Introduction
Breast augmentation using implants has been an important part of plastic surgery practice since the first breast implant was developed in 1963. More recently, some leading plastic surgeons have promoted an inframammary fold (IMF) approach when placing a breast implant. They think this method minimizes implant contact with breast tissue that could be contaminated by bacteria. If contamination can be avoided, the risk of biofilm formation is decreased and theoretically the complications of capsular contracture and the development of breast implant associated–atypical large cell lymphoma (BIA-ALCL) might be diminished.
However, many surgeons and patients continue to prefer a periareolar incision because visualization of the surgical field is optimized, and the resulting scar, hidden in the color change between the areola and the breast skin, is well camouflaged. The periareolar is my preferred incision and, over the past almost 30 years of practice, has resulted in no cases of BIA-ALCL, one peri-implant infection, and a grade 3–4 capsular contracture incidence of less than 1%.
This chapter details my preferred approach for periareolar breast augmentation, including preoperative evaluation and special considerations, the operative technique, postoperative care, and secondary procedures. Pearls for success are also discussed.
Indications and Contraindications
Ideal candidates for periareolar breast augmentation are healthy patients with no breast pathologic conditions present. The patient should have reasonable desires and expectations, and the patient’s anatomy and degree of symmetry should provide an adequate basis for a successful outcome. The patient should understand the risks and benefits of breast implants and the need for ongoing surveillance for breast health.
Patients who are poor candidates for breast augmentation are those with co-morbidities that increase the risk of complications and those with unrealistic expectations. Patients who cannot comprehend the risks or who are unwilling to return for long-term follow-up should be dissuaded from surgery.
Patients desiring implant volumes that cannot be supported by their anatomy are educated regarding the negative sequelae of overly enlarged breasts.
Preoperative Evaluation and Special Considerations
A patient desiring implant augmentation is evaluated with regard to overall health and particularly breast health. If the woman is of an age at which screening mammography is indicated, testing is performed preoperatively. I want to query the patient on her family history of breast cancer. I also want to know her childbearing history and whether she has plans for any additional children and breastfeeding.
Suitable candidates undergo breast examination to determine the quantity and quality of the breast tissue, skin thickness, and quality; the position of the nipple–areolar complexes; and the base diameter of the breasts. Any asymmetries of breast volume, breast mound location, breast width, nipple position, and areolar diameter are documented and discussed with the patient.
The patient is then informed of the range of implant sizing available for her, with the largest size being a high-profile implant that matches her base diameter. I refuse to place implants larger than recommended, because I think they create unnatural appearing breasts and do not provide good long-term results.
In my opinion, women with a strong family history of breast cancer should be steered toward submuscular saline implant augmentation so that future mammographic clarity is optimized. A patient with breast size asymmetry is counseled that the smaller breast is the “limiting factor.” Although she may desire the largest implant that will “fit” the smaller or narrower breast, the implant for the larger breast will have less volume, with the goal of improved symmetry between the two breasts. My opinion is that women who have not completed childbearing should be encouraged to forego augmentation until after the final pregnancy and to have ceased breastfeeding for at least 4 months before augmentation. Women desiring augmentation before completing childbearing are informed of the possibility of pregnancy- and breastfeeding-induced changes to the appearance of the breasts that might require additional maintenance work in the future. I inform them that breast augmentation may affect a woman’s ability to breastfeed, although many of my patients who have undergone periareolar breast augmentation have successfully breastfed.
