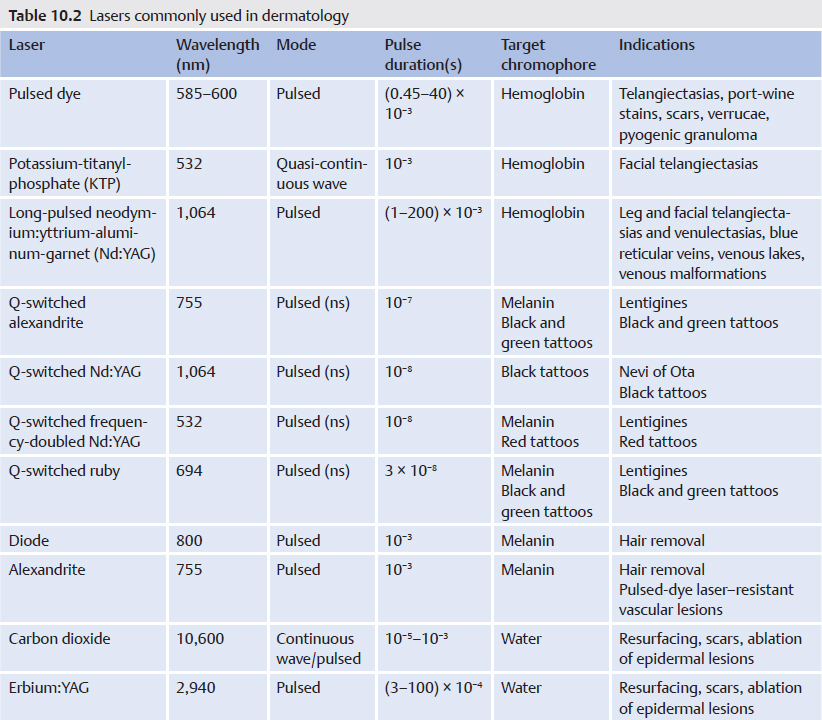
Because cutaneous lasers have different clinical applications related to their specific wavelengths and pulse durations, the choice of laser should be made on the basis of the individual absorption characteristics of the target chromophore (![]() Table 10.2).
Table 10.2).
10.5 Clinical Applications
The following section describes the use of lasers for the treatment of different skin diseases, including vascular lesions, pigmentation disorders, melanocytic lesions, and skin resurfacing.
10.5.1 Vascular Lesions
Oxyhemoglobin is the target chromophore in vascular lesions, and its absorption peaks are found at wavelengths 418, 512, and 577 nm, which corresponds to the yellow area of the electromagnetic spectrum. For this reason the lasers most frequently used in the treatment of vascular lesions, although not the only ones, are the KTP (532 nm), the PDL (577–600 nm), and the Nd:YAG (1,064 nm) lasers. Other lasers that can be used include the argon-pumped tunable dye laser (577, 585 nm), the copper bromide vapor laser (578 nm), and the krypton laser (568 nm). When one is treating vascular lesions, consideration should be given to the fact that, because melanin has a wider absorption spectrum that includes visible and infrared light, at these wavelengths absorption also occurs by epidermal melanocytes and, in general, by the whole epidermis, with the subsequent risk of hypopigmentation and scarring. The depth and thickness of the type of blood vessel targeted, as well as the patient’s skin phototype, are therefore important factors to take into account in the treatment of vascular lesions.
Port-Wine Stains
PWSs are a type of vascular malformation affecting 3 of every 100 newborns and are present at birth. Normally they present as pale pink macules or spots, which may occur singly or multiply at any anatomical site, although they are more common on the head and neck. They may have psychological and social consequences, which in some cases makes early treatment in childhood advisable. Depending on their location they may be associated with certain syndromes with systemic involvement (e.g., Sturge–Weber’s syndrome when their distribution follows the ophthalmic division of the trigeminal nerve or Klippel–Trénaunay–Weber’s syndrome when they are located in the extremities and accompanied by soft tissue hypertrophy and venous malformations).
It is essential to differentiate PWSs from nevus simplex or salmon patches, also known as flammeus neonatorum, angel’s kisses, or stork bites, which are pink macules or spots that characteristically fade during the first year of life in 50% of patients.
