Introduction
The female breast is a defining characteristic of femininity, and its distortion or absence may result in significant quality of life impairment and psychological distress. As a result, a variety of surgical techniques have been developed for reconstruction of congenital, traumatic, or oncological defects of the breast. These procedures have naturally and iteratively evolved over time, resulting in better cosmetic results and decreased surgical morbidity. Improvements in reconstructive outcomes increase overall satisfaction, self-esteem, body image, quality of life, and psychological well-being. In a testament to the benefits of breast reconstruction, the Women’s Health and Cancer Rights Act was enacted in 1998, mandating insurance coverage for breast reconstructive procedures in the United States. These advances are important because nearly 1 in 9 women will develop breast cancer in their lifetime. In the United States alone, nearly 250,000 new cases are detected annually, accounting for nearly 33% of all new cancer diagnoses per year.
This chapter is an overview of current practices in breast reconstruction and aims to cover the general principles of these procedures. It is not the intent of the authors to provide an encyclopedic discussion of this topic as entire textbooks have been written on portions of this chapter. As a result, the interested reader is guided to several excellent texts and landmark papers and manuscripts through this review.
Reconstructive Goals
The goals of breast reconstruction are to recreate a natura- appearing breast in clothing and, ideally, also when undressed, while limiting surgical morbidity. This process is individualized to best fit the reconstructive needs for volume and skin while taking oncological, social, and other concerns into consideration. As a result, a detailed history and physical examination paying close attention to social history, oncological history (when applicable), personal preferences of the patient, and availability of donor sites for reconstruction is necessary. This is a complicated process and requires practice and sensitivity. Nevertheless, successful completion of breast reconstruction is highly gratifying and personally rewarding.
Despite the nuances in anatomy, the breast can be defined by its fixed anatomical boundaries or “footprint” on the chest wall. Specifically, these boundaries include the inframammary fold (IMF) inferiorly; the second rib superiorly, the lateral border of the sternum medially; and an area located 1–2 cm posterior to the anterior axillary line laterally. Several authors have even attempted to quantify the ideal characteristics of an esthetic breast. However, while these measurements may represent the “ideal” breast shape, the reconstructive surgeon should aim for symmetry and pay attention to the patient’s desire which, in some cases, may differ substantially from these ideals. With this as a background, the reconstructive surgeon can begin to analyze surgical options for reconstruction of the complex three-dimensional shape of the breast. As the breast is naturally made up of skin, fat, and glandular tissues, a patient’s own skin and fat provide the most analogous tissue for a natural-appearing reconstruction. Shaping this tissue into an esthetically pleasing breast, however, can be a challenging task. Implants are also useful in many patients and can provide a pleasing reconstructive outcome.
Mastectomy Incisions
Mastectomy can be performed with a variety of incisions, including nipple sparing, skin sparing, Wise pattern, among others. The selection of the mastectomy incision should be made in conjunction with the breast surgeon and depends on oncological and esthetic factors. Esthetic factors include the size and shape of the breast, the degree of ptosis and the patient’s desires. This last point is very important. A large-breasted patient who desires a reduction and lift following their mastectomy is not served well with a nipple-sparing mastectomy since failure to fill the breast envelope will result in contour deformities that are difficult to manage. One option in these cases is to proceed initially with a breast reduction and lift, wait until the skin has fully healed and the blood supply to the nipple–areola complex (NAC) is restored through the periareolar scar, and then proceed with mastectomy. This option is not always possible or advisable in women who have active breast cancer. In most cases, an excellent outcome is achievable with virtually any breast incision if a reasonable mastectomy that does not overly thin the breast skin or violate the borders of the breast is performed.
Nipple-Sparing Mastectomy
Nipple-sparing mastectomy is an excellent option for most women. However, this approach may not be feasible in cases where the breast tumor is close to or involves the NAC. Nipple-sparing mastectomy is also not a good option in women with significant ptosis or those with very large breasts. The skin tone and thickness, as well as a sound approach to mastectomy taking care to preserve the blood supply of the skin and avoiding undue tension with retraction, are vitally important.
