12 Basic Surgical Techniques, Sutures, and Wound Closure Abstract Learning the principles and mastering the techniques of wound closure and suturing are essential to every surgical trainee, regardless of specialty. A good resultant scar begins with a properly designed incision, gentle and atraumatic handling of tissues, selection of the appropriate closure material, and correct reapproximation of the edges. The outcome of wound closure (i.e., the scar) is influenced by a number of factors, including location, shape, orientation, tension, contamination, patient-related factors, and surgical technique. Unfortunately, no matter how meticulous we are, poor scarring sometimes develops and must be addressed by various nonsurgical and surgical methods. In this regard, it is important to consider the amount of time since wounding and to set realistic goals with the patient. Scar revision is usually performed on fully or near-fully matured scars in order to optimize the benefits of the procedure. Scars needing intervention are usually managed conservatively for a period of 6–12 months, after which surgical treatments are available. This chapter describes the basic aspects of wound suturing as they relate to suturing material and basic techniques. Different methods of scar revision are also discussed. Keywords: needles, scar revision, scarring, suture, wound closure Plastic surgery is a broad and varied surgical specialty. Because plastic surgeons deal mainly with the repair and rearrangement of soft tissues, most of our procedures leave behind a mark, most commonly in the form of a scar, which is subject to scrutiny and judgment from patients and colleagues. Furthermore, an important part of our practice is correcting unpleasant “marks” left after another procedure (plastic or not). Additionally, not infrequently, patients with lacerations or who are to be operated by other surgical specialists, ask to be sutured by a plastic surgeon with the wish to obtain as fine a scar as possible. Excepting the unreasonably demanding ones, these patients are right to some extent in that, unlike other surgical specialties, an ongoing aspect of a plastic surgeon’s training is actually learning to achieve inconspicuous scars by identifying and managing all factors that may potentially affect wound healing and the final appearance of the resulting scar. Of all such factors, the one the surgeon has most (if not complete) control of is the surgical technique. This chapter describes the principles of wound closure, suturing techniques, and scar revision. Selection of the correct suture material is an important factor for the overall success of wound closure, regardless of its complexity. Unfortunately, however, proper education about and familiarization with the products available for tissue closure have fallen almost into oblivion in some areas and subspecialties. The main task for any suture in any tissue is to hold the edges together in correct apposition until healing is established. The choice of material will then be influenced not only by the type of tissue but also by the local and systemic conditions as well as the distraction forces that may occur during the healing process. Sutures can be classified according to different parameters as will be described here. There are different possible combinations, and, although the choice is usually based on training and personal preferences, it is important to consider certain factors that can guide selection of the best material ( Sutures are classified as resorbable or nonresorbable depending on whether the organism will degrade it or not. Nonresorbable sutures do not undergo any processes of degradation; they remain in place indefinitely until they are removed. Resorbable sutures may be resorbed by either proteolysis or hydrolysis. In proteolysis, the suture is digested by an enzymatic process of foreign body reaction, which generates a localized inflammation at the site of the stitch. In hydrolysis, the suture is gradually absorbed by the penetration of fluids and is thus less inflammatory than proteolysis. Resorbable sutures have established degradation rates; nevertheless, certain factors, such as contamination/infection, fever, and poor nutritional status may accelerate their resorption and as such should be considered when selecting the most appropriate material. Likewise, in areas with high enzymatic content, such as the stomach or cervix, faster degradation of resorbable sutures is observed. Table 12.1 Factors influencing the selection of suture material
12.1 Introduction
12.2 Sutures
12.2.1 Classification of Sutures
![]() Table 12.1).
Table 12.1).
Resorbable/Nonresorbable
Type of tissue Anatomical area Presence of or potential for contamination Local inflammation Tension of closure Wound’s healing capacity Patient comorbidities, including wound-healing disorders |
Note
Resorbable Sutures
The local environment, presence of contamination, inflammation, fever, and an altered nutritional status may accelerate the rate of degradation of resorbable sutures.
