Introduction
Breast augmentation is one of the most popular aesthetic procedures worldwide, including in Asia. The unique Asian cultural background, which is more conservative, influences various options for Asian breast augmentation. Many Asian women prefer an axillary incision to inframammary fold (IMF) incision because they do not want others to notice any scar on their breasts when they are in a public bath, swimming pool, or any other public places. From the ethnic perspective, Asian skin is darker than Caucasian skin and has a higher risk of hypertrophic and hyperpigmentation scarring.
The axillary approach has been questioned because of the blind, inaccurate, and bloody dissection. However, with the help of endoscopy, the axillary approach can have clear visualization and precise dissection, ensuring much better results than blind dissection. It has been demonstrated that axillary approach breast augmentation is a safe technique that has no impact on sentinel lymph node detection. If the dissection is appropriately performed, there is minimal chance of damaging the nerves and vessels. The periareolar incision is infrequently used, mainly because of the risk of changes in nipple–areolar sensibility, interference with milk ducts, and therefore possible bacterial contamination of implants.
In this chapter we discuss two dominant primary implant breast augmentation techniques in an Asian population: silicone implant subpectoral breast augmentation via IMF incision and endoscopy-assisted axillary incision.
Indications and Contraindications
IMF incision is suitable for almost all cases, especially for the difficult ones such as those involving ptosis, low pole constriction, and complicated revision surgery.
Axillary incision is preferred for patients who wish to hide the scar away from the breast. There are some limitations for this incision, so the relative contraindications are as follows:
- •
Severe breast ptosis needing mastopexy
- •
Lower pole constriction/short nipple-to-fold distance and need to stabilize new IMF
- •
Tubular breast
- •
Snoopy nose deformity
- •
Complicated breast revision cases (IMF approach needed)
Preoperative Evaluation and Special Considerations
Patients who seek breast augmentation have an extended consideration period and have collected much information on the internet. Sometimes, the more information they have, the more unrealistic their expectation can be, and the more confused they are due to “Dr. Google.” Patients should be informed about all the surgical procedures and details, including all the possible complications and risks. The formal consent form should be signed after all consultations.
A careful history and physical examination should be applied when approaching prospective breast augmentation patients. Meticulous attention should be given to the following:
- •
In evaluating breast development, the surgeon should inspect both breasts for symmetry, checking contour, fullness, nipple–areola position, the relationship between the position of the areola complex and the IMF, the relative relationship between breast and chest wall, and the distance to cleavage; and examine for musculoskeletal abnormalities such as scoliosis and soft tissue abnormalities (mass or nodule).
- •
Either obvious or subtle, asymmetries should be noted and explained to patients, ensuring that they are aware of all the details about their breast and chest wall beneath it.
- •
Pregnancy and breastfeeding history and breast mammogram history should be recorded.
Preoperative Measurement and Markings
Detailed measurements are necessary for both patients’ communication and making a surgical plan. Most importantly, dimensions of the breast can give surgeons guidance to choose the right implants for optimal results. Here we classify all the essential dimensions into two groups: measurement for education (aims to help patients to know more about their breast and understand the results) and measurement for surgical planning ( Table 5.1 ).