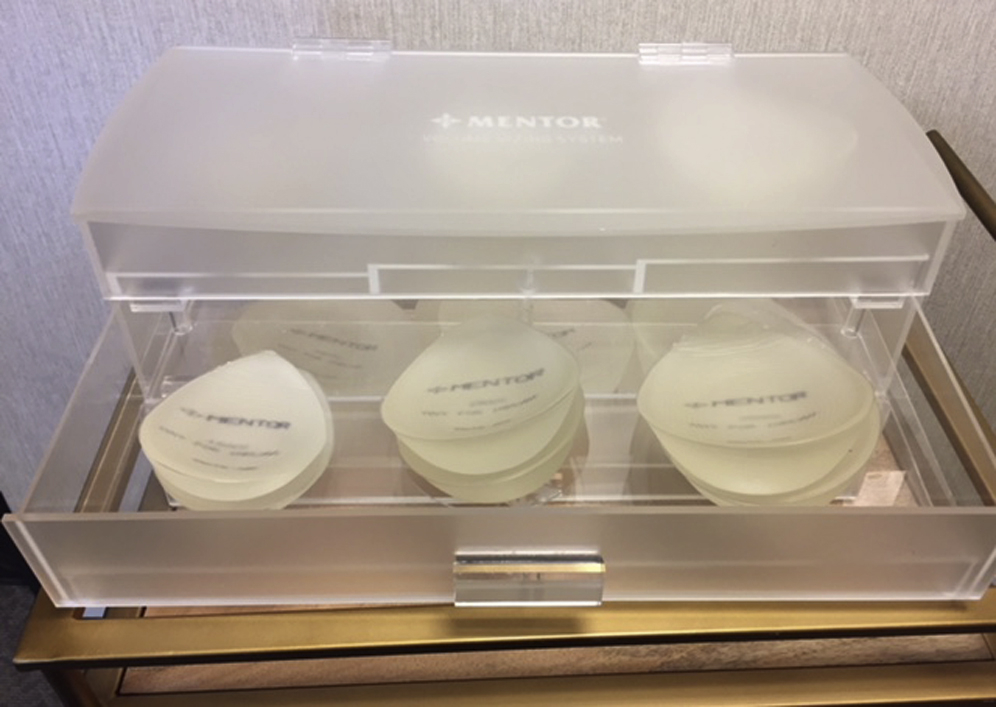
After the breast examination and discussion of the details of augmentation surgery and postoperative care, I have the patient use the Mentor sizing system of silicone breast forms placed within a soft bra ( Fig. 2.1 ). I inform her of the range of sizes she can consider based on her breast base diameter. When the patient finds a size she likes in a bra, I ask her to also put on her shirt (we also provide snug tank tops) so she can see how she will look in clothes. This sizing by the patient helps guide me in visualizing her goal. I inform the patient that I will be guided by the implant size she has picked, but I will use sterilized “sizers” in the operating room to verify the appropriate volume, and that I may alter the implant size somewhat from her original choice to ensure a favorable result.
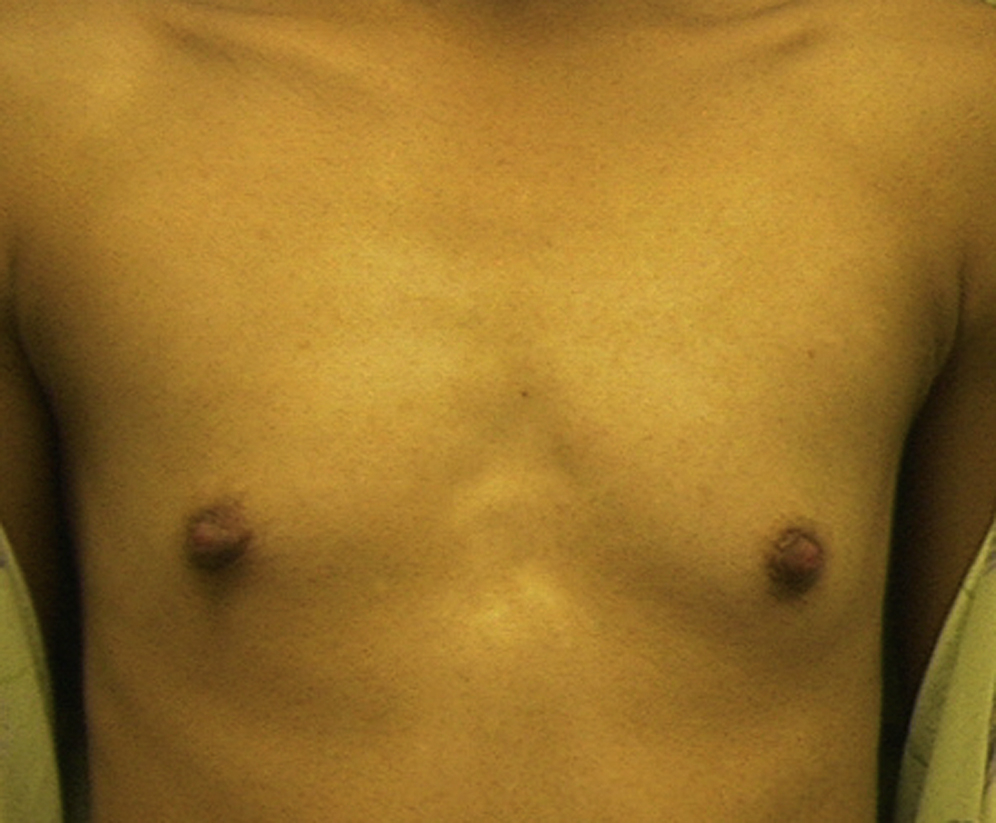
If the patient presents with a small areolar diameter (less than 3 cm) through which an implant cannot be easily placed, I inform her of the need to opt for an IMF approach ( Fig. 2.2 ).
Surgical Technique
