For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
For videos accompanying this chapter see ExpertConsult.com . See inside cover for access details.
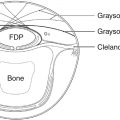
The brachial plexus comprises a complex grouping of nerve fascicles, giving function and sensation to the upper extremity. Progressing from proximally to distally, the plexus is divided into regions termed roots, trunks, divisions, cords, and branches. Within these nerves, there is a clearly defined internal topography that will guide future reconstructive efforts ( Fig. 53.1 ).

Roots
The traditional brachial plexus has contributions from cervical roots C5–C8 and thoracic root T1. Anatomical variations of this included a prefixed plexus (additional contribution from C4) and a postfixed plexus (additional contribution from T2). The spinal roots pass between the anterior and middle scalene muscles. There are three nerve branches exiting from the root level. The dorsal scapular nerve arises from the C5 nerve root and supplies the rhomboid muscles and the levator scapulae muscle. The long thoracic nerve arises from roots C5, C6, and C7 and supplies the serratus anterior muscle, which stabilizes the scapula. The nerve to subclavius arises from the distal C5 and C6 nerve roots. This nerve supplies the subclavius muscle, which is unable to be tested on clinical examination.
Trunks
In the inferior portion of the posterior cervical triangle, the roots combine to form trunks. The upper trunk is formed from C5 and C6. The middle trunk is a continuation of the C7 root. The lower trunk is formed from C8 and T1. There is a single branch off the upper trunk, the suprascapular nerve, that is critical for shoulder function. It departs from the upper trunk, travels deep to the trapezius muscle and runs through the suprascapular notch of the scapula to supply the supraspinatus and infraspinatus muscles.
Divisions
Passing deep to the clavicle, each trunk divides into an anterior and posterior division. There are no extraneous branches at the level of the divisions.
Cords
