Introduction
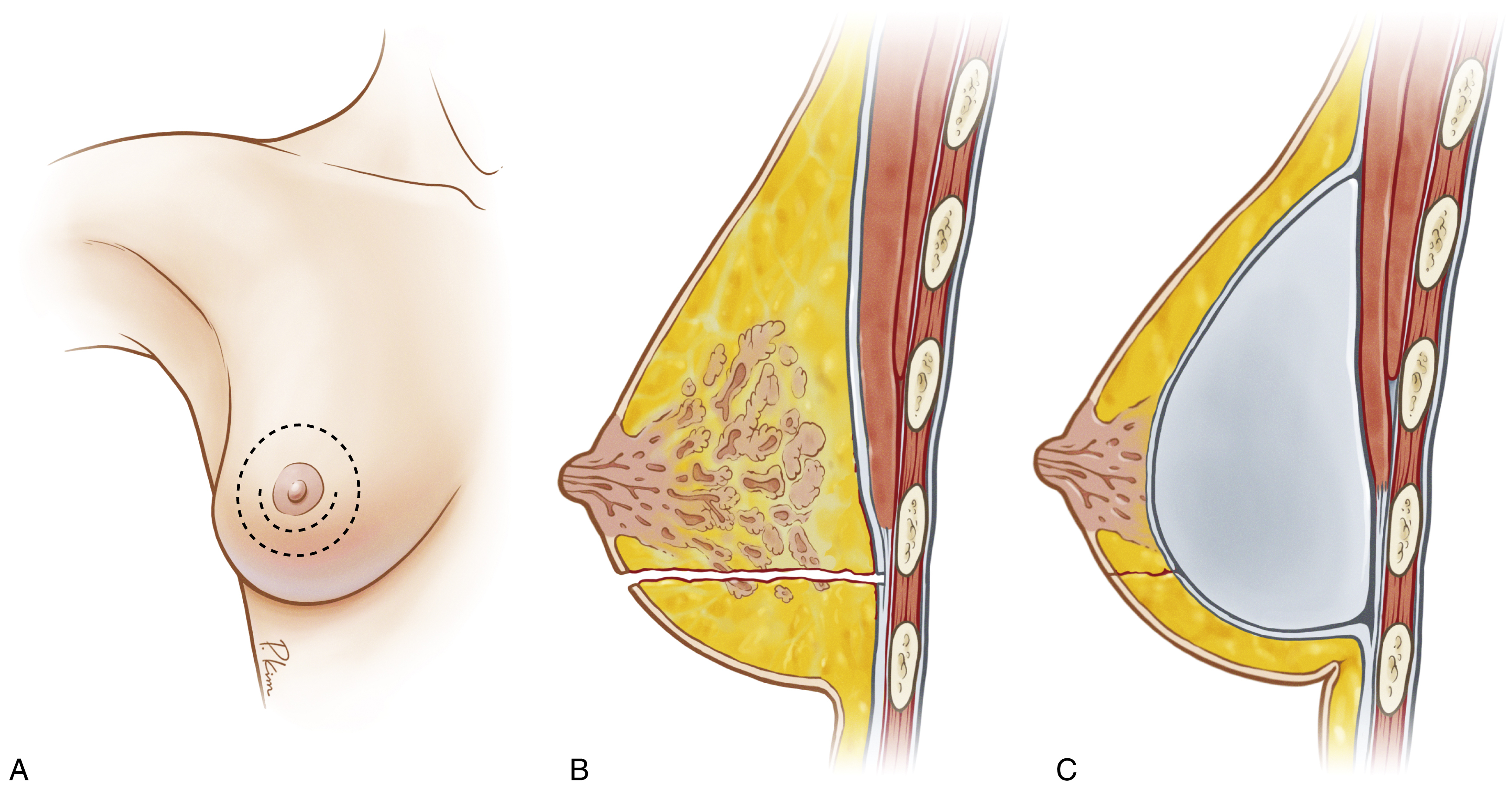
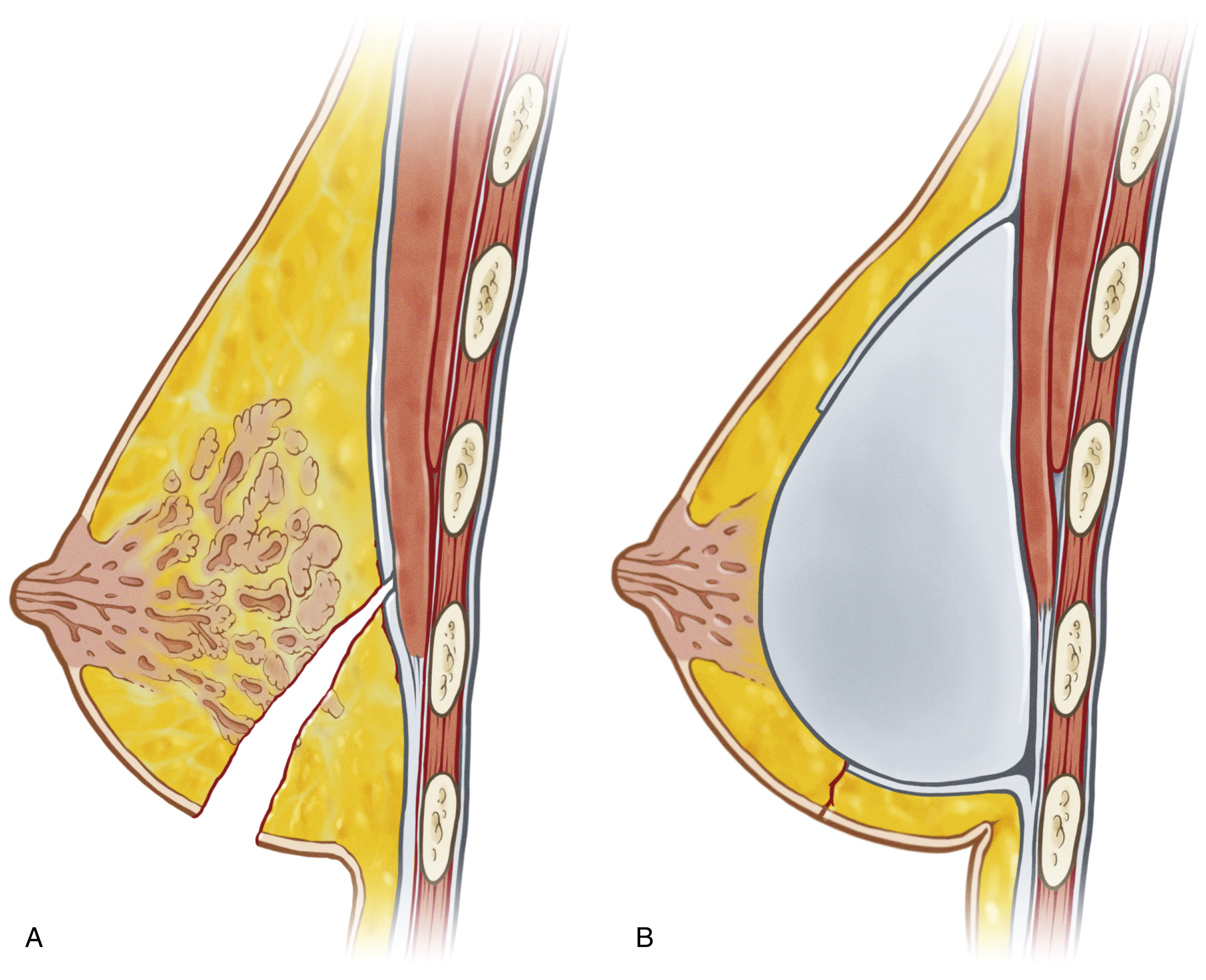
The pectoral fascia is a thin layer of dense connective tissue, covering the surface of the pectoralis major muscle. It can be easily dissected along the subfascial implant insertion. The pectoral fascia helps support the breast implant, and even in slim patients a smoother transition is achieved in the breast upper pole if the fascia is firmly attached to the muscle.
Various approaches can be used to perform a subfascial breast augmentation (transaxillary, inframammary fold [IMF], periareolar, vertical, and short horizontal incisions), which makes this technique more versatile. Capsular contracture seems to be less frequent in subfascial placement compared with the subglandular pocket, probably because of a higher vascularized tissue (pectoralis major muscle).
Subfascial implant placement avoids the negative aspects of a submuscular pocket (animation deformity) and provides a shorter recovery. In this chapter the authors describe their technique on subfascial breast augmentations, including indications, operative techniques, postoperative care and expected outcomes, management of complications, and secondary procedures for revisions.