Although breast augmentation is often performed under general anesthesia, I prefer to perform breast augmentations using local anesthesia and intravenous sedation. This is more economical for the patient and is quite comfortable. The patient is sedated with a combination of midazolam and morphine sulfate, and then rib blocks are placed using 0.25% bupivacaine with 1:200,000 epinephrine, approximately 10 mL per side ( Fig. 2.3 ).

After prepping and draping, the planned periareolar incision line is drawn, taking care to be right along the edge of the areola. The incision runs from 3 o’clock to 9 o’clock in smaller areolae and from about 4 o’clock to 8 o’clock in areolae that are more generous. The natural borders of the breast are marked circumferentially to guide the dissection ( Fig. 2.4 ). Local anesthetic consisting of ¼% lidocaine with 1:400,000 epinephrine is injected into the incision line and then used throughout the procedure to maintain comfort for the patient.

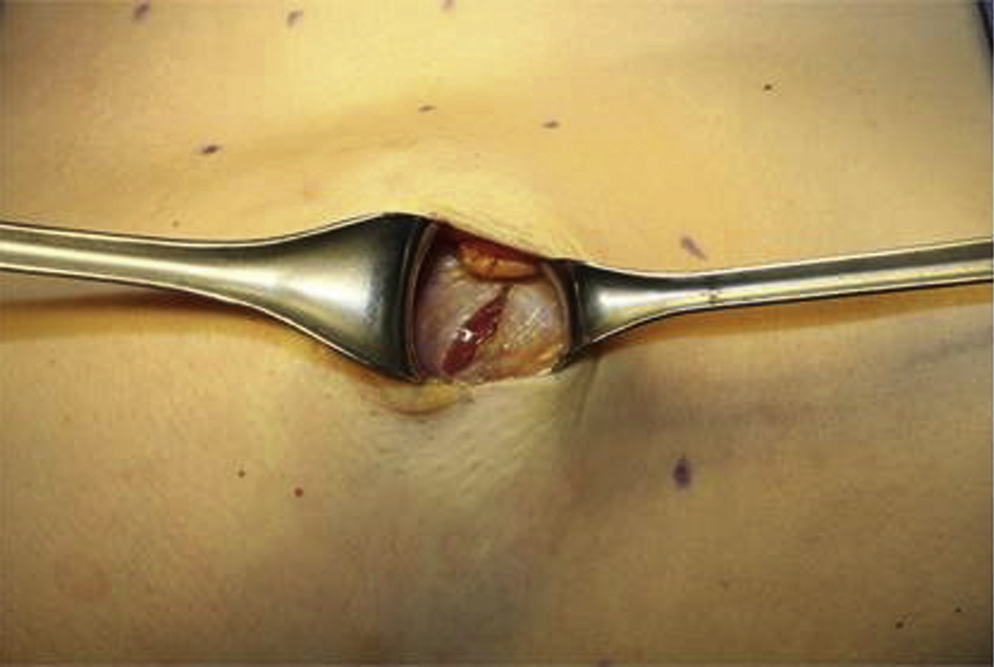
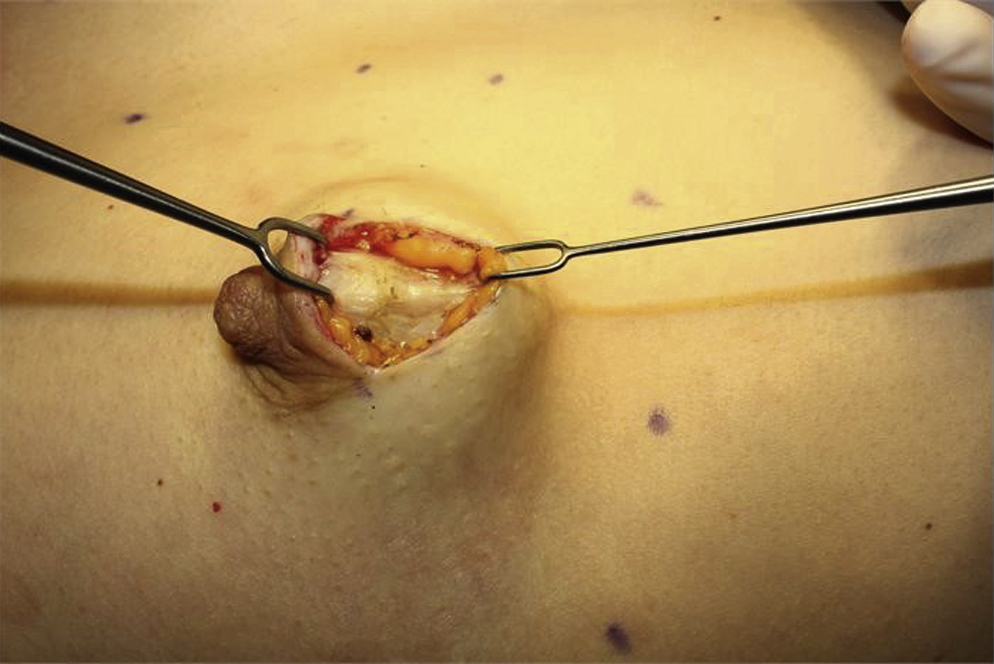
The incision is created, and all superficial bleeding vessels are cauterized with a needle-point cautery. Double skin hooks are placed on either side of the incision, and the underlying tissue is divided with the electrocautery on cutting mode ( Fig. 2.5 ). Skin hooks may need to be replaced with small to medium Richardson retractors to expose the base of the dissection. Dissection is carried straight down through the breast tissue to the pectoralis fascia in most patients ( Fig. 2.6 ). However, in nulliparous women the subcutaneous dissection is aimed obliquely toward the IMF to reach the lower border of the pectoralis. This dissection minimally disrupts the breast tissue connections to the nipple ducts, with the goal of preserving the ability to breastfeed later on.

Once the dissection reaches the pectoral muscle, the pectoralis fascia is incised with the electrocautery ( Fig. 2.7 ). The fascia and muscle are then grasped with Allis clamps on either side of the muscle fiber line. Gently pulling the clamps upward, the muscle is divided in the direction of the muscle fibers, obliquely, until the loose areolar tissue of the submuscular space is encountered ( Fig. 2.8 ). If the muscle is thick, the Allis clamps may need to be repositioned deeper to improve visualization.