Burn Scars
Jill S. Waibel
Ashley Rudnick
BACKGROUND
Advances in burn care over the last decade have resulted in new innovations, better treatment, and improved outcomes.1 Patient care is championed by the collaboration of many disciplines focused on team work of each individual burn survivor.2 Burn trauma remains one of the most devastating injuries we address as physicians. The strength of burn victims must be respected as they endure pain, infection, organ failure, scarring, and functional compromise. Their life, families’ life, social network, and employment is jolted into turmoil. The complexity of treating burn patients from the moment they enter the burn unit through to reconstructive procedures is a journey and mandates dedication of all providers.3
Rehabilitation from a traumatic injury begins acutely within minutes of admission to the intensive care unit or burn unit and continues for months to years.2 After injury a complex stepwise fashion occurs that depends on intrinsic and extrinsic forces involving hundreds to thousands of unique biological growth factors, inter-leukins, adhesion proteins, and differentiated cells. Many factors affect how scar will ultimately heal, including location injury, hormones, genetics, chronic inflammation, tension on the wound borders, and delayed epithelization (>21 days).
Scars are the ultimate outcome of skin injury and cause significant morbidity to the patient.
Studies show the prevalence of scar contractures at dis-charge is high around 40% to 55%, thus showing the need for optimal and timely rehabilitation.4 Outpatient care is essential to success. No 2 patients have the same scar; thus, every burn and trauma patient must have an individualized multidisciplinary healing plan from their physician team.5
Advances and understanding in wound healing have improved burn and trauma injury and scar management. Traditional therapy was extensive surgical intervention, with trauma patients often having upward of 40 surgeries. The role of dermatologist has expanded with the advancements of laser surgery, laser surgery with phar-macotherapy, and minor surgical procedures. Burn and trauma injuries most commonly form hypertrophic and contracture scars 2 to 7 months after the initial injury. Hypertrophic burn scars can drastically affect patient’s daily lives.6 Neuropathic pain, pruritus, and decreased range of motion decrease patients’ level of function in work and recreational arenas.7,8,9,10
PRESENTATION
A burn scar from injury begins acutely within minutes and continues for months to years.2 Initially, a burn scar may present as an erythematous patch or plaque, vesicles or blisters, or an ulcer.
DIAGNOSIS
Clinical Diagnosis
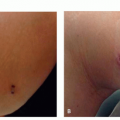
The most common type of postinjury burn scar is a hypertrophic scar (Figure 8.3.1). Hypertrophic scarring is a late complication of thermal cutaneous injury that can lead to substantial functional impairment and disfig-urement. It appears as a thick flesh-colored or hyperpigmented plaque corresponding to the site of injury.
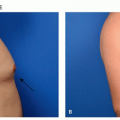
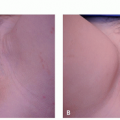
Hypertrophic scars may occur anywhere on the body but have especially detrimental consequences when across joints that may lead to scar contractures and decreased range of motion11 (Figure 8.3.2). Bombaro et al. reported that hypertrophic scarring develops in up to 80% of all burn patients with partial and deep-thickness injuries.10
 FIGURE 8.3.1 A 62-year-old Caucasian woman with Fitzpatrick skin type II with erythematous, hypertrophic burn and traumatic scar on right leg due to fire explosion from motorcycle accident. |
 FIGURE 8.3.2 A 10-year-old Caucasian boy with Fitzpatrick skin type II with erythematous, hypertrophic, contracture burn and traumatic scar due to fire explosion from indoor firepit. |
Histopathology
Hypertrophic scars are characterized by excessive and disorganized deposition of both extracellular matrix and collagen. Histologically, hypertrophic scars have a nodular appearance with dense whorled fibroblast proliferation in the dermis, increased numbers of abnormal type III collagen-containing myofibroblasts, large collagen bundles, and occasionally increased dermal mucin.12 Keloidal scars are also nodular but are rela-tively hypocellular, with thick, dense, hyalinized collagen bundles often described as having “bubble gum” appearance.
Subtypes
First degree: Erythematous, dry, and tender.
Second degree: Erythematous, wet, and very painful. Propensity to develop hypertrophic scars. May have vesiculation.
Third degree: Dry, erythematous to hyperpigmented, insensate, and waxy in appearance. Heals with contractures. Typically associated with overlying blistering. Intact blisters help with pain control. Debride if infection occurs.
Fourth degree: Underlying subcutaneous tissue, ten-don, or bone exposed.
Differential Diagnosis
The distinction between third- and fourth-degree burn scars is difficult, and often the extent is underestimated.
Spontaneous generalized keloids
Sclerotic xanthoma disseminatum
Keloidal scleroderma
PATHOGENESIS
The rehabilitation of a patient with burn injury is a complex, time-consuming journey in rehabilitation medicine. Rehabilitation starts in the burn unit by understanding each individual patient’s functional losses caused by the injury.13 Burn care includes reconstruction, rehabilitation, and recovery.14 Reconstruction is the restoration of skin and other structures that are causing loss.15 Comprehensive care allows a person to have meaningful recovery and participation back to their life. Burn injuries may be quite extensive and may include brain injuries, peripheral nerve injures, amputations, and scarring. For the purposes of this chapter we will focus on the understanding and treatment of the cutaneous scarring.
Scar formation is the consequence of trauma to the skin that may affect epidermis, dermis, fat, fascia, or muscle. There are different types of scars, including immature (less than 12 months from injury), mature (greater than 12 months from injury), atrophic, hypertrophic, contracture, or keloids (Figure 8.3.3). The development of different types of scars depends on many factors including the type and severity of injury, age, anatomic area, course of healing process, genetics, and individual predilections.
From the time of wound closure there is a strong potential for development of hypertrophic scarring after burn injury. Family genetics increase the likeli-hood of developing hypertrophic scarring. The time to heal directly correlates to the propensity to form hypertrophic scars, with scars healing in 14 to 21 days having a 30% incidence of hypertrophic scar.16,17,18
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