Nipple-sparing mastectomies can be performed with an incision in the inframammary fold, lateral breast incision with or without a periareolar extension, or a vertical incision. These incisions all have advantages and disadvantages. For example, a lateral incision decreases the length of the mastectomy skin flap and allow excellent exposure of the upper/outer part of the breast. In addition, if mastectomy or skin flap or nipple–areola necrosis occurs following surgery with this incision, the skin can simply be excised and re-expanded with an expander converting the procedure to skin-sparing mastectomy. However, the lateral breast nipple-sparing mastectomy incision has a higher rate of nipple–areola necrosis (particularly if the incision is extended around the NAC). This incision is also more likely to result in outward malposition of the nipple–areola by decreasing the relative potential of expansion of the lateral breast skin as compared to the medial breast skin. As a result, the medial breast area may be overexpanded, thus shifting the position of the nipple laterally.
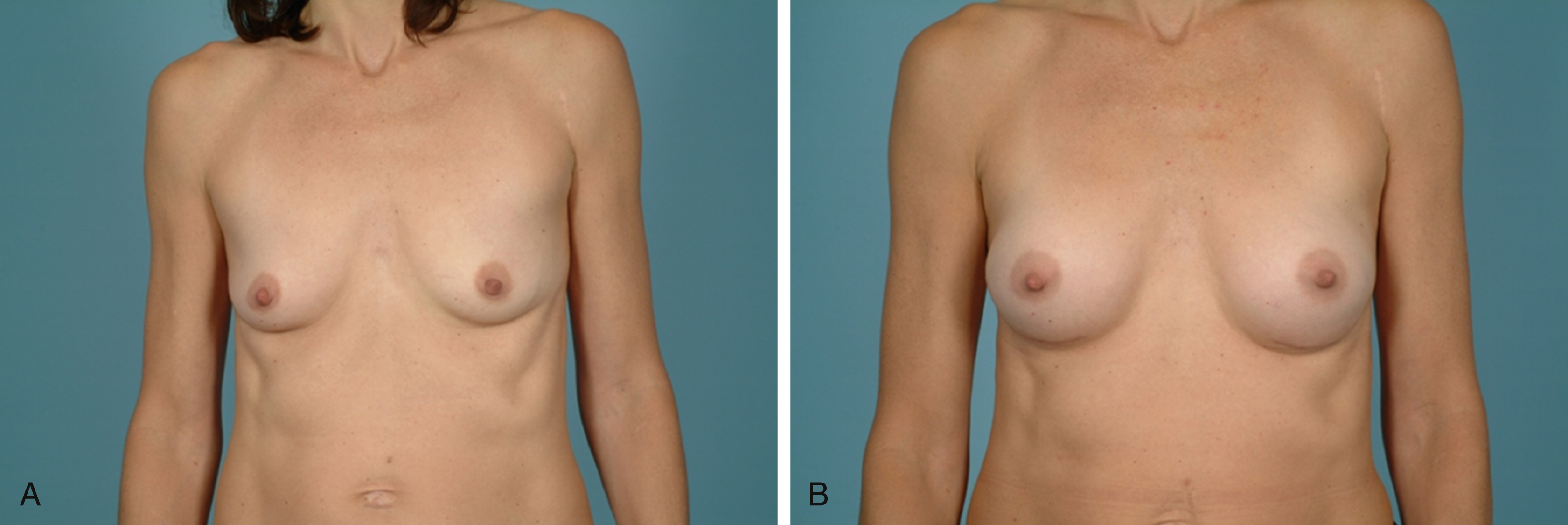
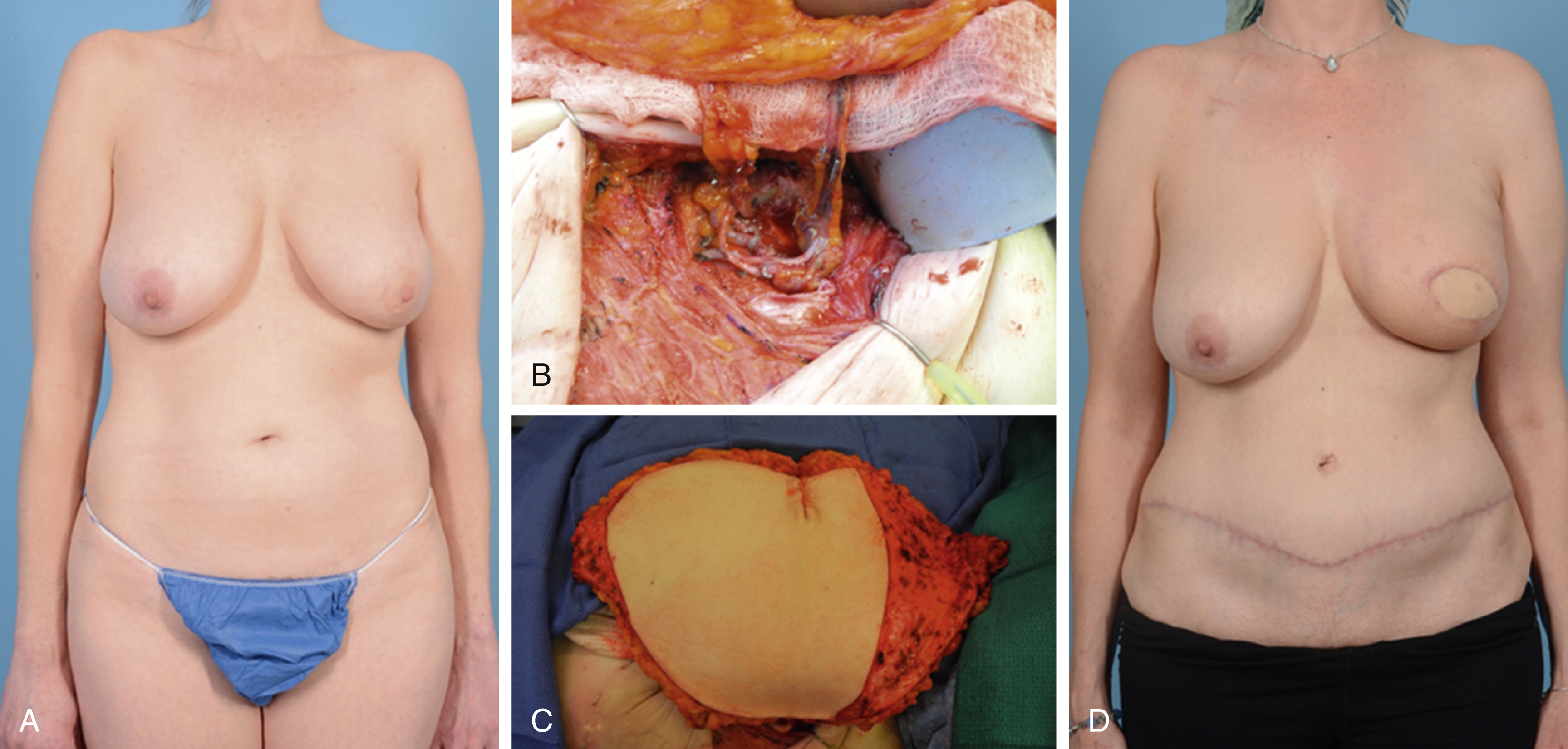
The inframammary incision avoids all incisions on the breast and can hide the mastectomy incision in the fold. This incision also avoids cicatricial distortion of skin expansion and is less likely to cause nipple malposition. However, the inframammary incision is more technically challenging, particularly in patients with large or more ptotic breasts. This incision also limits exposure of the upper part of the breast and may complicate resection of upper–outer or upper–medial breast tumors. Excess tension on the skin with retraction or disturbance of skin perfusion may result in skin necrosis that is difficult to deal with in patients treated with inframammary mastectomy since there is little excess skin laxity in this area and excision of necrotic skin will almost certainly result in distortion of the reconstructed breast. In severe cases, mastectomy skin ischemia may involve a triangular-shaped area that includes the NAC and the skin incision ( Fig. 36.1 ). Full-thickness necrosis in these cases necessitates reconstruction with a flap to replace the skin and restore the normal shape of the breast. Finally, the inframammary skin incision may make it difficult to expose recipient vessels for free flap breast reconstruction. Nevertheless, in experienced hands, the inframammary incision results in excellent esthetic outcomes ( Fig. 36.2 ).

The vertical nipple-sparing mastectomy incision is an excellent choice in cases where autologous reconstruction is planned. This incision facilitates excellent exposure of the breast for mastectomy and dissection of the internal mammary artery/vein for microvascular anastomosis. Likewise, the vertical incision is less likely than the lateral breast incision to cause nipple–areola malposition. However, in our experience, this incision has a higher rate of nipple–areola ischemia than the inframammary incision, particularly when an extensive mastectomy is performed. Nevertheless, in cases where perfusion of the mastectomy skin is damaged, these areas can simply be excised and expanded or replaced by skin from the free flap.
Skin-Sparing Mastectomy
Skin sparing mastectomy is a good option in most cases and provides flexibility for reconstruction and excellent exposure for mastectomy. Skin-sparing mastectomy is safe and does not increase the risk of local recurrence or distant metastasis. The most aggressive skin-sparing mastectomy is an areola-sparing mastectomy in which the nipple but not the areola is resected along with the breast. This is an excellent option in women who wish to maximally minimize their risk of breast cancer by removing as much breast tissue as possible since the areola, unlike the nipple, does not contain breast ducts. The areola-sparing mastectomy can also help hide the scar from the procedure within the areola or just outside it thus decreasing the final length of the mastectomy incision because a large elliptical excision of the NAC is avoided. Finally, the preserved areola skin is thicker than the surrounding breast skin and regains muscular activity following mastectomy. These features preserve the ability of the areola skin to respond to cold or touch thereby permitting reconstruction of a highly esthetic nipple. This incision is not ideal, however, for patients with excess ptosis or those in whom the breast tumor extends close to or involves the NAC.
Skin-sparing mastectomy can also be performed by simply excising the NAC with a circular incision and replacing this area with skin from a flap. A vertical or medial extension of this incision can greatly increase the exposure of recipient vessels while preserving the overall esthetics of the breast. This incision has also been reported for use with tissue expander/implants closing the mastectomy skin in a “cross-shaped” fashion. However, in our experience, we have found that this approach limits expansion of the central breast area and decreases projection where it is most needed. In most cases, an elliptical incision removing the NAC and skin lateral/medial to this area is the best option for skin-sparing mastectomy when tissue expander/implant reconstruction is planned. This approach allows excision of all excess skin and redraping to avoid medial/lateral breast dog ears. Wider elliptical excisions also allow lifting the breast and repositioning the reconstruction higher up on the chest; however, this approach can result in long, unsightly incisions that are difficult to hide.