Monofilament/Braided
According to their configuration, sutures are classified as monofilament or braided (also called multifilament). Monofilament sutures are composed of s single thread. Due to the little resistance that tissues offer to the passing of monofilaments, these sutures are ideal for delicate structures, such as vessels and nerves, though they are used in various other tissues as well. Furthermore, because of their single-thread configuration, monofilaments usually elicit less reaction from the tissues and have a low risk of infection in comparison to their braided counterparts. One of the main shortcomings of monofilaments is their high packing memory—defined as the tendency of a suture to retain the shape it had in its original envelope—which makes it a little harder to manipulate and requires more ties to secure the knot. Also, if improperly handled, monofilaments are more prone to developing cracks or weak spots, which could reduce their tensile strength.
Multifilament sutures consist of several strands braided together. Braided sutures have a higher friction coefficient and almost no memory, which facilitates their handling and increases knot security. Due to their multithread configuration, braided sutures have varying degrees of capillarity, defined as the ease with which fluids are wicked along the threads. Additionally, bacteria may home between the threads and spread into the wound site. This potential shortcoming needs to be considered when suturing wounds at risk of contamination or infection. In an attempt to lower such risk, some manufacturers have developed braided sutures coated with antibiotics; although their efficacy remains to be demonstrated. Another disadvantage of multifilaments is their “saw effect” as they pass through the tissues, which can be an issue when trying to close wounds with friable edges. Coating makes the suture less sharp and has been introduced by some manufacturers to reduce this effect.
Natural/Synthetic
Sutures may be of natural or synthetic origin. Natural threads include silk, linen, and collagen (more commonly known as catgut), the latter derived from either the serosal layer of beef (bovine) or the submucosal fibrous layer of sheep (ovine) intestines. Natural sutures were the first available in the market and continue to be used in a number of settings; however, they have some important disadvantages, including high capillarity, the generation of a sometimes strong inflammatory reaction, problems with tolerance, and loss of mechanical strength when wet. Synthetic materials on the other hand include the absorbable polyglycolic acid, polylactic acid, poliglecaprone 25, and polydioxanone as well as the nonabsorbables nylon, polyester, polyvinylidene fluoride (PVDF), and polypropylene. Synthetic sutures are more frequently used because they have overcome many of the shortcomings of natural sutures.
12.2.2 Tensile Strength
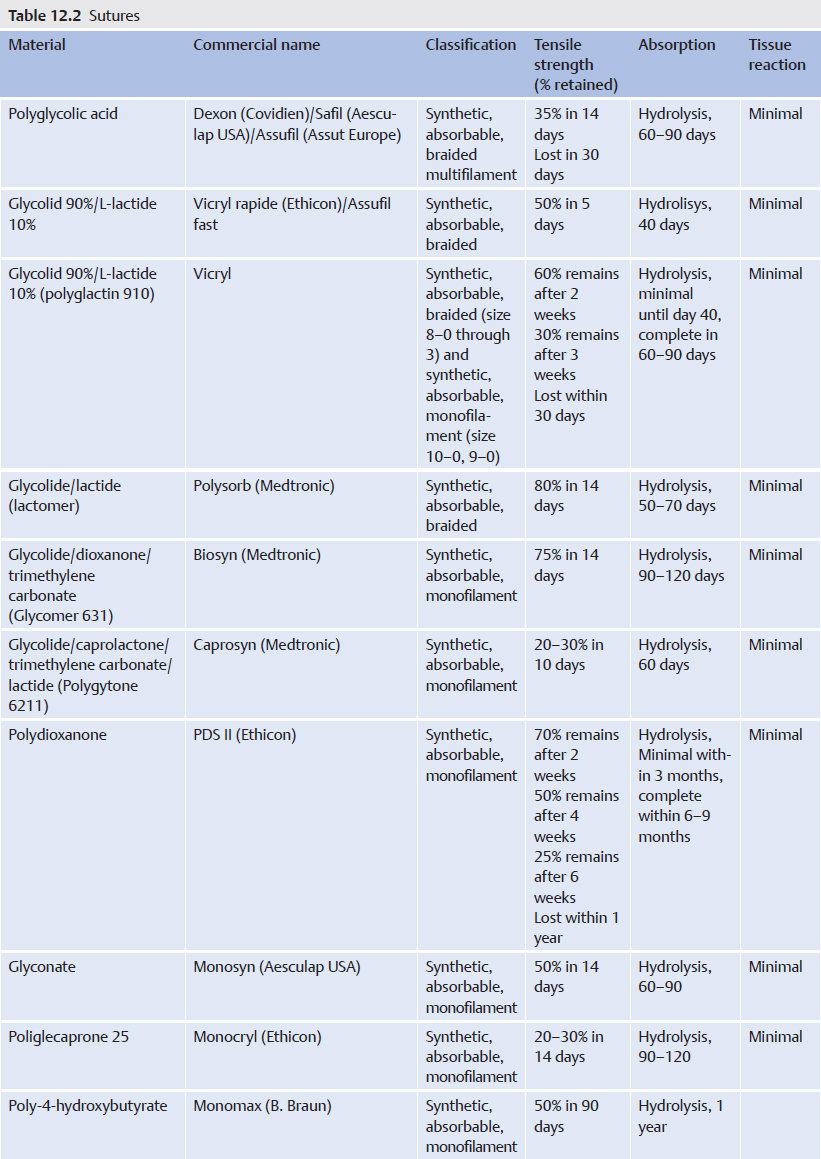
![]() Table 12.2 summarizes the main sutures available today with regard to their permanence, configuration, origin, absorption, and tensile strength.