Indications and Contraindications
Any size and shape of implants can be used in subfascial breast augmentation cases and all kinds of approaches, depending on whether the procedure is only breast augmentation or mastopexy augmentation. There are no contraindications for this technique because of the maneuver of muscle coverage superomedially and fat transfer if necessary to avoid rippling in slim patients.
Patients with tuberous breasts usually present with lower pole hypoplasia and some degree of nipple–areola complex weakness and prolapse. In these cases, a subfascial pocket is created, the fascia is incised radially in lower pole, and fat can be added in this region to allow shape improvement.
Secondary mammaplasty that is primarily subglandular can be performed, removing the anterior capsule and elevating the fascia and posterior capsule to create a new pocket for the new implant. If the implants were submuscular primarily, a new subfascial pocket is created in the secondary procedure.
Preoperative Evaluations and Special Considerations
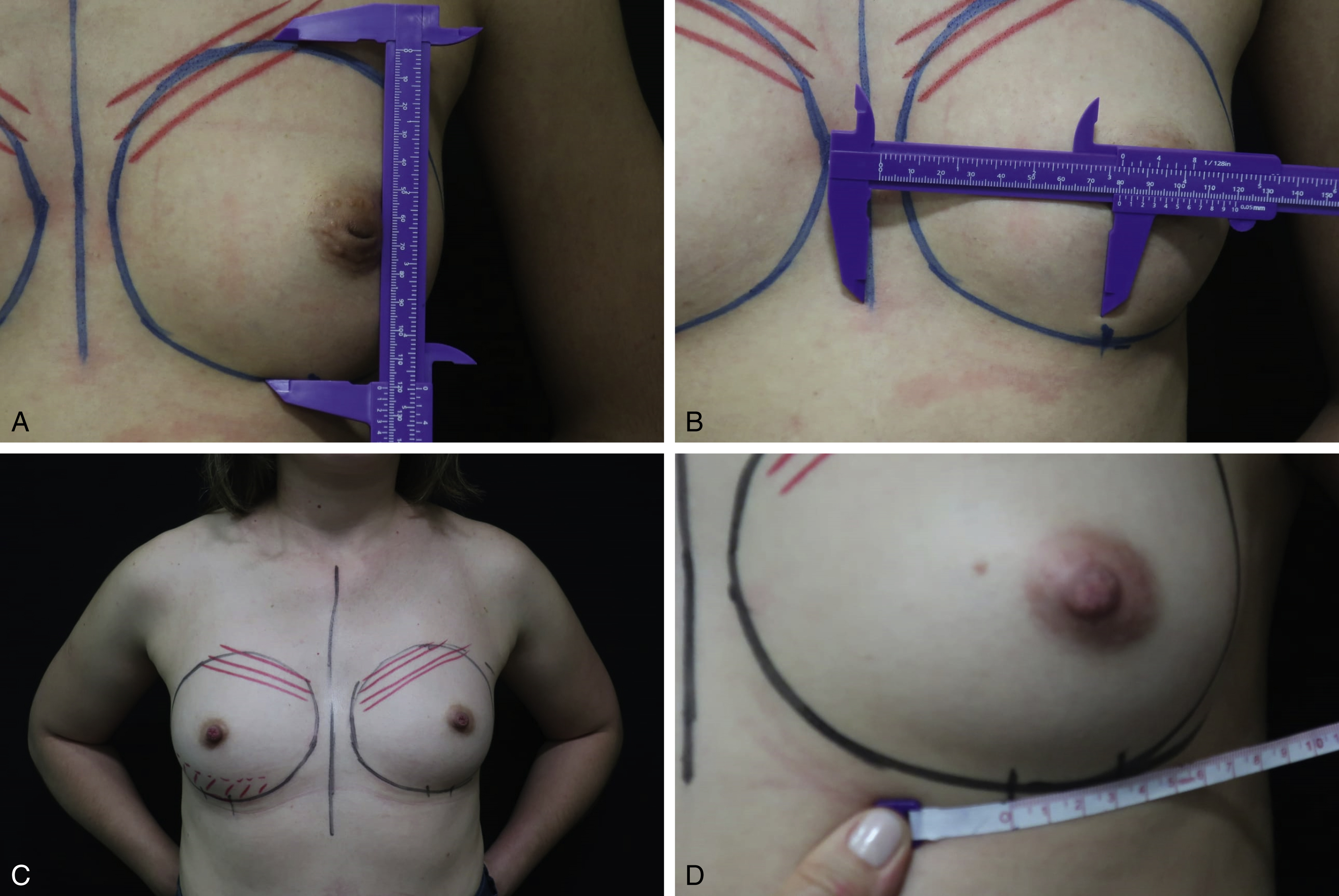
All patients can be provided a subfascial implant placement, especially thin patients. Ideal primary patients have hypomastia, no ptose, and the presence of a soft tissue envelope to cover the implant. In very slim patients with absence of soft tissue coverage, subglandular placement is difficult. In these cases, a spreader maneuver is done in the muscle fibers at the superomedial pole of the breast and in some cases fat transfer is done, as shown in Figs. 4.1; 4.2A, B; and 4.3 . It is also important to measure breast height and base to properly choose the implant volume.