Non-Skin-Sparing Mastectomy or Delayed Reconstruction
In some cases, skin-sparing mastectomy is not possible. This is an issue, for example, in patients who have been previously treated with radiation and have unfavorable prior partial mastectomy scars (i.e., incisions that are not in-line with the NAC or located in anatomically unfavorable areas of the breast). These patients are at high risk of developing mastectomy skin flap necrosis if a standard skin-sparing mastectomy is performed. In other patients, the skin may be involved with tumor and may require wide resection, or the skin may be previously damaged by radiation and thereby not suitable for reconstruction. In these cases, it is often better to remove the damaged skin and replace it with healthy flap skin thus, at the minimum, restoring the natural shape of the breast but at the cost of larger breast incisions.
Wise Pattern Mastectomy
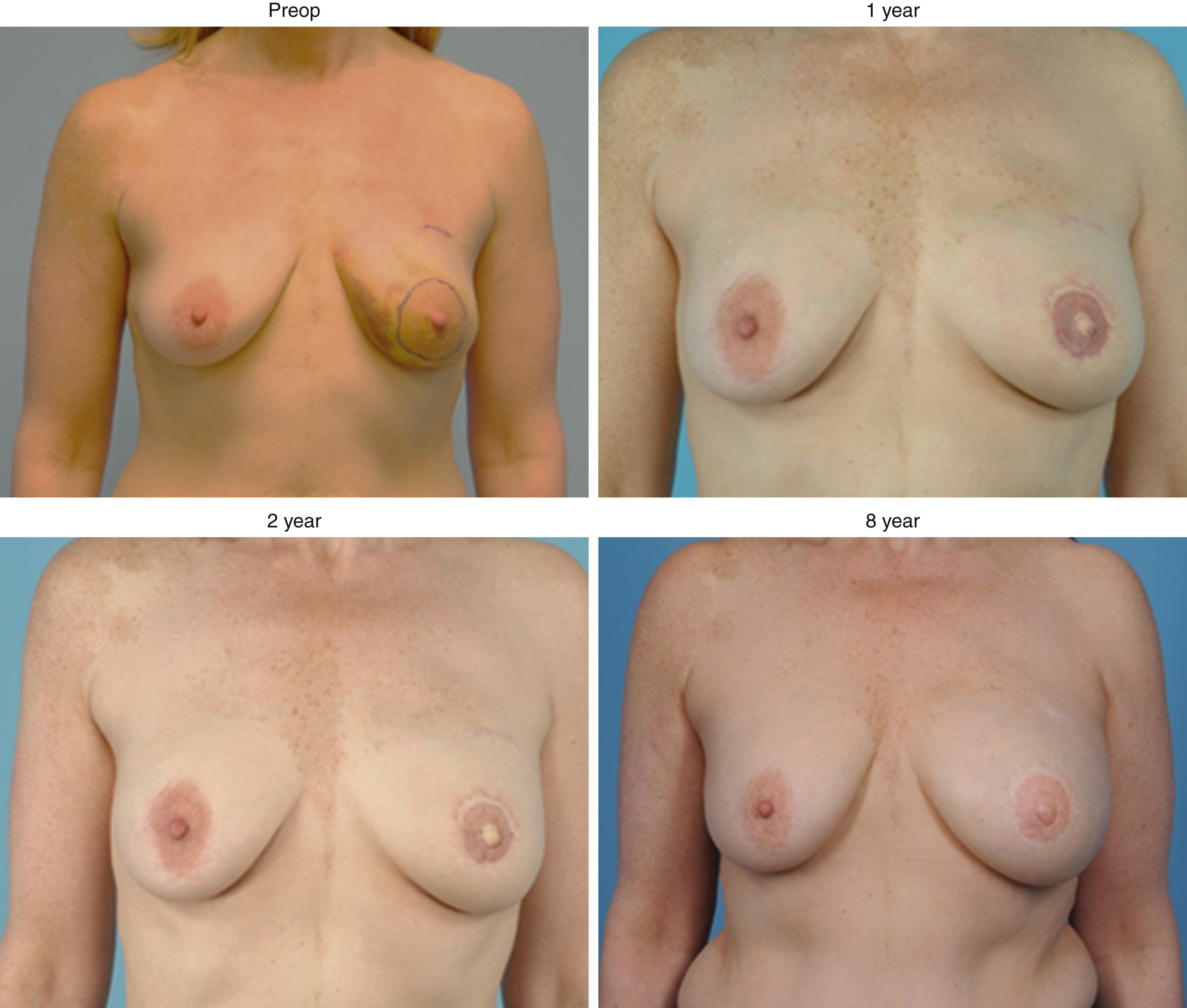
Wise pattern mastectomy is an excellent option for patients with breast ptosis or macromastia. This incision enables reduction of the skin envelope and simultaneous narrowing of the breast width. In addition, preservation of the lower mastectomy skin flap increases lower pole projection and covers the T-point, thus providing an extra layer of protection in case of skin breakdown or mastectomy skin flap necrosis. The Wise pattern mastectomy is designed as would be performed for a standard breast reduction. In our experience, it has been helpful to make the vertical limbs of the pattern slightly longer than usual (8–10 cm rather than the typical 7 cm used for Wise pattern breast reduction). The mastectomy is done using the vertical and upper flap incisions, and the breast is dissected from the lower skin flap that would ordinarily be removed following breast reduction. This skin flap is then de-epithelialized and used to cover the lower portion of the reconstruction (either a tissue expander or autologous breast reconstruction) to improve projection and contour of the lower breast pole. The Wise pattern mastectomy can be technically challenging for breast surgeons, particularly in women with severe macromastia. Aggressive mastectomy with violation of the later breast fold or dissection above the level of the second rib greatly increase the risk of mastectomy skin flap necrosis. In these situations, the lower mastectomy skin flap can be used to replace the ischemic breast skin, and indocyanine green angiography (ICGA) is helpful to assess the degree of skin resection necessary. This results in the placement of a triangle of skin in the inferior portion of the breast; however, the long-term results can still be excellent ( Fig. 36.3 ).

Autologous Tissue Breast Reconstruction
Autologous tissue breast reconstruction, in the appropriately selected patient, offers several advantages over implant-based techniques. This approach usually results in a more natural-appearing and more natural-feeling reconstructed breast and avoids the long-term complications of breast implants such as capsular contracture, implant rupture, and asymmetry due to weight gain or aging ( Fig. 36.4 ). Autologous breast reconstruction is, however, more technically challenging and demands a thorough understanding of anatomy and tissue perfusion. As a result, progress in surgical techniques together with advanced knowledge of anatomy have led to continuous improvement and evolution of autologous breast reconstruction resulting in better esthetic outcomes and decreased donor site morbidity.
In 1965, the microsurgery pioneers Tamai and Komatsu successfully replanted an amputated thumb at the metacarpophalangeal joint, marking the beginning of the microsurgical renaissance in plastic and hand surgery. This was followed in 1973 by Taylor and Daniel’s report of a successful free microvascular skin flap and then in 1975 by Toyomi Fujino, who performed the first microvascular reconstruction of a congenital breast aplasia defect with a free myocutaneous flap from the buttocks anastomosed to the thoracoacromial vessels. These technical advances facilitated transplantation of tissues from one part of the body to another and increased the number of options available for reconstruction.