Table 12.2 summarizes the main sutures available today with regard to their permanence, configuration, origin, absorption, and tensile strength.
12.2.3 Gauges and Needle
The diameter or gauge of a suture can be expressed in two ways: according to the United States Pharmacopeia (USP) or the European Pharmacopeia (EP), with the former being the most widely used, ranging from 12–0 to 10. Simply and briefly, the higher the number of zeros, the thinner the suture is (e.g., 5–0 is thinner than 3–0). Conversely, for whole-numbered gradings (e.g., 0, 1, 2, 3, and 4), the higher the number, the thicker the suture (e.g., a 3 suture is thicker than a 1 suture) (![]() Table 12.3).
Table 12.3).
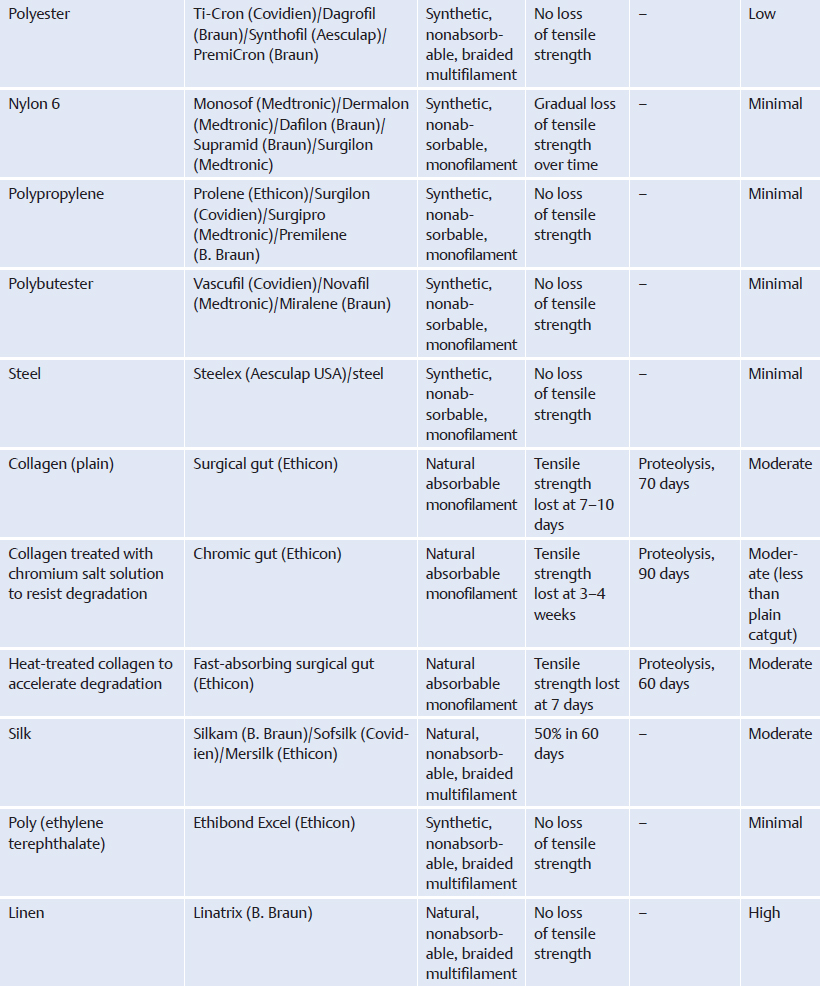
Regarding needles, most sutures come already armed in their packaging, meaning they are already attached to a needle. Some sutures are double-armed; they are armed with two needles, one at each end of the thread. Needles are made of stainless steel alloy, which allows, to a certain extent, bending without breaking. Even though there are different types of needles, they all share the same basic structure, which includes a point, a body, and an eye or attachment zone. Additionally, there are four basic measurements that define the structure of a needle, namely the arc (also called the needle length), chord length, radius, and diameter (![]() Fig. 12.1).