Breast augmentation mammaplasty and breast augmentation mastopexy cases can be performed with a subfascial implant pocket.
Differences in breast sizes usually can be handled by using different implant volumes. Adding fat in the smaller breast at the end of the procedure can be helpful if similar implants are used. When concomitant mastopexy is performed, excessive tissue from a larger breast can be resected and a similar size of implants can be used.
Cases of mild to moderate tuberous breast can be managed properly with a transaxillary or inframammary breast augmentation. However, more severe cases must be treated with mastopexy techniques (e.g., periareolar breast augmentation).
Radial incisions in the fascia should be performed to smooth the fibrous ring and improve breast contour. Fat transfer to the lower pole can be done at the end of the procedure.
Slim patients are very challenging because of the absence of adequate tissue coverage. Some muscle fibers (pectoralis major muscle) can be elevated with the fascia in the superior part of the pocket to create a smoother transition in the upper pole breast. Fat grafting can be done to camouflage rippling (composite breast augmentation).
Surgical Techniques
Relevant Surgical Anatomy
The pectoral fascia is a dense connective tissue that originates from the clavicle and sternum, covers the pectoralis major muscle, and continues down with rectus abdominis fascia. It can be bluntly dissected along the subfascial plane and has some specific characteristics.
At the second rib level, the pectoral fascia tightly connects with the superficial fascia of the breast, and it is difficult to dissect the pocket. This is usually the upper undermining point, which defines breast limits.
Along the point that corresponds to the fourth intercostal space, a horizontal septum originating from pectoral fascia connects with the nipple. This septum is a guide to dissection, especially in infraareolar and periareolar mammoplasties and mastopexies cases.
The pectoral fascia is a well-defined anatomic structure made of dense and consistent connective tissue. It can be used to minimize implant edge appearance and make the breast implant less noticeable. A subfascial pocket can be used even in slim patients.