Ground-breaking anatomical dissections by Taylor and Palmer in the late 1980s described the concept of skin angiosomes, identifying source vessels for various regions of the body. This was an important discovery and suggested that large areas of skin could survive based simply on a single artery and vein (i.e., a perforator), leading the way for the development of a variety of flaps. The angiosomes concept has thus served as a basis for rational, anatomically-based flap design and has greatly advanced autologous tissue breast reconstruction using donor sites that include the abdomen, the inner/outer thighs, the back, and the gluteal areas.
Abdominally-Based Flaps
Pedicled Transverse Abdominis Myocutaneous Flap (pTRAM)
History
The abdomen is the ideal donor site for autologous breast reconstruction because this area can provide ample tissue, and the donor site scar can be placed in a favorable position. The abdomen also enables harvesting of a large skin paddle that is suitable for reconstruction of large chest wall defects. The use of abdominal tissues for reconstruction can be traced back to Sir Harold Gillies, who first described the use of tubed abdominal flaps for breast reconstruction in 1942. These operations required multiple delay procedures and often resulted in flap failure. This history is nicely reviewed by Uroskie and Colen. In 1977, Drever described the use of the epigastric island flap, now commonly referred to as the vertical rectus abdominis myocutaneous flap (VRAM), for breast reconstruction. This flap had an excellent blood supply and, unlike the previously reported tubed flaps, could be transferred in a single operation. A few years after this initial report, Robbins described the use of the VRAM flap for breast reconstruction. The abdominal donor site rapidly gained popularity and became the workhorse for reconstruction following the description of the pedicled transverse rectus abdominis myocutaneous flap (pTRAM) flap by Hartrampf et al, in 1982. This flap is based on skin perforators arising from the deep superior epigastric artery and vein, and enabled surgeons to place the abdominal scar in the lower abdomen. The ability to improve the contour of the abdomen while reconstructing the breast was intuitively appealing to both patients and plastic surgeons. In addition, unlike the latissimus flap (the other commonly used autologous option at the time), the pTRAM flap provides a large amount of skin and soft tissues that could be used to replace the missing skin/volume of the breast without an implant. This was particularly important in the early 1980s since at that time, immediate breast reconstruction was rarely performed, and most women who presented for breast reconstruction had large skin and soft tissue deficits.
Patient Selection
The pTRAM can be performed in patients who have a suitable body habitus and sufficient lower abdominal skin and fat to restore the volume of the breast. Obesity, active smoking, significant co-morbid conditions, and history of prior abdominal surgery are relative contraindications. Obesity and smoking significantly increase the risk of complications, including partial flap loss, fat necrosis, and abdominal wall complications. Patients with a history of open cholecystectomy are at high risk of abdominal skin necrosis and hernia. The right upper rectus muscle is also transected in this operation, thereby precluding harvest of a right-sided flap. A prior history of abdominoplasty is a contraindication for pTRAM flap breast reconstruction. Other abdominal operations such as cesarean section, midline laparotomy, laparoscopy and appendectomy, increase the risk of abdominal complications but may be feasible if the rectus muscle has not been injured. Prior chest wall surgery, including medial sternotomy or procedures in which the internal mammary artery/vein have been damaged or resected, usually preclude the use of a pTRAM flap for breast reconstruction.
Surgical Technique
The pTRAM is still commonly performed in many areas of the United States and Europe. This procedure is relatively simple to perform, does not require microsurgical skills and, in experienced hands, can provide excellent outcomes. The flap is marked in the lower abdomen with the upper skin incision line usually drawn 1–2 cm above the umbilicus. This upper incision placement does place the lower abdominal incision higher than a typical abdominoplasty or free TRAM flap (see below), however, capturing the periumbilical perforators greatly improves the blood supply of the flap and decreases complications such as fat necrosis or partial flap loss. The upper skin incision is performed, and the upper skin flap is elevated to the level of the xyphoid centrally and the costal margin laterally. The lower incision is then performed, and the flap is carefully elevated from lateral to medial taking care to preserve the cutaneous perforators arising from the rectus muscle in these areas. The flap dissection is continued to expose the medial and lateral row perforators arising from the rectus muscle and supplying the overlying skin. The anterior abdominal wall fascia is then incised, and the intercostal branches to the rectus muscle are ligated. The inferior epigastric artery and vein are identified and dissected distally for 5–8 cm and ligated. The inferior epigastric pedicle can be used as a fallback and anastomosed to recipient vessels in the chest in case the perfusion from the superior epigastric artery/vein is inadequate. The rectus muscle is then dissected from inferior to superior taking care to avoid injury to the pedicle vessels that run on the deep surface of the muscle. The flap may be transferred to the breast from the ipsilateral or contralateral abdominal area. In the authors’ experience, we have found that an ipsilateral flap has a longer reach and results in less significant disruption of the inframammary fold. Once the flap is dissected, a tunnel is made connecting the abdominal site to the breast, and the flap is carefully pulled through to avoid avulsion of the cutaneous perforators of the flap. The perfusion of the flap is then assessed, and the flap is inset into the defect to reconstruct the breast.
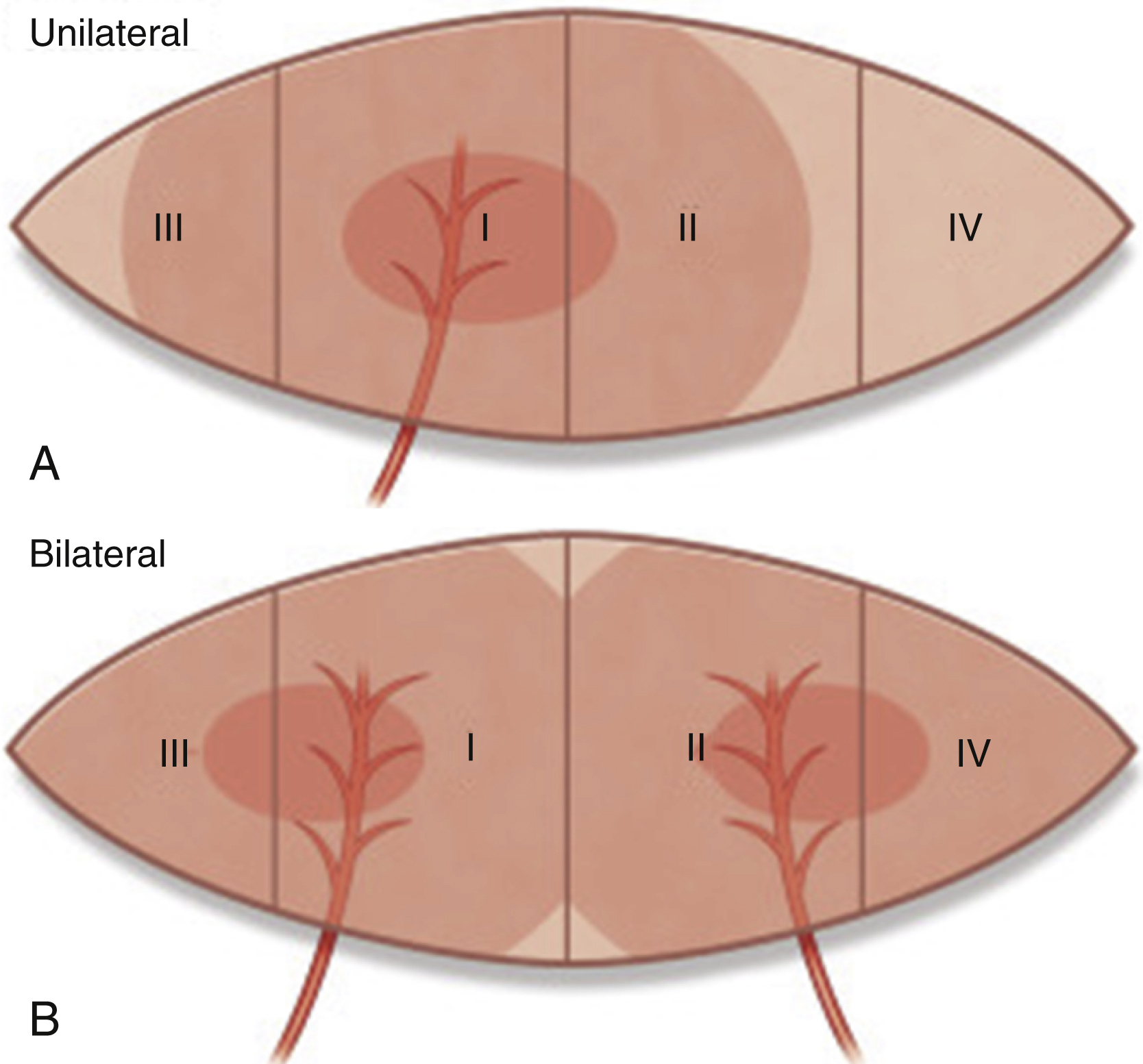