Fig. 12.1).
The needle’s attachment zone may be eyed or swaged. Eyed needles must be threaded manually, offering the advantage of using any combination of needle and thread; however, manual threading can be difficult and time consuming for thinner sutures and carries the inherent risk of puncture during manipulation. In addition, the protrusion of the thread at each side of the eye may cause drag and may damage the tissue as it passes through. Swaged needless, on the other hand, are eyeless and have the suture already incorporated to them so that the attachment zone is thinner than the body of the needle, thus eliminating drag. Finally, there are sutures with a needle insertion system that allows easy removal by pulling on the thread without having to cut it (control release needle, Ethicon).
The body of the needle usually represents the fraction of a circumference with the curvature ranging from 5/8 to 1/4 of a circle, although other shapes, such as straight, hook-shaped, progressive/asymptotic, and ski-shaped needles are available as well. Regardless of their shape and curvature, needles can have three basic configurations: round, triangular, and spatula. With round-bodied needles the tissues are spread around the needle rather than being cut by it, making round-bodied needles ideal for closure of fascia, tendon, peritoneum, or friable tissues, among others. Triangular needles are also called cutting needles due to the presence of a sharp edge that cuts through the tissues. Conventional cutting needles have the apex of the triangle (e.g., the sharp edge) on the inside of the needle, whereas in reverse cutting needles the cutting edge is on the exterior of the curve, making them preferable for skin closure. Additionally, the reverse cutting configuration increases needle strength and makes it more resistant to bending. Spatulated needles have extremely sharp edges, which cause minimal trauma to the sutured tissues and are used mainly in ophthalmic surgery and microsurgery.
USP | Thread gauge (mm) |
12–0 | 0.001–0.009 |
11–0 | 0.010–0.019 |
10–0 | 0.020–0.029 |
9–0 | 0.030–0.039 |
8–0 | 0.040–0.049 |
7–0 | 0.050–0.069 |
6–0 | 0.070–0.099 |
5–0 | 0.10–0.149 |
4–0 | 0.15–0.199 |
3–0 | 0.20–0.249 |
2–0 | 0.30–0.349 |
0 | 0.35–0.399 |
1 | 0.40–0.499 |
2 | 0.50–0.599 |
3+4 | 0.60–0.699 |
5 | 0.70–0.799 |
6 | 0.80–0.899 |
7 | 0.90–0.999 |
8 | 1.00–1.099 |
9 | 1.10–1.199 |
10 | 1.20–1.299 |
The point of the needle usually follows the shape of the body, except in tapered needles in which there is a sharp pointed tip but a blunt (round) body (![]() Fig. 12.2).
Fig. 12.2).
12.2.4 Tissue Adhesives
As their name implies, these are biological adhesives derived from cyanoacrylate that have the ability to polymerize in the presence of moisture. This produces an adherent resistant band between the edges of adhesive contact, which facilitates wound edge apposition and healing. Because they provide very little or no tensile strength, the use of tissue adhesives is mainly restricted to the epidermal approximation of tension-free superficial cutaneous wounds. For deeper wounds, an adhesive may be used provided that the subcutaneous and/or dermal planes have been securely approximated with the use of sutures. Some commercially available tissue adhesives are LiquiBand (Cardinal Health), Histoacryl (B. Braun), Dermabond (Ethicon), Indermil (Covidien), and Leukosan (BSN medical).
