CHAPTER 67 Brachioplasty
Physical evaluation
• Evaluate the extent of adiposity and skin excess of the arm, axilla and lateral chest.
• Estimate the degree of upper arm tapered sagging along the posterior margin from the axilla and the elbow towards the most hanging center.
• Search for the inferior dislocation of the posterior axillary fold (PAF). The ptotic PAF broadens the attachment of the arm to the chest, simulating a wing. The loosely suspended PAF contrasts to the tightly adherent deep axillary dome and elongated anterior axillary fold.
• Analyze the enlarged and deep axilla. It may be more than twice normal, which we call hyperaxilla.
• Determine if the anterior axillary fold (AAF) is the flattened and elongated. The descended breast accentuates the AAF deformity.
• Consider the lateral chest skin laxity leading into mid-torso transverse rolls.
• The ideal candidate has ptotic skin that more than doubles the expected width of the upper arm.
• Oversized, obese arms should be identified and treated with liposuction. Brachioplasty may follow.
Technical steps
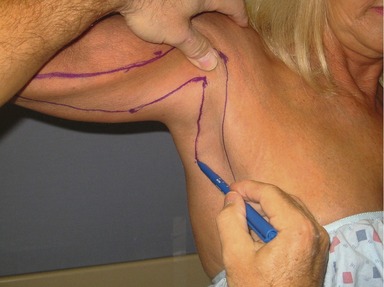
With the patient sitting, the arm and forearm are abducted 90 degrees with the palm forward. Dot the mid-point of the arm slightly posterior to the medial bicipital groove. An anterior line is drawn from the medial elbow through this dot to the deltopectoral groove across the dome of the axilla (Fig. 67.1). By gathering and pinching excess skin and fat posterior to the initial mark, the width of mid-arm excision is determined and a second dot is made near the posterior border (Fig. 67.2). A straight line is drawn from that point to meet the medial elbow termination of the first line (Fig. 67.3). Then by pinching posterior arm skin towards the superior axilla, a critical point is picked and marked along the inferior border of the medial arm that can be advanced to the deltopectoral groove at the proximal termination of the anterior line (Fig. 67.4). Approximation of these points should raise the posterior axillary fold, and equalize the lengths of the anterior and posterior lines. The line then acutely angles to descend inferiorly through the axilla, skirting the posterior axillary fold (Fig. 67.5). A parallel line descends from the deltopectoral groove through the axilla (Fig. 67.6). The distance between these last two lines removes the excess skin of the axilla and lateral chest.

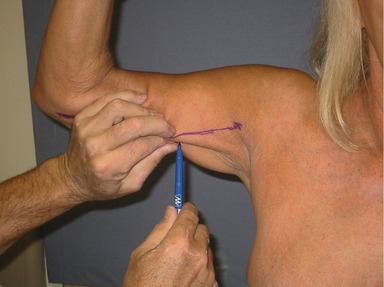
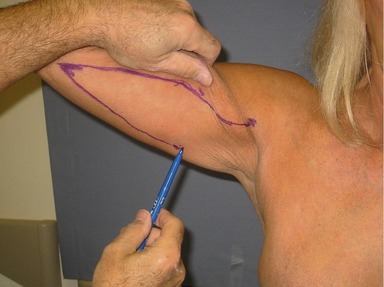
Fig. 67.3 A straight line is drawn from that point to meet the medial elbow termination of the first line.