Hartrampf divided the abdominal tissues into four zones: zones 1 and 2 are ipsilateral to the harvested muscle while zones 3 and 4 cross the midline to the other side ( Fig. 36.5 ). Zones 1 and 2 can be consistently transferred with a pTRAM. However, extended flaps with large segments of zone 3 are less reliable and susceptible to distal necrosis. Zone 4 is not well perfused and should not be used with a pTRAM. Perfusion across the midline of the abdomen can be improved by anastomosing the deep inferior epigastric vein to a recipient vein in the axilla, a process known as supercharging a flap. Less commonly, the deep inferior epigastric artery may also require anastomosis. Another option is to delay the flap by incising the skin and ligating the deep inferior epigastric vessels 2–4 weeks prior to flap transfer. Other authors have described the use of bipedicle TRAM flaps in which both rectus muscles are harvested, thus providing a dual blood supply to the skin. This surgical approach enables transfer of virtually all of the lower abdominal skin/fat and greatly increases the perfusion of the flap even in patients with comorbid conditions such as obesity; however, removal of both rectus muscles can be quite morbid, decreasing abdominal/core strength and resulting in higher rates of hernia formation as compared to a unilateral pTRAM or other abdominally-based flaps.
The abdominal fascia is closed either primarily, or more commonly, using permanent mesh that is placed as an inlay between the edges of the fascia. The contralateral fascia is often plicated to bring the umbilicus back to the midline. The patient is brought into a slightly flexed position, and the abdominal skin is closed over drains. Progressive tension sutures repairing the skin to the abdominal fascia are helpful to avoid excess tension on the abdominal skin incision and decrease the rates of abdominal seromas. These sutures usually enable the surgeon to remove the abdominal drains in a week or less following surgery.
Outcomes
The pTRAM flap is safe, with very low reported rates of complete flap loss. However, the rate of partial flap loss is significant (2%–10%) and can result in delayed healing, distortion of the reconstructed breast, and poor esthetic outcomes. The reported rates of fat necrosis with pTRAM flap reconstruction are also highly variable, ranging from 2%–3% to as high as 20% and depend largely on the surgical technique, the surgeon experience, and the definition of a clinically significant area of fat necrosis. These ischemic flap complications occur because the superior epigastric artery and vein are not the dominant blood supply of the lower abdominal skin and because there is considerable variability in the number/size of connections between the superior and inferior deep epigastric vessels. Thus, placing the flap higher up on the abdomen improves the blood supply by increasing the likelihood of capturing perforators that arise from the deep superior epigastric vessels. However, this flap design decreases the arc of rotation of the flap and results in a higher/less aesthetic lower abdominal donor scar.
The pTRAM also can be associated with high rates of abdominal wall complications such as abdominal wall laxity or hernia. These complications can occur in as many as 10%–12% of patients, although very low hernia rates have been reported by some authors. Nevertheless, the closure of the abdominal wall is crucially important since the long fascial incision, together with the removal of the entire muscle clearly disrupts the abdominal wall and can result in significant morbidity.
Free TRAM (fTRAM) and Muscle-Sparing TRAM (msTRAM)
History
With time comes experience, and the high rate of fat necrosis and abdominal wall complications of the pTRAM led surgeons to experiment with other techniques aiming to decrease the incidence of these problems. In 1979, Holmström reported the use of the free TRAM flap in a series of experiments conducted on discarded abdominoplasty tissues. Using angiography studies and a clinical series, he showed that the blood supply to the lower abdominal skin was reliable and that the procedure was technically feasible. The msTRAM was an evolution of the fTRAM and aimed to further decrease the morbidity of a fTRAM by decreasing the amount of muscle and fascia harvested with the flap.
Patient Selection
The fTRAM and msTRAM have the same indications and relative contraindications as the pTRAM. However, because of the improved perfusion of the free flap options, these procedures are usually well tolerated, with low rates of complications even in obese patients. Active smokers have higher rates of wound healing complications; however, free flap breast reconstruction is an option if the patient understands the risk. These complications are generally self-limited and usually resolve without the need for additional surgical intervention. Similarly, prior abdominal surgery or a history of prior abdominal liposuction do not preclude fTRAM or msTRAM breast reconstruction; however, it may be necessary to confirm the continuity of the pedicle vessels with imaging studies. A history of clotting abnormalities is a relative contraindication to these procedures as the risk of vascular complications is significantly increased in these patients. However, this risk may be mitigated by judicious use of anticoagulation.
Surgical Technique
To perform an fTRAM, the lateral and medial edges of the rectus muscle are identified, and the abdominal fascia is incised. The rectus muscle is transected superiorly and inferiorly, and the inferior portion of the muscle together with the deep inferior epigastric artery and vein are harvested. The flap is then transferred to the chest and perfusion is restored with microvascular anastomosis to the thoracodorsal artery/vein or the internal mammary artery/vein.
In the msTRAM, the lateral and medial borders of the rectus muscle are identified, and the dissection continues with exposure of the lateral and medial row perforators. The flap is elevated to spare as much of the fascia as possible. The fascia is incised, and the perforating vessels are harvested together with a portion of the rectus muscle. Usually, the central portion of the rectus muscle is harvested leaving the medial and lateral borders of the muscle intact and in continuity with the upper portion of the muscle. This is important since the neurovascular supply to the rectus muscle is derived from the lateral intercostal nerve branches leaving at least some of the muscle innervated. This procedure also decreases the amount of fascia that is removed, thus decreasing the need for mesh reconstruction.
A two-team approach is usually used for flap harvest and preparation of recipient vessels. The internal mammary vessels are the recipient vessels of choice for most surgeons, as they are of similar caliber to the deep inferior epigastric vessels and can be exposed widely for ease of microsurgical anastomosis. In most instances, the 3rd rib cartilage is removed in part or in whole to provide access to the underlying internal mammary artery/vein; however, a rib-sparing approach can be used. Alternately, the thoracodorsal vessels can be used as recipient vessels.