12.3 Wound Closure
Wound closure is one of the first skills taught to any medical student or surgical trainee. There are several factors that influence the final outcome of wound closure, namely orientation, shape, location, tension, presence or risk of contamination/infection, patient-related factors, and surgical technique.
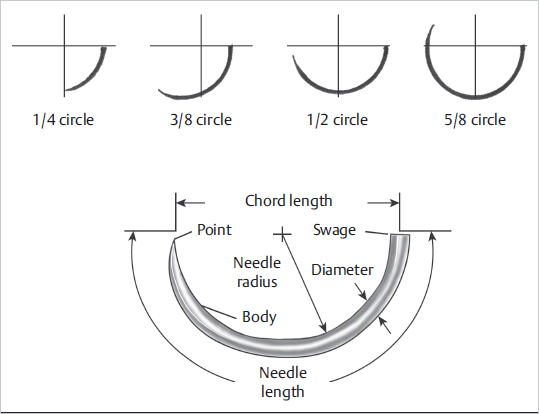
Fig. 12.1 Anatomy and curvature of a needle. (Reproduced from Janis, Essentials of Plastic Surgery, 2nd edition, ©2014, Thieme Publishers, New York.)
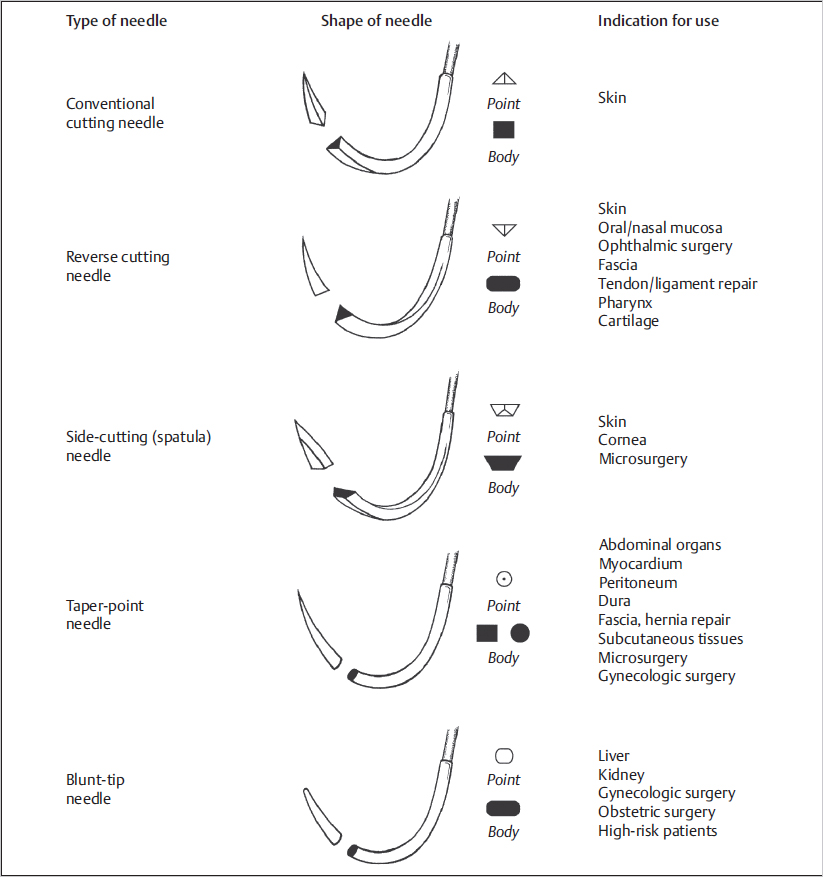
Fig. 12.2 Main configurations of suture needles. (Reproduced from Janis, Essentials of Plastic Surgery, 2nd edition, ©2014, Thieme Publishers, New York.)
