Burns
Dominic C. Kim
Abel D. Jarell
I. BACKGROUND
In the United States, approximately 450,000 individuals are treated for thermal injuries yearly, of whom 5,000 are hospitalized, 25,000 are admitted to specialized burn centers, and 3,500 die. Scalding by hot objects or liquids is most often the mechanism of injury in children, accounting for nearly 80% of burns, whereas flame burns are the most common mechanisms overall, with adults accounting for the majority. In fact, according to the Center for Disease Control, unintentional burns in patients from <1 to 4 years old continue to be one of the leaders in nonfatal injuries treated in US emergency departments yearly. Other possible burn etiologies include contact, chemical, electrical, radiation, and intentional burns. Contact burns predominate in the pediatric population in the home setting, whereas chemical and electrical burns are mostly attributed to industrial and workplace mishaps in the adult sector.
Sustained cutaneous exposure to temperatures exceeding 40°C has been shown to denature proteins and compromise plasma membrane integrity, resulting in thermal burns. The resultant degree of cutaneous damage is directly related to the duration and intensity of heat exposure, the type of heat source, and the thickness of the exposed cutaneous surface. Further, duration and intensity of the heat source are synergistic—coagulation necrosis results from 45°C exposure for 3,600 seconds or a 60°C exposure for 10 seconds. Both structural malformations and synthesis of local mediators such as histamine, serotonin, bradykinin, nitric oxide, and oxygen-free radicals contribute to the physiologic effects inherent in burn pathology. In addition to local changes, more systemic effects may ensue, manifesting as shock, respiratory and renal failure, cardiac depression, immunodeficiency, and the entrance into a hypermetabolic state where nutritional support becomes critical.
Burn categories are based on depth and are traditionally categorized as first, second, or third degree. The depth of the burn is often related to its cause. Scalds from hot liquids are usually partial thickness, whereas injuries from contact with flames, hot metal, or electric current are usually full thickness. However, thermal injuries are a dynamic entity, with the depth of the burn evolving over time and peaking at about 3 days, a process known as conversion. Therefore, it is often difficult to ascertain the true depth of injury at the time of presentation, presenting clear clinical challenges.
II. CLINICAL PRESENTATION
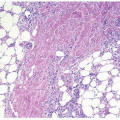
First-degree burns involve only the epidermis and typically resemble a sunburn. The lesions are usually erythematous, edematous, painful, and dry. Desquamation may occur after a few days. These lesions usually heal within 5 to 10 days with postinflammatory pigmentary alteration but without scarring unless secondarily infected. Seconddegree burns can be either superficial or deep. The former involves the entire epidermis and part of the underlying dermis, with patients displaying
blanchable erythema, edema, serous or hemorrhagic bullae, erosion, and exudation. The latter involves yet deeper layers of the dermis, with patients presenting with red to pale skin with serosanguineous or hemorrhagic bullae, erosions, and generally nonblanchable lesions. Superficial second-degree burns reepithelialize from adnexal structures (hair follicles) and, if left undisturbed, heal within 2 weeks without scarring. Deep second-degree burns often have damaged adnexal structures; healing rarely occurs within 3 weeks, with resultant scarring and contractures, especially in children. Third-degree burns involve the complete destruction of the epidermis and dermis, including the subcutaneous fat. The cutaneous surface may either assume a dry, firm, nonblanching, translucent appearance, often resembling parchment paper, or an anesthetic, charred, tan appearance with a leathery consistency. Such burns heal slowly, often over months, with hypertrophic scarring and contractures. First- and second-degree burns are generally painful, whereas destruction of the dermal plexus of nerves in third-degree burns renders the tissue insensitive to pain (Table 7-1).
blanchable erythema, edema, serous or hemorrhagic bullae, erosion, and exudation. The latter involves yet deeper layers of the dermis, with patients presenting with red to pale skin with serosanguineous or hemorrhagic bullae, erosions, and generally nonblanchable lesions. Superficial second-degree burns reepithelialize from adnexal structures (hair follicles) and, if left undisturbed, heal within 2 weeks without scarring. Deep second-degree burns often have damaged adnexal structures; healing rarely occurs within 3 weeks, with resultant scarring and contractures, especially in children. Third-degree burns involve the complete destruction of the epidermis and dermis, including the subcutaneous fat. The cutaneous surface may either assume a dry, firm, nonblanching, translucent appearance, often resembling parchment paper, or an anesthetic, charred, tan appearance with a leathery consistency. Such burns heal slowly, often over months, with hypertrophic scarring and contractures. First- and second-degree burns are generally painful, whereas destruction of the dermal plexus of nerves in third-degree burns renders the tissue insensitive to pain (Table 7-1).
III. WORKUP
Factors that determine burn severity include total body surface area (TBSA) involvement (only second- and third-degree burns), depth of the injury, age, associated injuries, delay in resuscitation, and use of drugs, among others. Although a simplified approximation, the Rule of Nines is a quick and useful technique in assessing TBSA in adults (Fig. 7-1). Adjustments must be made for children under 10 years of age. Approximating the palmar hand surface as 1% TBSA may be used in this patient population. The depth of the burn and additional injuries are directly proportional to the severity. Mortality for a given burn size is directly proportional to the age. Delayed resuscitation efforts negatively dictate treatment options, and the use of drugs hinders resuscitation efforts greatly.
TABLE 7-1 Severity of Burns | |||||
|---|---|---|---|---|---|
| |||||