Once the flap dissection is completed, and recipient vessels have been prepared, the anterior surface of pedicle vessels is marked with methylene blue or a marking pen, and the vessels are divided. Marking the anterior surface of the pedicle helps to avoid twisting of the pedicle during microvascular anastomosis. The microsurgical anastomosis is performed, and the flap is inset. The abdominal wall is repaired, and mesh is used as necessary to reinforce the abdominal fascia repair. Transversus abdominis plane blocks are used at our center for postoperative pain control in the abdomen. The patient is brought into a slightly flexed position, and the abdominal skin is closed as discussed for the pTRAM.
Outcomes
Several groups have compared outcomes between the fTRAM flap with the pTRAM and demonstrated decreased rates of partial flap loss, fat necrosis, abdominal wall laxity, and hernias. The use of the fTRAM also avoids the unsightly bulge in the epigastrium that can occur with the tunneling of the pTRAM into the breast area. The improved blood supply of the fTRAM enables the safe transfer of larger amounts of abdominal tissues, facilitates inset of the flap, and improves esthetic outcomes in the breast and the abdomen.
The msTRAM and the fTRAM have an excellent blood supply and tissue perfusion that routinely enable the transfer of tissues across the midline, including most or all of zone 3 and, occasionally, even zone 4. In experienced hands, these flap options have excellent outcomes with low rates of total flap loss (<1%) and fat necrosis (5%–8%). A recent meta-analysis of 11 studies comparing outcomes following 1891 pTRAM vs. 866 fTRAM flaps found a significantly lower risk of fat necrosis and partial flap loss with microvascular techniques. Another meta-analysis of outcomes following msTRAM and fTRAM reported a pooled rate of 4.9% for fat necrosis, 1.8% partial flap loss, and 1% total flap loss. The msTRAM and fTRAM also have lower rates of abdominal wall complications and decreased abdominal weakness as compared to the pTRAM. The pooled rates of abdominal wall bulge/laxity/weakness in a meta-analysis of 14 studies was 5.9% while the rate of abdominal hernia was 3.9%.
Deep Inferior Epigastric Artery Perforator (DIEP) and Muscle-Sparing TRAM Flaps
History
In 1989, Koshima and Soeda first described the concept of the “inferior epigastric artery skin flaps without rectus abdominis muscle” for the reconstruction of a groin defect and a defect of the oral cavity. A few years later, Robert Allen Sr reported the use of the deep inferior epigastric artery (DIEP) flap for breast reconstruction. Since its original description, numerous authors have published favorable outcomes with the DIEP flap, and its use has become routine in centers that specialize in microvascular autologous tissue breast reconstruction.
Patient Selection
The DIEP flap is usually the first choice for microsurgical autologous reconstruction because of its long pedicle length, the caliber, and ease of dissection of the inferior epigastric artery and vein, the large amount of skin and fat that can be harvested, and the inconspicuous donor site scar. The ability to simultaneously reconstruct a bilateral mastectomy with one donor site scar is also a major advantage of the DIEP flap. The DIEP flap has the same indications and relative contraindications as the fTRAM/msTRAM.
Surgical Technique
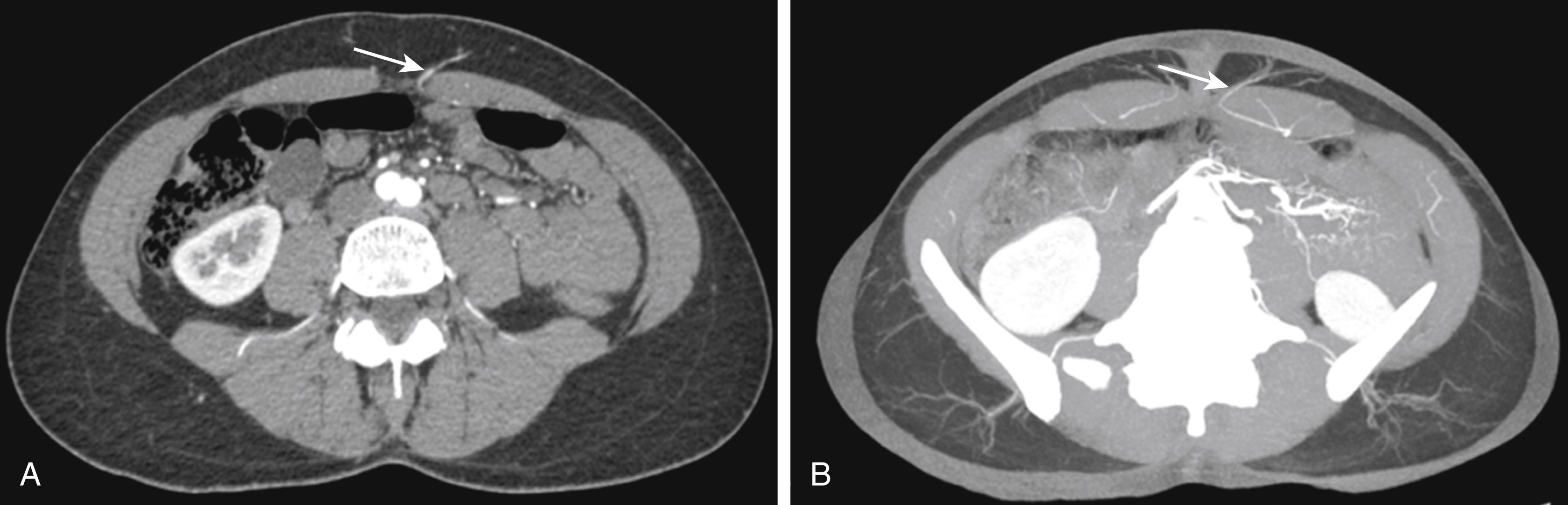
The DIEP flap is the natural evolution of the muscle-sparing flap. In this procedure, the perforating vessels that perfuse the skin are dissected free from the rectus muscle, and the innervation of the muscle is largely maintained. The size and location of the abdominal wall perforators can be assessed preoperatively using computed tomographic angiography (CTA) or magnetic resonance angiography (MRA) ( Fig. 36.6 ). This information may enable the surgeon to assess the feasibility of performing a DIEP, decrease operative time, and provides an estimate of the amount of tissues available for breast reconstruction. The position of the perforators is usually marked in relation to the umbilicus, and the flap is designed to capture the largest perforators. In some cases, however, preoperative imaging may not be available, and the procedure can simply be performed by surgically exposing the perforators and selecting the best option for reconstruction. The use of a handheld Doppler may help identify perforators preoperatively in these cases; however, in general, this is not necessary.
Flap dissection is begun as with the msTRAM to elevate the upper abdominal flap and to identify the perforating vessels to the skin. The superficial inferior epigastric vein (SIEV), if present, should be identified and dissected for several centimeters. This vessel may be useful as an additional venous outflow option if the flap is congested following the completion of perforator dissection. If a preoperative MRA or CTA was performed, this is used to guide the surgeon to the “ideal” perforator. Without imaging, the surgeon should choose the largest perforator encountered. This can be judged based on size, visible pulsation, or handheld Doppler ultrasound. Once a perforator(s) is chosen, the anterior abdominal wall fascia is incised, taking care to avoid injury to the vessel. The perforator is then carefully dissected through the rectus muscle back to the main pedicle. The length of the pedicle dissection is guided by the size of the recipient vessels and the surgeon’s preference. In cases where multiple perforators are harvested, it may be necessary to divide motor branches that travel between the perforators. These motor nerve branches can usually be microsurgically repaired.