Preoperative Markings
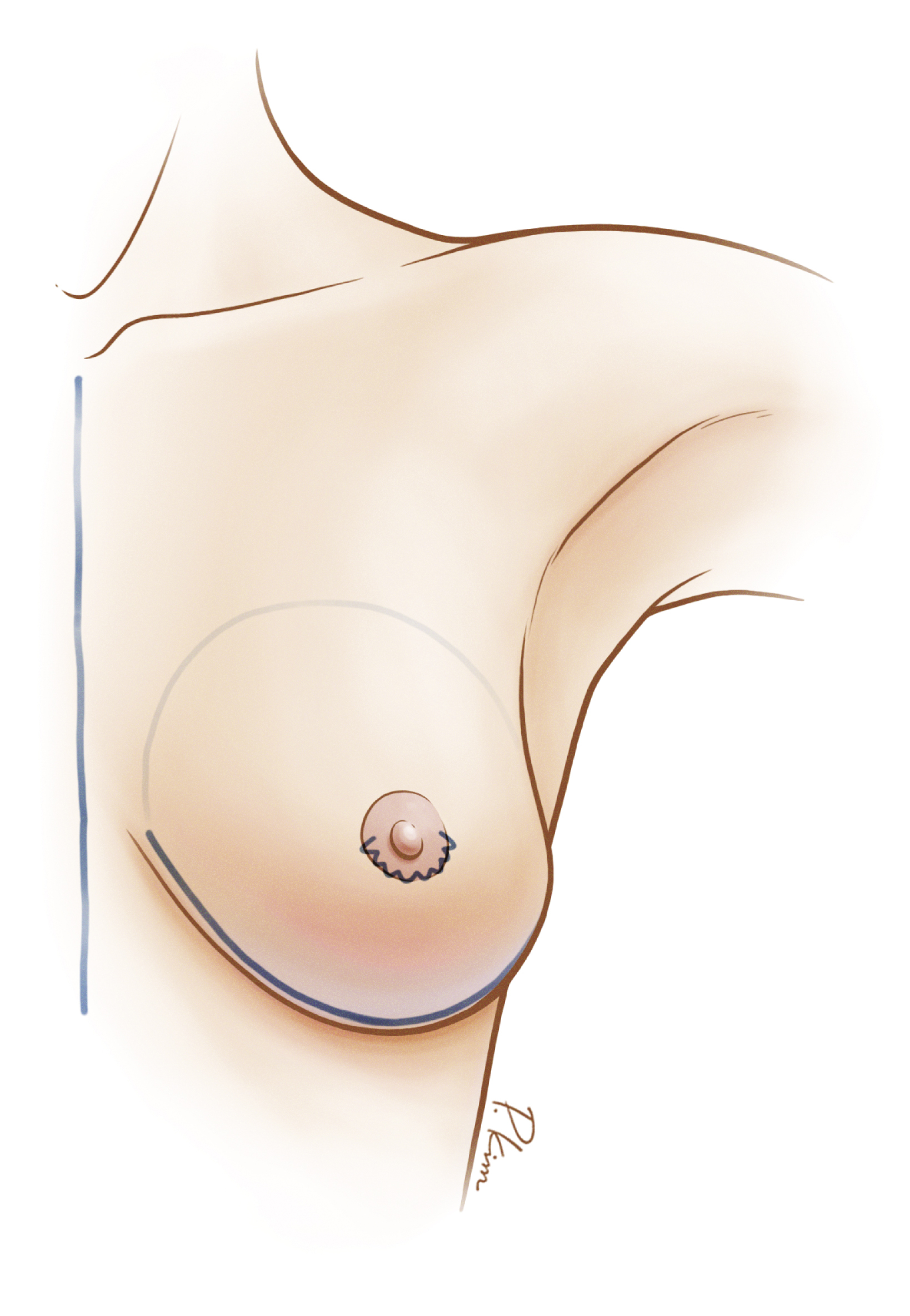
Skin markings are done with the patient standing. The pocket footprint (breast limits) is marked. Precise measurements must be taken using the inframammary fold (IMF), the nipple–areola complex, and the suprasternal notch as key landmarks. The midline of the chest and IMF are marked. Lines are drawn first straight down the midline from the suprasternal notch to the xyphoid process and second from a point 5 cm from the suprasternal notch at the clavicle to the nipple–areola complex and then straight down to the areola. The incision is marked depending on incision choice. In breast augmentation mammaplasty (transaxillary, infraareolar, and inframammary incision), the nipple–areola complex placement does not change, different from mastopexies (periareolar, vertical, and inverted T), in which the nipple–areola complex distance is elevated to correct ptosis ( Fig. 4.4A–C ).
Surgical Techniques
After incision, subfascial pocket undermining should be done very carefully to avoid fascia injury, and, if there is doubt about its limits, some muscle fibers may be lifted up with the fascia. Currently, an electrocautery device with a thin tip is used to undermine the pocket.
Upward traction is necessary to make dissection easier and more precise. Limits for dissection are the second intercostal space superiorly, 1.5–2 cm from midline medially, 5–7 cm below the areola to the new IMF (or the actual IMF, respecting its limits), and to the anterior axillary line laterally.
The distance between pocket implants should not be less than 2–3 cm to prevent symmastia. Lateral undermining is minimal to prevent implant lateralization. Some muscle fibers (pectoralis major muscle) can be elevated with the fascia in the superior part of the pocket, incising between the fibers to create a smoother transition in upper pole breast.
Once dissection is completed, meticulous hemostasis is performed and the implant is inserted into the pocket. Fascia can be sutured with absorbable suture (  ).
).