| Measurement for Education | Measurement for Surgical Planning |
|---|---|
| BW | BW |
| SN-N | SN-N |
| C-N | MSS |
| N-IMF | C-N |
| N-N | PT |
| N-M | N-IMF |
| DAC | |
| PT | |
| MSS | |
| D-NS | |
| D-IMFS |
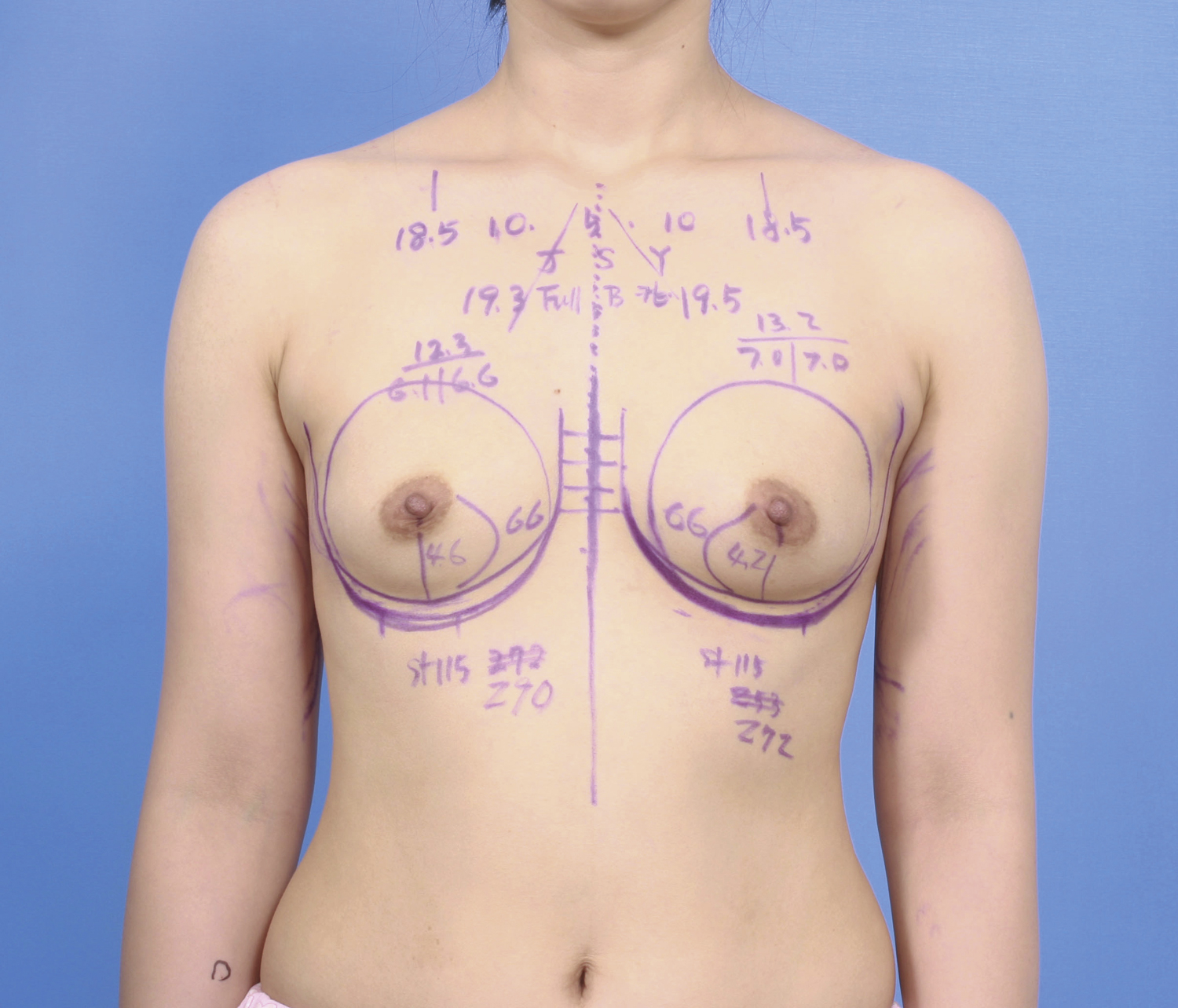
All those measurements should be informed to patients and recorded in the medical chart. Based on the individual breast dimensions, proper implants should be selected to match the patient’s expectation and to ensure the safety of the long-term follow-up. The measurement and marking should be performed in a standing position, and all the essential measures can be placed on patients’ breasts before the surgery ( Fig. 5.1 ).