12.3.1 Orientation
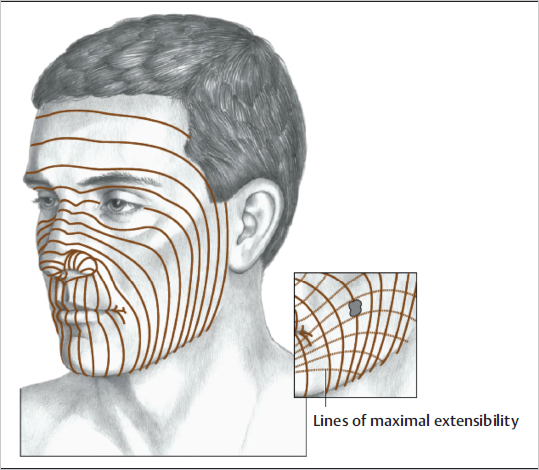
All incisions leave a scar, without exceptions. Scars cannot be erased; instead they can be strategically hidden or, if on exposed areas, positioned to make them as inconspicuous as possible. With time they may even become less noticeable, but they do not disappear. Thus an important factor determining a scar’s final aspect is orientation. During the 19th and 20th centuries several anatomists and surgeons studied the mechanical behavior of skin, some of them with a purely anatomical descriptive purpose and others with the aim of delivering a guide to placement of surgical incisions. That is how, not surprisingly, up to 36 different guidelines have been described. In 1962, Borges described the relaxed skin tension lines (RSTLs) as lines that follow the furrows formed when the skin is relaxed by pinching, muscle contraction, or joint mobility. These lines then became the main guideline for the placement of incisions, especially in the face. Perpendicular to RSTLs are the lines of maximal extensibility (LMEs), which, as the name suggests, indicate the direction at which skin has its greater mobility (![]() Fig. 12.3). It follows that, in order to obtain a scar as inconspicuous as possible, incisions should be made parallel to RSTLs and closed in the direction of LMEs. In addition, when planning facial incisions, the aesthetic units and subunits of this anatomical area should be considered (
Fig. 12.3). It follows that, in order to obtain a scar as inconspicuous as possible, incisions should be made parallel to RSTLs and closed in the direction of LMEs. In addition, when planning facial incisions, the aesthetic units and subunits of this anatomical area should be considered (![]() Fig. 12.4). When we look at someone’s face, we unconsciously expect a certain break at the margin between two different units. Hence, if the scar lies over such a line, it will be much less noticeable than if it lies within the unit. Moreover, in cases in which a block of tissue is excised, a better result is sometimes obtained by removing and replacing the whole subunit rather than a part of it, even if this involves removing healthy surrounding skin.
Fig. 12.4). When we look at someone’s face, we unconsciously expect a certain break at the margin between two different units. Hence, if the scar lies over such a line, it will be much less noticeable than if it lies within the unit. Moreover, in cases in which a block of tissue is excised, a better result is sometimes obtained by removing and replacing the whole subunit rather than a part of it, even if this involves removing healthy surrounding skin.
The orientation of surgical incisions (and resulting scars) is related not only to making them inconspicuous but also to avoiding any functional impairment. This concept is of utmost importance when planning incisions over joints or flexion creases. An incision must never cross perpendicularly over a joint or flexion crease because this might lead to contracture and restrict the joint’s range of movement. Instead, zigzag, such as a Brunner type in the hand, or S-shaped incisions, such as those used for axillary and inguinal lymph node dissection, should be used (![]() Fig. 12.5).
Fig. 12.5).
Note
Relaxed Skin Tension Lines
The relaxed skin tension lines described by Borges should not be confused with Langer’s lines. Karl Langer was an anatomist who studied the direction of ellipses formed after stabbing a roundtipped awl into hundreds of cadavers. Langer’s lines represent lines of tension (cleavage) and are different from RSTLs. In fact, in many areas, RSTLs and Langer’s lines lie perpendicular to one another.
12.3.2 Shape
Semicircular scars can sometimes lead to swelling and bulging of tissue on the concave side, producing a step-off commonly referred to as a trapdoor deformity. The possible mechanisms leading to this include wound contraction along the curvilinear margin and disruption of venous and lymphatic drainage. Pincushioning is a similar phenomenon, often seen in round-shaped flaps in which the flap becomes bulgy inside an apparently constricted scar halo. Although this may sometimes lead to an unsightly result, in some cases it can be used favorably to re-create dome-shaped structures in areas such as the nose.