Prior to division of the pedicle, it is prudent to assess the perfusion of the flap by checking capillary refill and bleeding from the edges of the flap. These clinical signs can alert the surgeon to areas of the flap that are not well perfused. This assessment can be confirmed using ICGA. This technology can also be used to assess perfusion of mastectomy skin flaps, thereby possibly decreasing the risk of postoperative complications.
The DIEP flap can reliably transfer tissues across the abdominal midline in most patients. In some cases, perfusion is inadequate, most commonly manifesting as venous congestion. In these cases, the SIEV contralateral to the pedicle vessels can be anastomosed either to a branch of the DIEV or, more commonly, to the internal mammary vein. This may necessitate a vein graft. In other cases when the entire lower abdominal flap is needed for reconstruction, perforating vessels on both sides of the abdomen can be dissected, and both pedicles anastomosed to the internal mammary artery/vein in an anterograde/retrograde fashion. These so-called “stacked flaps” have excellent perfusion and facilitate the shaping of the breast to create ptosis or reconstruct large volume defects ( Fig. 36.7 ).
Once the flap has been harvested, it is weighed and transferred up to the chest for microvascular anastomosis. In most cases, a flap harvested from the contralateral abdominal wall is used since this orientation allows the pedicle vessels to run along the medial border of the chest and place the SIEV in close proximity to the internal mammary vessels, giving the surgeon the option of additional venous outflow or supercharging of the flap. However, an ipsilateral flap is also commonly performed if the perforating vessels in this area are superior in size/caliber as compared with the contralateral flap. In this case, the SIEV can easily be anastomosed to the axillary vessels if necessary. Following microvascular anastomosis, the flap is shaped and secured to the chest wall. Any twisting, kinking, or tension on the pedicle should be avoided. A skin paddle is usually left visible for postoperative flap monitoring, and the remainder of the flap is de-epithelialized. The skin is closed in layered fashion after placement of a closed suction drain.
The abdominal donor site is closed as outlined for the msTRAM. Mesh may be used as necessary if the fascia is attenuated or in patients with a prior history of abdominal operations. The abdominal wall may be plicated to improve the contour of the abdominal wall.
Postoperatively, patients are treated with an enhanced recovery after surgery (ERAS) protocol in which they are monitored for 4–6 hours in the recovery room and then transferred to a regular room. “Flap checks” are performed every 15 minutes for 1 hour, every 30 minutes for 2 hours and then every 1 hour for the next 24 hours. Patients are treated with subcutaneous heparin or Enoxaparin just prior to surgery and then daily for up to 1 month based on their risk of deep venous thrombosis as assessed by the Caprini Score. After discharge from the hospital, patients are asked to avoid strenuous activity, and lifting objects greater than 10 pounds for 6 weeks to prevent abdominal wall dehiscence.
Outcomes
Although some older studies had suggested that the DIEP flap may have a higher risk of partial flap loss and fat necrosis as compared with fTRAM/msTRAM, more recent studies suggest that the risk of these complications is similar in experienced hands and in properly selected patients. DIEP flaps also have lower rates of abdominal wall laxity and hernia as compared with fTRAM and pTRAM flaps. The pooled abdominal wall bulge/laxity/weakness rate reported in 11 studies with 930 DIEP flaps was 3.1%. This rate compares favorably with the pooled rate of 5.9% reported in 14 studies with 2015 fTRAM flaps. Similarly, the pooled rate of abdominal wall hernia in 10 studies reporting on 1529 DIEP flaps was 0.8% as compared to a rate of 3.9% in 18 studies reporting on 2609 msTRAM flaps.
Superficial Inferior Epigastric Artery (SIEA) Flap
History
The SIEA flap is an axial adipocutaneous flap based on the superficial inferior epigastric vessels and was first described in 1971 by Antia and Buch for the repair of a soft tissue defect of the face. Robert Allen Sr reported the first use of the SIEA flap for partial and total breast reconstruction.
Patient Selection
The SIEA flap has the same indications and contraindications as the DIEP flap. However, the use of this flap option may be limited by the caliber of the pedicle vessels, which are variable among individuals. These vessels can be analyzed preoperatively using imaging with CTA or MRA or with a handheld Doppler. In practice, the major indication for this flap is whether the superficial inferior epigastric artery is present, has a suitable size, and a palpable/visible pulse. The superficial inferior epigastric artery branches off of the common femoral or the superficial circumflex femoral artery and, when present, has a diameter of 1.1–1.9 mm. However, the artery has considerable anatomical variability and is absent in as many as 57% of individuals and, by some estimates, only adequate in diameter for microvascular anastomosis in fewer than 25% of cases.
Surgical Technique
The flap markings and patient setup are the same as for the DIEP flap. The procedure begins with the inferior skin incision just through the dermis, followed by careful dissection through the subcutaneous tissues to identify the SIEV. Deeper dissection, usually lateral to the SIEV and 4–7 cm from the midline, is performed through Scarpa’s fascia to identify the SIEA. If the SIEA is present and suitable for microsurgical anastomosis, the dissection is continued to the origin of the vessels, and the flap dissection is completed by ligating the DIEP perforators. Flap perfusion can be assessed prior to ligation of the DIEP perforators to ensure that adequate blood supply is present. If not, the SIEA is aborted, and a DIEP flap is elevated instead. The flap is then ligated, and microsurgical anastomosis is performed to the internal mammary vessels. The contralateral flap is preferred since this orientation places the pedicle vessels at the medial border of the flap, decreasing the risk of tension or kinking on the anastomosis. If an ipsilateral flap is chosen for the reconstruction, the flap is rotated 180 degrees to line up the SIEA/SIEV with the internal mammary vessels.
Great care is taken during insetting of an SIEA flap to avoid kinking of the pedicle vessels since these vessels are relatively short and exit the tissues more superficially than the pedicle for the DIEP flap ( Fig. 36.8 ). This anatomical orientation, particularly in obese patients with thick flaps, can result in a sharp turn of the pedicle vessels through the pectoralis muscle to reach the internal mammary vessels, making it more likely to kink or place the anastomosis under tension. The superficial nature of the pedicle in the SIEA flap also increases the possibility of compression by the mastectomy skin flaps as may occur in patients with a history of radiation. The breast and abdominal incisions are closed as described for the DIEP flap. The abdominal fascia may be plicated as necessary to improve the contour of the lower abdomen.

Outcomes
The primary advantage of the SIEA flap as compared to other abdominally based tissue options is lack of injury to the abdominal wall fascia or musculature. Patients treated with SIEA flaps have essentially no risk of abdominal wall hernia and retain abdominal core strength. However, this advantage is balanced by an increased risk of microvascular complications because the SIEA is usually smaller in diameter as compared to the DIEA and because the pedicle for the SIEA flap is relatively short. As a result, even experienced surgeons reporting large series of cases have reported total flap loss rates of 3%–5%; a number that is considerably higher than msTRAM or DIEP flaps. The rate of fat necrosis following SIEA flaps is also higher than other abdominally-based options due to the anatomical variability of the vascular supply of this flap.