The divisions pass deep to the pectoralis minor muscle and combine in a predictable fashion to form the cords. The cords are named in relation to their anatomical location around the axillary artery. The anterior divisions of the upper and middle trunks combine to form the lateral cord. The medial cord is the continuation of the anterior division of the lower trunk. All of the posterior divisions combine to form the posterior cord.
Branches
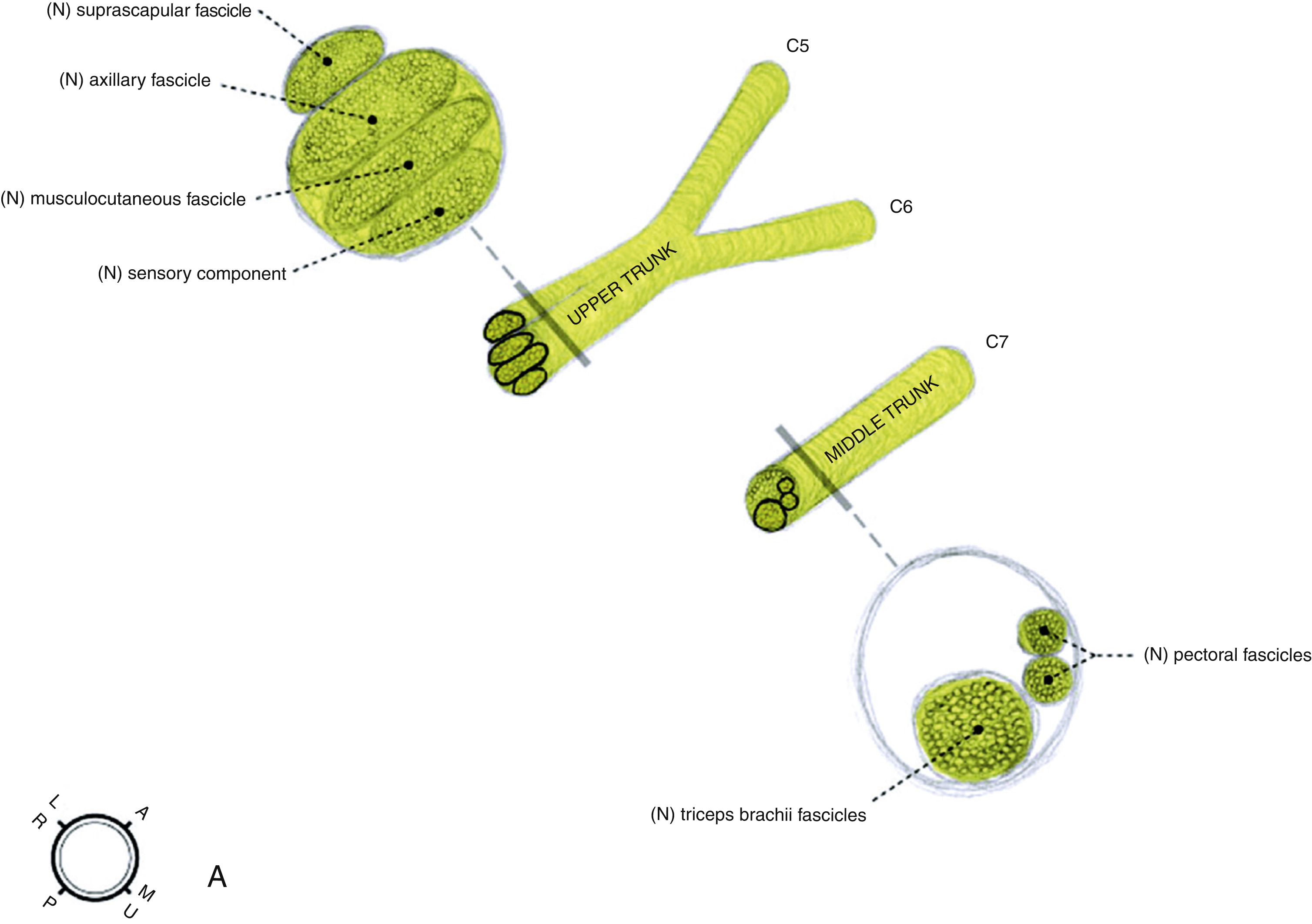
There are several branches that arise from the cords. The lateral cord gives off the lateral pectoral nerve, which innervates the clavicular head of the pectoralis major. The medial cord gives off the medial pectoral nerve, which innervates the sternocostal head of the pectoralis major muscle. The medial brachial cutaneous and medial antebrachial cutaneous nerves also branch from the medial cord supplying sensation to the medial aspect of the upper arm and forearm. More distally, the lateral and medial cords each contribute to the median nerve, supplying the sensory and motor functions of the nerve respectively. This relationship continues distally and is useful for understanding the internal topography of the median nerve, where motor fascicles are located on the medial side of the nerve and sensory fascicles remain more lateral. Following its contribution to the median nerve, the lateral cord becomes the musculocutaneus nerve. This nerve innervates the coracobrachialis, biceps brachii, and brachialis. The terminal portion of this nerve is the lateral cutaneous nerve of the forearm. After contributing to the median nerve, the medial cord becomes the ulnar nerve, which, after innervating the flexor carpi ulnaris and the small and ring flexor digitorum profundus muscles, is primarily responsible for the intrinsic musculature of the hand.
The internal topography of the ulnar nerve can best be remembered as sensory–motor–sensory, where the most medial portion of the nerve will eventually contribute to the dorsal cutaneous ulnar branch, exiting the main portion of the ulnar nerve approximately 9 cm proximal to the wrist crease and providing sensation to the dorsal ulnar aspect of the hand. After this division, the more medial 40% of the ulnar nerve will pass through Guyon’s canal to become the deep motor branch and the more radial 60% will contribute to the superficial sensory branch ( Fig. 53.2 ).