Surgical Technique
Subpectoral Breast Augmentation via Inframammary Fold
Relevant Surgical Anatomy
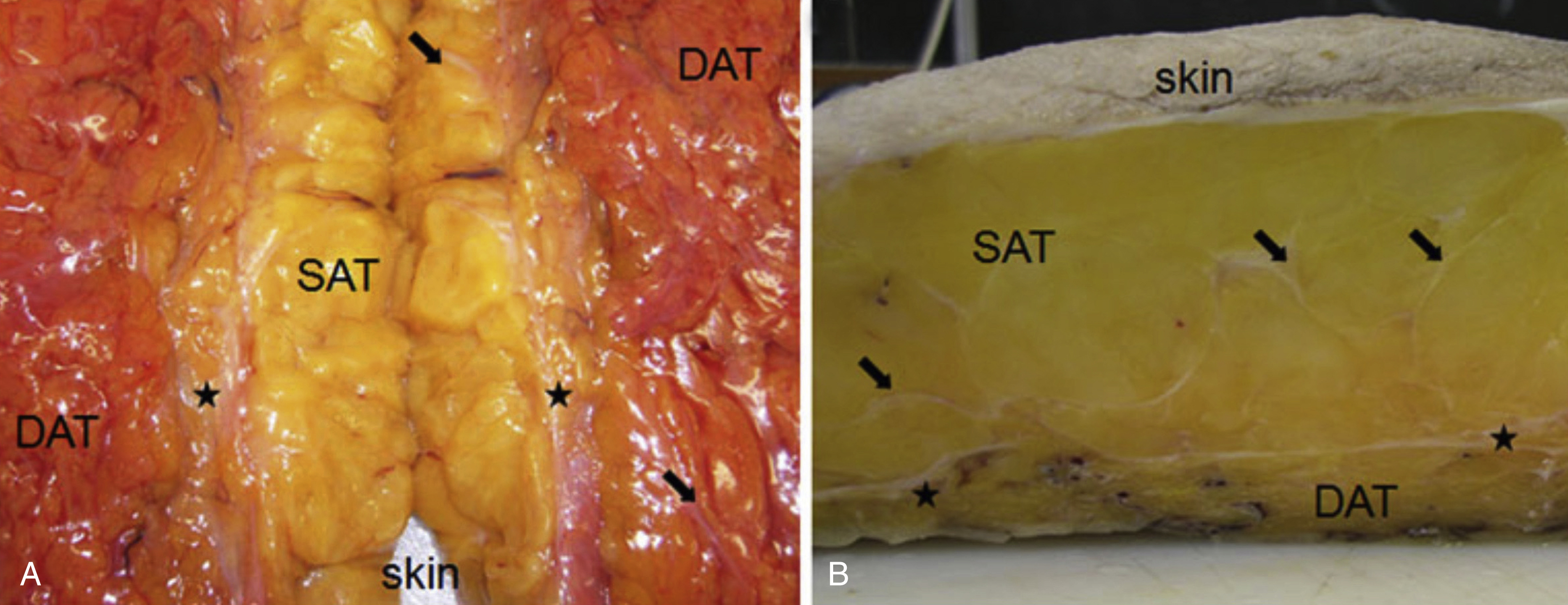
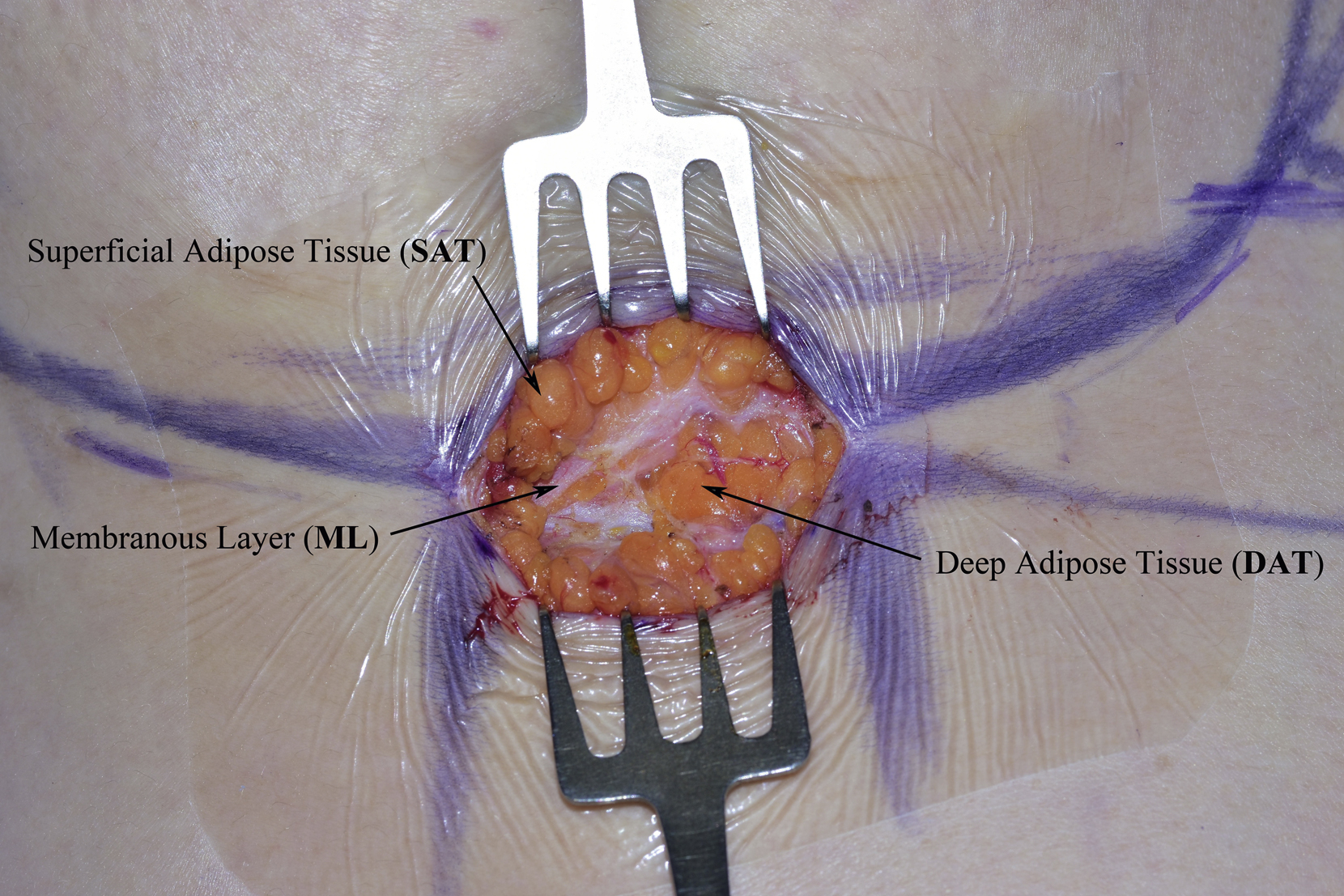
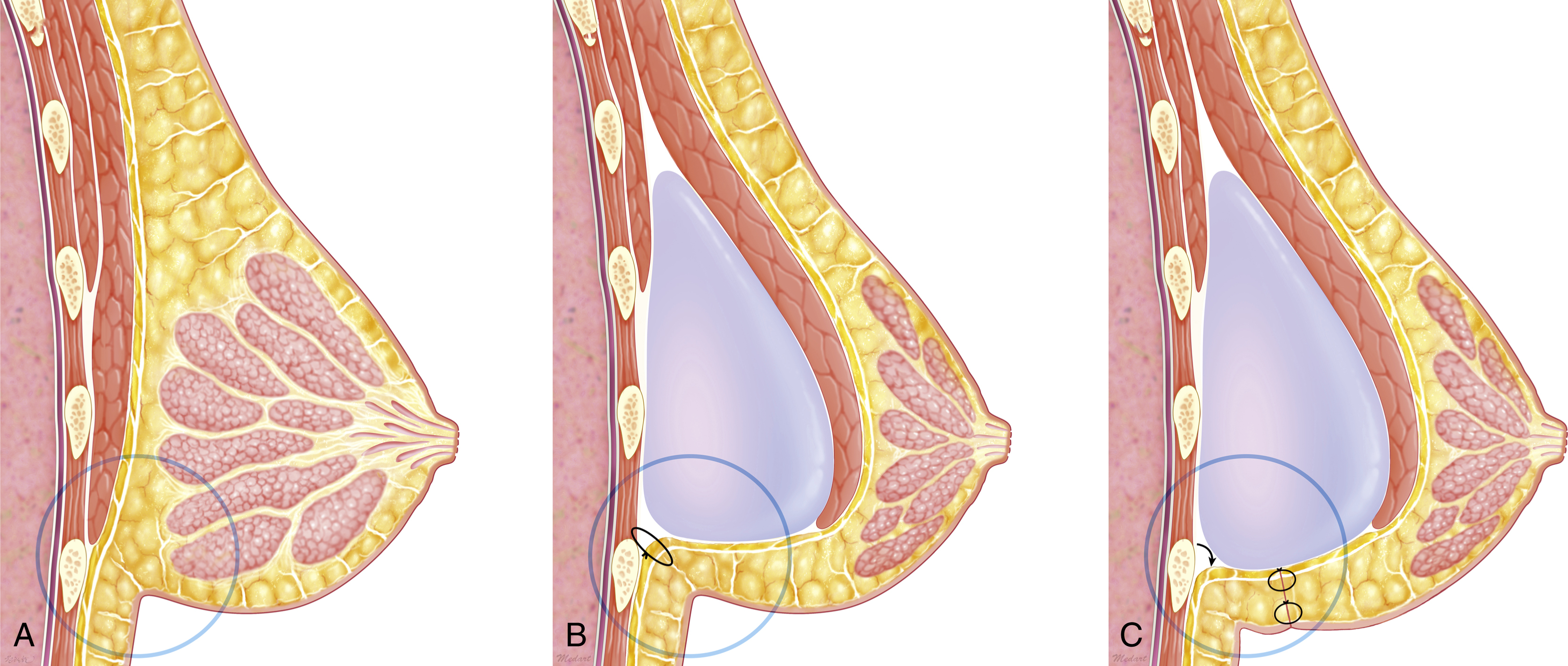
Lancerotto et al have described that there are three layers of abdominal subcutaneous adipose tissue: a superficial adipose tissue (SAT), a membranous layer (ML), and a deep adipose tissue (DAT) ( Fig. 5.2 ). The SAT is made of large fat lobes encased in fibrous septa in a honeycomb-like structure and has nearly constant characteristics throughout ( Fig. 5.3 ). These septa (retinacula cutis superficialis) appeared well defined, mostly oriented perpendicular to the surface, and mechanically strong, anchoring the dermis to the deeper planes. The DAT is flatter, less well defined, and has smaller fat lobes, and the fibrous septa (reticular cutis profunda) were less consistent and mostly obliquely oriented. These septa permit lateral displacement readily, the mechanical strength of these septa is weak, and they permit lateral sliding. The breast gland is an ectodermal origin structure contained in a superficial adipose tissue, in which strong reticular cutis superficialis