The size and location of the lesion determine the response to the laser treatment. Thus lesions located on the distal part of extremities and the centrofacial region (the area innervated by the second branch of the trigeminal nerve: the medial area of the cheeks, the lower eyelid, nose, and upper lip) usually respond worse to treatment than those located on the periphery of the face (in descending order: forehead, upper eyelid, lateral malar region, or jaw) and the neck. In addition, the earlier the treatment is performed, the better the response, even at ages of less than 6 months. As for the characteristics of the vessels, lesions with deep vessels with thicker walls show a poorer response to treatment. In contrast, the greater the extent of the lesion, the better the response to the laser will be. In any case, treatment of PWSs requires multiple sessions (after 8–10 sessions a lightening of 80% or more is achieved).
Most PWSs are superficial, with the vessels located at a mean depth of 0.46 mm. Two patterns of PWS located on the extremities can be defined: the better-defined geographic pattern (![]() Fig. 10.1) and the blotchy pattern with less well defined edges. The former are at greater risk of becoming hypertrophic, thick, darker, and deeper and are sometimes associated with soft tissue hypertrophy and lymphatic malformations. In such cases, in order to increase laser penetration, larger spot sizes should be used together with greater fluences and wavelengths. The PDL was created specifically for this disorder and initially emitted light at a wavelength of 577 nm. Currently, the pulsed-color laser, which uses the liquid medium rhodamine, emits short pulses of light flashes with a wavelength between 585 and 595 nm. Although this reduces absorption by the chromophore, penetrance is greater, which in turn makes it more effective in the treatment of PWSs. Many authors recommend using fluences of between 4 and 15 J/cm2, with spot sizes of between 7 and 12 mm. The ideal situation would be to begin with fluences of 5 or 5.5 J/cm2 and a spot size of 7 mm and to gradually increase these by 0.5 J/cm2 at each subsequent treatment session at intervals of 3 or 4 months.
Fig. 10.1) and the blotchy pattern with less well defined edges. The former are at greater risk of becoming hypertrophic, thick, darker, and deeper and are sometimes associated with soft tissue hypertrophy and lymphatic malformations. In such cases, in order to increase laser penetration, larger spot sizes should be used together with greater fluences and wavelengths. The PDL was created specifically for this disorder and initially emitted light at a wavelength of 577 nm. Currently, the pulsed-color laser, which uses the liquid medium rhodamine, emits short pulses of light flashes with a wavelength between 585 and 595 nm. Although this reduces absorption by the chromophore, penetrance is greater, which in turn makes it more effective in the treatment of PWSs. Many authors recommend using fluences of between 4 and 15 J/cm2, with spot sizes of between 7 and 12 mm. The ideal situation would be to begin with fluences of 5 or 5.5 J/cm2 and a spot size of 7 mm and to gradually increase these by 0.5 J/cm2 at each subsequent treatment session at intervals of 3 or 4 months.
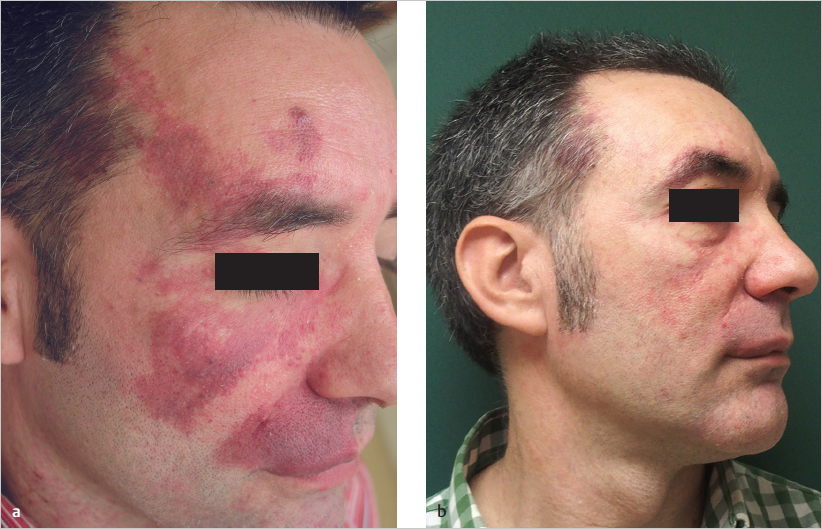
Fig. 10.1 (a) A 39-year-old man with a port-wine stain on the right hemiface. (b) Result after 12 sessions with a pulsed-dye laser.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