The posterior cord gives off the upper subscapular nerve, the thoracodorsal nerve, and the lower subscapular nerve. These branches innervate the superior portion of the subscapularis muscle, the latissimus dorsi muscle, and the lower subscapularis/teres major muscles, respectively. The two most terminal branches of the posterior cord are the axillary nerve and the radial nerve. The axillary nerve travels through the quadrangular space (bounded by the humerus, the long head of triceps brachii, teres minor, and teres major) with the posterior circumflex humeral artery. It innervates the deltoid and the teres minor, but also provides sensation to a patch of skin overlying the deltoid, sometimes known as the “soldier’s patch.” This sensory component is located at the most inferior portion of the axillary nerve. The radial nerve travels through the triangular interval (bounded by the teres major and the lateral and long heads of triceps brachii) with the profunda brachii artery. Wrapping around the spiral groove, the radial nerve goes on to supply the elbow, wrist, finger, and thumb extensors.
Clinical History and Assessment
Brachial plexus injuries occur in approximately 1% of polytrauma victims, most frequently in young males. The vast majority are due to motor vehicle collisions and of these, up to 84% may involve motorcycles. Due to these circumstances, many patients present with multisystem trauma requiring resuscitative procedures. Associated closed head injuries including loss of consciousness can occur in almost three-quarters of patients, which can often result in a delay of recognition of a brachial plexus injury. It is not uncommon for the patient to be the first to identify the injury. In the obstetrical population, approximately 1.6% of deliveries have a shoulder dystocia and of these, almost 20% experience a brachial plexus palsy.
Acquiring a thorough history is critical in the investigation of a patient with a brachial plexus injury. The mechanism of injury may provide information to recognize a pattern of injury or to estimate the degree of injury. For a trauma, details about a motor vehicle collision, including the speed, direction of impact, use of safety equipment such as seatbelts or helmets, and concomitant injury may be useful in ascertaining risk to certain structures. In the event of a blow or a fall, knowing the direction and weight of impact, location of impact, and arm position can contribute valuable information. Knowledge of preexisting upper extremity injuries and medical comorbidities is also useful. The patient’s general medical status may contribute to candidacy for surgical intervention. In an obstetrical brachial plexus injury, information about birth weight, gestational age, shoulder dystocia, delivery aides such as forceps, and duration of labor are useful.
An important component of the history is evaluation of pain. Patients should be questioned regarding the severity, location, and nature of their pain to assist in determining musculoskeletal versus neuropathic components. Severe pain can be suggestive of root avulsions. Inclusion of a pain questionnaire at the initial assessment and then at subsequent visits can provide both quantitative and qualitative assessment of pain. Having a low threshold for starting neuropathic pain medications or involving a pain specialist is crucial for these patients, as pain management can be a significant problem. In addition, patients should be screened for depression and mood disorders, as the incidence in this patient population can be as high as 40%.
In this patient population, serial clinical examination is crucial to determine spontaneous recovery. At the initial physical examination, a complete upper extremity sensory and motor examination should be performed with care to document both peripheral and central nervous system examination. Atrophy may not initially be present but will later mark denervated muscle groups. Having a systematic approach to the brachial plexus examination will allow for determination of patterns of injury and more specifically about level of injury. A thorough knowledge of the anatomy of the plexus can help to localize lesions simply by physical examination.
The location of scars on the upper extremity, shoulder, and neck should be noted, from either trauma or surgical intervention. Joint mobility should be assessed for the entire extremity, and, in the setting of any decreased passive range of motion or stiffness, early intervention with an occupational or physiotherapist should be arranged to optimize overall outcome. Assessment should be carried out for concomitant findings such as a Horner’s sign (ptosis, miosis, and anhydrosis), which occurs due to injury to the cervical sympathetic fibers during avulsion of the C8 and T1 roots.
Perhaps the most critical part of the physical examination is accurate documentation. Careful recording of the Medical Research Council (MRC) scale for muscle strength for each muscle group in an organized fashion will allow comparison over time. Given the known rate of recovery following nerve injury of 1 mm/day, this allows for assessment of whether spontaneous recovery is progressing at the expected rate, or whether surgical intervention may be appropriate. It should be remembered that examination for potential donors is as important as identifying nonfunctioning muscle groups. The preparation for surgical reconstruction of brachial plexus injuries is the biggest determinant of success.