hold up the breast gland between the ML and the dermis at the IMF level without herniation. Without the fixation of the ML and SAT to deep fascia, the DAT layer can be separated easily with the loosening of the reticular cutis profunda by weight of the implant in a wedge-like fashion, in which case, there is a possibility of bottoming out of the implant. It is the main reason why new IMF line should be reconstructed with a fixation method in breast augmentation with implant regardless of incision choice. Without the fixation, the chance of inferior malposition of implant always exists, especially with smooth-surfaced implants and even microtextured implants ( Fig. 5.4A–C ) .
Preoperative Markings
Placement of the incision location precisely in the new IMF is the key factor to better aesthetic outcome. Thus labeling the new IMF and identifying the incision location is vital before undergoing surgery. The breast width, the type of breast implant selected, the pocket location, the strength of the fibrous connections around the existing IMF, and the degree of the breast ptosis should all be considered when redefining the new IMF and incision. The author’s personal preference is to use Charles Randquist’s formula because it is simpler and easier to follow and practice than others, which mainly based only one crucial factor: the breast implant width ( Table 5.2 ). The IMF incision should be placed in the darkest area under the shadow of the breast mound on standing position. The length of the incision will be 4–5cm, depending on the implant size.
| Breast Width (BW) | 11.0 cm | 11.5 cm | 12.0 cm | 12.5 cm | 13.0 cm |
| New N-IMF | 7.5 cm ± 0.5 cm | 8.0 cm ± 0.5 cm | 8.5 cm ± 0.5 cm | 9.0 cm ± 0.5 cm | 9.5 cm ± 0.5 cm |
| Fine Adjustment | +0.5 cm | Tight skin > 2–4 cm pinch test > Lower pole fullness | |||
| –0.5 cm | Loose skin > upper pole fullness |
Surgical Procedure
After the surgical preparation, two critical steps should be performed to prevent contamination: use of nipple shields and use of an incision shield with sterile transparent film. Because the breast is of ectodermal origin, the nipple can be a continuous bacterial dissemination focus during the operation even with bactericidal skin preparation. Use of an incision shield on the IMF incision can protect incision margin skin injury and minimize the risk of implant contamination during the insertion process.