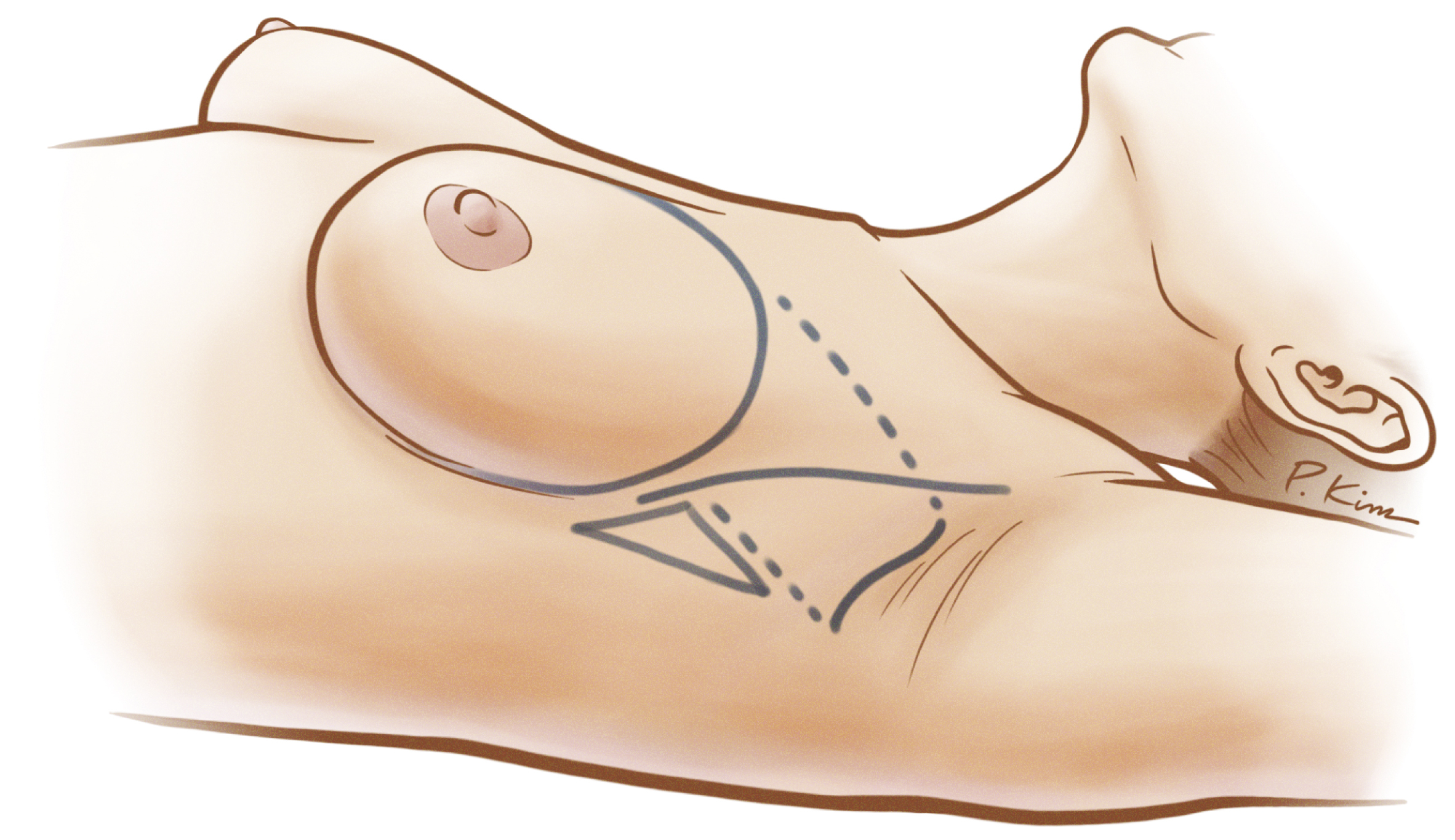
Axillary Approach for Subfascial Augmentation
The axillary incisions are placed in a natural crease. An S-shaped, 4-cm-long incision is made in the main axillary fold 1 cm behind the lateral border of the major pectoralis muscle. It is important never to cross beyond the lateral edge of the pectoralis muscle. A subcutaneous tunnel is dissected up to the superior lateral border of the muscle, preserving an inferior lateral triangle of soft tissue containing most of the lymphatic vessels, as we can observe in Fig. 4.1 .