Thigh-Based Flaps
While the abdominal donor site is an excellent option in many patients, this area may not be suitable in some individuals due to paucity of abdominal tissue, a history of previous abdominal surgery, or an aversion to abdominal scars. In these cases, tissues harvested from the medial or lateral thighs may be a good option.
Gracilis Flaps
Transverse Upper Gracilis (TUG)/Transverse Myocutaneous Gracilis (TMG) Flap
History
The transverse myocutaneous gracilis (TMG) or transverse upper gracilis (TUG) flap is the most commonly cited thigh-based flap used for breast reconstruction since its first description by Yousif et al in 1992. This flap is oriented transversely, extending anteriorly along the groin crease to the posterior midline of the thigh along the gluteal crease. This orientation is analogous to a medial thigh lift, and the blood supply to the flap is the gracilis pedicle, which is a branch of the profunda femoris artery. The pedicle for the flap is reliably found deep to the adductor longus muscle approximately 6–8 cm distal to the groin crease. Musculocutaneous perforators from the gracilis pedicle and septocutaneous perforators around the gracilis muscle provide perfusion to the skin and soft tissues of this flap.
Patient Selection
Gracilis-based flaps are good options for patients who are not candidates for abdominally-based flaps or would like to avoid the abdominal scar and have sufficient tissue of the medial and posterior thigh for breast reconstruction (i.e., patients with a pear-shaped body habitus). Poor candidates for the thigh donor site include those with peripheral vascular disease, severe venous insufficiency or history of deep vein thrombosis, and any unexplained swelling suspicious for primary lymphedema. Morbidly obese patients or those with large amounts of adipose tissues in the medial thigh areas are also poor candidates for gracilis-based flaps.
Surgical Technique
The groin crease and inferior gluteal fold are marked with the patient in the standing position. The superior border of the flap will be 1–2 cm below this line and should not extend beyond the posterior midline of the thigh. Anteriorly, the tip of the flap is located 2–5 cm anterior to the adductor longus muscle, which is easily marked with the patient in the frog-legged position. An ellipse is drawn to connect the anterior- and posterior-most portions of the flap after pinch test confirms the amount of tissue that can be harvested (reliably 6–8 cm). A conservative approach to flap width is essential, as this transversely oriented flap results in the greatest tension lines on closure. Excess tension can result in labial spreading and/or flattening of the inferior gluteal crease.
The patient is prepped and positioned in the frog-legged (or less commonly, lithotomy position). A two-team approach can be used for flap harvest, while the recipient vessels are being prepared or the mastectomies performed. The anterior portion of the flap is incised, and a superficial dissection proceeds posteriorly to avoid skeletonizing the greater saphenous vein and reduce the risk of lower extremity lymphedema. The adductor longus muscle is identified, and this fascia is incised throughout the width of the flap over the muscle, ensuring capture of septocutaneous perforators between the adductor longus and gracilis muscles. The adductor longus muscle is then retracted anteriorly revealing the gracilis pedicle. At this point, the pedicle can be easily dissected to its takeoff (6–8 cm). It is isolated circumferentially before the final skin incisions are made and the entire gracilis muscle is harvested. Care should be taken to avoid beveling to include greater volumes of the flap to improve the contour of the final donor site.
The ipsilateral flap is used for breast reconstruction with anastomosis to the internal mammary vessels. The flap is inset to the chest wall following microvascular anastomosis, leaving a skin paddle for postoperative monitoring. Patients are monitored postoperatively as noted above. Compressive garments are routinely applied over the donor site. There are no specific precautions besides avoiding trauma to the incision and strenuous activity until the donor site is well healed.
Outcomes
Excellent results and high patient satisfaction have been reported following TUG flap breast reconstruction; however, this flap does have limitations. These include a short pedicle, smaller flap size, limited skin available for reconstruction and muscle sacrifice. Aggressive harvest of this tissue is associated with wound dehiscence, labial spreading, poor cosmesis, and lymphedema with complication rates of up to 60% demonstrated in the literature. With this flap, the resulting incision on closure lies in the lines of greatest tension of the thigh. Thus, a conservative approach to tissue harvest is essential. Donor-site wound complications have been reported to be as high as 27%, with rates of labial spreading and a visible scar being 11% and 78%, respectively.
One devastating complication that can result following TUG flap harvest is lymphedema of the lower extremity. This can result from skeletonization of the proximal femoral vein in the anterior portion of the flap, where the major lymphatic drainage of the lower extremity is found. Lakhiani et al report limiting the anterior dissection in this area to avoid lymphedema and to prevent visibility of the incision from the frontal view. Despite these potential complications, up to 83% of patients report satisfaction following use of this flap for breast reconstruction.
Diagonal Upper Gracilis (DUG) Flap
History
To account for some of the limitations experienced with the TUG flap (see above), Dayan et al modified the orientation of the flap along Langer’s lines, calling it the diagonal upper gracilis (DUG) flap. The benefits of the orientation are an increased flap width along the lines of least tension, low risk of wound healing issues, and avoidance of the femoral triangle and the lymphatics vessels. Like the TUG flap, the DUG flap is based on the gracilis pedicle (medial circumflex femoral vessels). Patient selection is also similar to the TUG flap, with ideal patients being those with excess skin laxity and tissue of the proximal posteromedial thigh that are not candidates for, or prefer to avoid abdominally-based flaps.
Surgical Technique
The flap is a diagonally-oriented ellipse over the gracilis muscle in the proximal thigh. This orientation not only results in less tension on the incision but also captures the angiosome of the flap. The DUG flap is marked with the patient in the frog-legged position on the operating room table by first palpating the adductor longus (AL) prominence. The anterior incision is placed vertically along the posterior border of the AL muscle for approximately 10 cm, keeping the anterior border of the flap away from the draining lymphatics of the lower extremity. From here, the incision line is drawn posteriorly in a curvilinear fashion over the gracilis muscle. A pinch test determines the width of the flap, which is reliably 10–12 cm depending on patient body habitus and the posterior incision is marked connecting the proximal and distal aspects of the flap.
The proximal 10 cm of the anterior incision is made first with dissection proceeding down and through the AL fascia. The AL muscle is then distracted anteriorly revealing the gracilis pedicle. Pedicle dissection is quick, and the remainder of the incisions are performed following its isolation. The entire gracilis muscle is harvested with this flap. A straight-lined closure is performed over a closed suction drain. The closure is oriented in the resting skin tension lines and thus results in no postoperative mobility restrictions. Additionally, the area supplied by the obturator nerve is largely removed with harvest of the flap, resulting in little to no sensory loss to the patient.
Outcomes
Given the novelty of this flap, there is little data available on complication profile and long-term outcomes; however, Dayan and Allen Jr report a 6-year experience with over 60 DUG flaps, showing an excellent complication profile. In this series, flaps averaged 10.3 cm in width, ranging from 8 to 13 cm. One patient experienced 20% flap necrosis, and the overall incidence of donor-site complications was 10%.
The main disadvantages of the DUG flap include a visible posterior scar, short pedicle (6–8 cm), muscle sacrifice and a smaller flap to use for breast reconstruction. Atrophy of the gracilis muscle with time can also result in shrinking of the flap, though this can be minimized with primary fat grafting of the gracilis during breast reconstruction or stacking the flaps for a unilateral reconstruction ( Fig. 36.9 ). Overall, this flap is technically easy to perform, provides a reliable blood supply and can result in excellent satisfaction in the appropriately selected patient.