- 1.
Skin incision
The incision should be made deep to superficial dermis along the new IMF with a scalpel and shift to monopolar needle electrocautery to avoid unnecessary bleeding.
- 2.
Dissection through subcutaneous fat to expose the pectoralis major muscle
The surgeon should continue to dissect through the dermis and subcutaneous fat, straight down to the muscle layer. Make sure that all the dissections are quick, neat, and vertical to the skin surface. For this purpose, retraction of both chest flap and abdominal flap with retractor should be without traction, in order not to deviate up or down. Once the musculature is visible, the surgeon should check, locate, and identify the pectoralis major muscle carefully. The muscles at this level are the pectoralis major muscle, rectus abdominis muscle, external oblique muscle, serratus anterior muscle, and intercostal muscles.
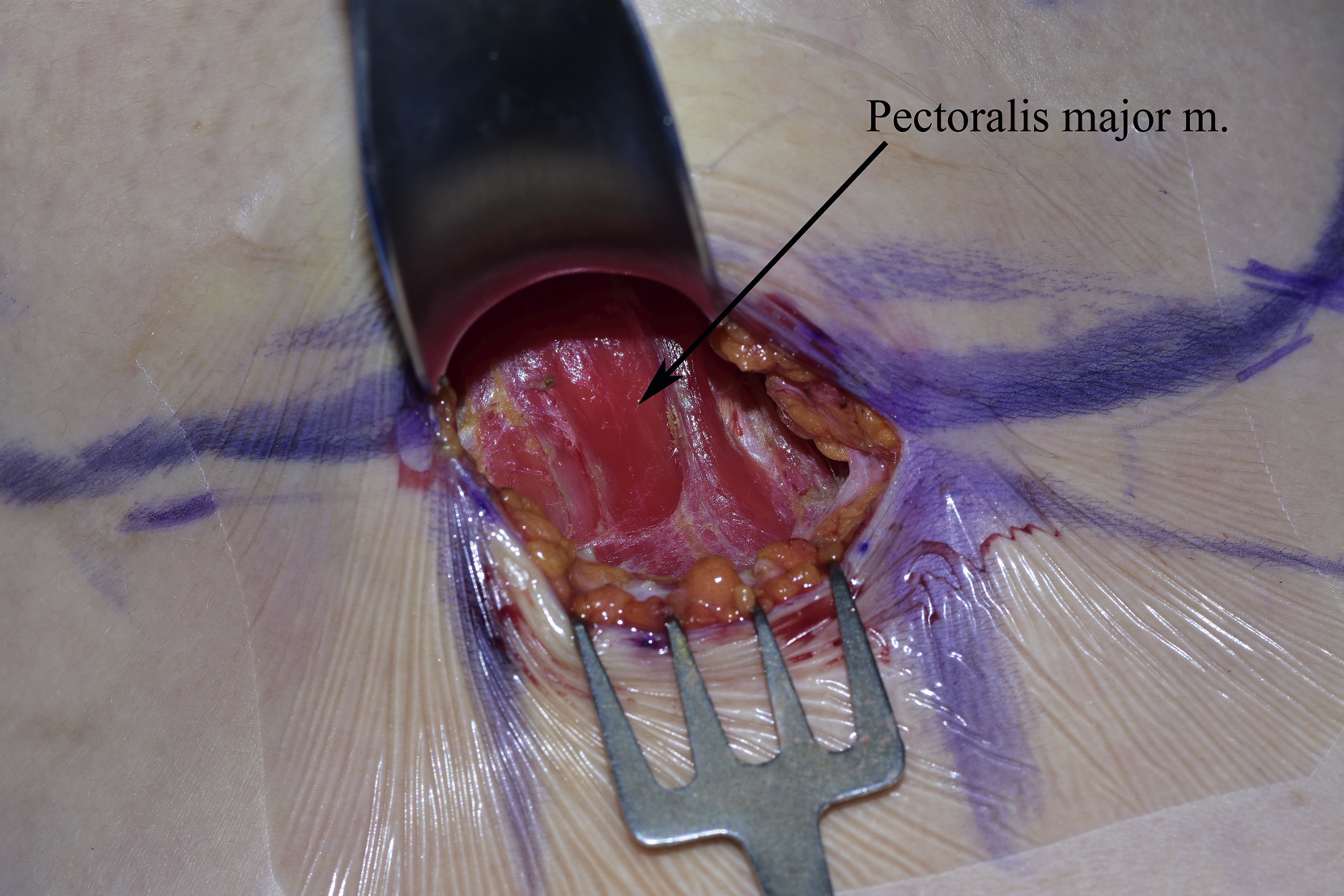
Check the direction of muscle fibers, and then use the retractor to grasp the mammary gland and subcutaneous tissue and to elevate pectoralis major musculature anteriorly, which will be very helpful to identify the lower lateral origin of the pectoralis major muscle ( Fig. 5.5 ). Differentiation of pectoralis major muscle from intercostal muscles is critical not to produce a pneumothorax, which comes from penetrating the intercostal muscles. The surgeon separates the pectoralis major muscle fibers from rib and its costal origin, leaving a 5-mm length of the stump at the origin to prevent inadvertent cutting of perforator, which may retract to the intercostal space, making bleeding difficult to control.
- 3.
Creation of implant pocket
When the lower and lateral costal origin of pectoralis major muscle has been divided laterally, the subpectoral space, a loose areolar space, can be found easily. Use the monopolar needle or forceps electrocautery to cut through the muscle fibers attached to the chest wall and to create a precise pocket. The width of the pocket is from the parasternal line, which follows appearance points of a medial cutaneous branch of the intercostal nerves to the anterior axillary line, which usually follows the line of appearance points of a lateral cutaneous branch of intercostal nerves. The horizontal dimension of dissection should just fit; should this be excessive, this may cause injury of the lateral cutaneous branch of the fourth, fifth or sixth intercostal nerve and widening of intermammary distance with the supine position.
The dissection plane will follow Tebbetts’ “dual-plane principle.” The general sequence should begin in a cranial direction, continue medially, and finish laterally. When the dissection continues cranially into the upper pole, surgeons should pay special attention to make sure not to deviate under the serratus anterior or pectoralis minor. The medial dissection also should be cautious and precise. The release of the pectoralis major muscle’s sternocostal origins in the medial border should be very cautious; the dissection should stop at about 4 o’clock on the right side and about 8 o’clock on the left side. Cranially from 4 and 8 o’clock level to 3 o’clock level, decreasing the cutting amount of pectoral sternal origin with gradual tapering can leave intact attachment of pectoralis major to the sternal origin. Leaving the sternal origin of the pectoralis major muscle is very important to prevent complications or unpleasant results, such as synmastia, neurovascular bundle injury, and future implant edge visibility and animation deformity. The dissection continues upward in a cranial direction, releasing the uppermost parts of the pocket just as needed with implant height. The last dissection will be the lateral part where the tissue should be released appropriately to create a fit and sufficient pocket for the selected implant.
A sizer can be a more accurate option to precisely check the dimensions of the pockets.
- 4.
Implant insertion
Soak the implants in an antibiotic solution or povidone-iodine (Betadine). The surgeon should change into a new pair of powderless gloves and be careful not to touch anything except the implants during insertion. Insertion of the implant into the pocket should be carried out carefully and consistently. There should be no rough force, nor a sharp instrument to insert. An insertion sleeve can be very helpful to squeeze the implant into the pocket. An insertion sleeve can avoid potential implant shell and gel injury and prevent any contamination of the implant from surgeons’ hands or surrounding tissue surface.
Once the implant has been inserted, the surgeon should check the right orientation and position of the implant, especially the anatomic implant. The surgeon can look at the line or markings on the anterior surface of the implant to make sure there is no upside down or rotation. Usually, no drain is needed for primary breast augmentation through IMF incision.
- 5.
Wound closure
Wound closure is another basic procedure in IMF incision breast augmentation. A multilayered wound closure technique can anchor the incision wound to the chest wall right at the new IMF, without any shift upward or downward.
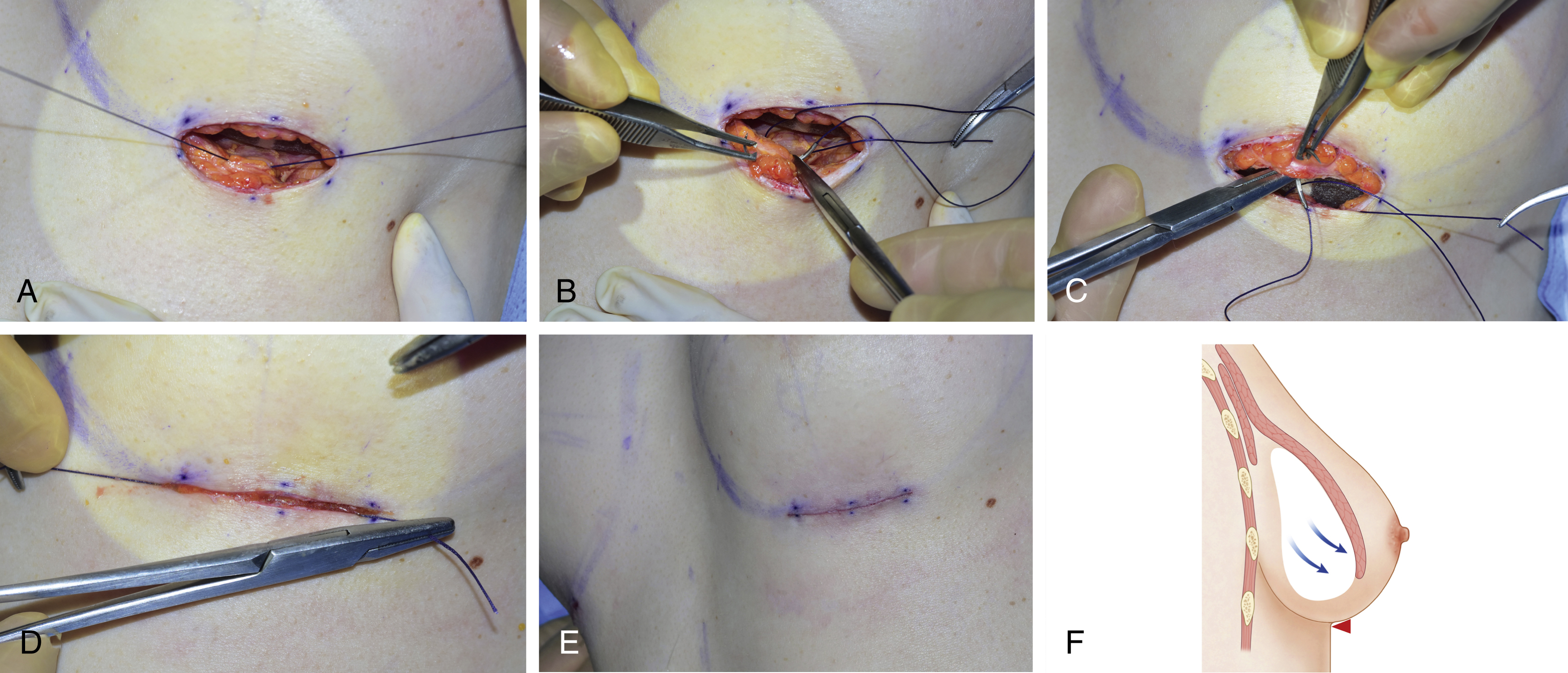
The wound is closed in three layers as follows. The first layer of sutures is three deep layer sutures with 2-0 Vicryl.
Three deep layer sutures are made at the central, medial, and lateral end of incision opening. The central deep layer suture is not tied at the beginning. For enhancing the medial and lateral deep sutures visualization, the central suture can be knotted tightly after medial and lateral suture knot formation. It is crucial to grip the fascial structure firmly so that the suture does not cut through the soft tissue. However, the surgeon must be careful not to go too deep to avoid pleura injury. The tension becomes minimal, and the edges of the wound can approximate each other with everting manner after first deep layer closing is adequately and firmly performed.
The second layer of sutures is superficial fat and dermal layer suturing, aiming to approximate the wound edges further and to bring tissue into a crest on both sides of the wound. Inverted sutures with long absorbable monofilament thread, like 3-0 PDS thread, which can last longer, can be used to reduce the dermal layer tension ( Fig. 5.6A–F ).