Etiology
The etiology of brachial plexopathy can be traumatic, iatrogenic, compressive, neuralgic amyotrophy or radiation.
Traumatic
The majority of brachial plexopathies secondary to trauma occur in young males, with up to 90% of cases comprising this patient population. Traumatic injuries to the brachial plexus can be divided into open and closed injuries. Open injuries are those secondary to penetrating injury, such as knives or other sharp objects. These necessitate immediate surgical exploration. The majority of traumatic brachial plexus injuries are closed, and these can be composed of crush injuries or traction injuries. Crush injuries tend to occur after motor vehicle accidents, whereas traction injuries are more likely to be related to motorcycle accidents, skiing, falls, and sports injuries. In traction injuries, displacement of the upper extremity inferiorly combined with neck flexion contralaterally causes an increase in the neck–shoulder angle, which results in injury to the upper roots and trunks. This commonly occurs in both high-velocity injuries such as motorcycle collisions and also in lower-velocity accidents such as sports injuries. The opposite can occur with strong upward force or traction on the upper extremity increasing the scapula–humoral angle and causing injury to the lower plexus. The brachial plexus is susceptible to these injuries due to limited mobility secondary to prevertebral fascia and attachment of the cervical roots to the vertebrae. Traction injuries are also responsible for obstetrical brachial plexopathies, most commonly following shoulder dystocia. Risk factors for obstetrical plexus injury include high birth weight, fetal acidosis, posterior arm involvement, and narrow pelvis.
Iatrogenic
During long operations, positioning of the upper extremity can contribute to a traction palsy. Most commonly these injuries are neuropraxic in nature and will recover spontaneously; occasionally, however, a more severe injury will occur. There are patient factors that contribute to the propensity for developing these injuries, including diabetes, hypothyroidism, prior injury, hereditary neuropathy with liability to pressure palsy (HNPP), and obesity.
Compression
Compression can be secondary to structures adjacent to the plexus in an enclosed space such as malignancy, callous formation, hematoma or pseudoaneurysm. Anatomical variants may be responsible for compression primarily or may increase the propensity for trauma to the brachial plexus. These variants include cervical ribs, prominent transverse processes, and congenital fibrous bands. Compression often occurs in the costoclavicular space as the brachial plexus travels between the clavicle and the first rib. Traumatic injuries can result in swelling or hematoma that cause compression of the brachial plexus. Occupational injuries where a heavy object lands on the shoulder or neck are an example.
Neuralgic Amyotrophy
Brachial neuritis, or Parsonage–Turner syndrome, is a brachial plexopathy of unclear etiology that most commonly involves the lower brachial plexus; the axillary nerve is implicated in up to 70% of patients. Most commonly, these nontraumatic plexopathies present with a history of severe neuropathic pain that resolves and then is followed by patchy weakness. Possible contributory factors are viral disease, infection, immunization, trauma, surgery, and autoimmune mechanisms. The majority of these plexopathies will have a full spontaneous recovery within approximately 3 years, however the prognosis is more guarded in the setting of other medical comorbidities such as diabetes.
Radiation
Transient or permanent brachial plexopathy can occur as a result of radiation therapy. Approximately 1.2% of women receiving radiation as adjuvant therapy for breast cancer will present with clinical manifestations anywhere from 6 months to 20 years following treatment (median 1.5 years).
Investigations
Imaging
Brachial plexopathy and level of injury are primarily a clinical diagnosis supported by electrodiagnostic studies, however there are several circumstances where imaging contributes valuable information.
Plain films are useful for identifying fractures that might be associated with certain patterns of brachial plexopathy. For example, a transverse process fracture is more likely associated with a root avulsion injury because of the deep cervical fascia that tethers cervical root to transverse process. Clavicular fractures can cause sharp injuries to the plexus on bony fragments, or can contribute to compression injuries related to either hematoma acutely, or callus formation in a more delayed fashion.
CT myelography is a useful investigation for assessing for root avulsion. The use of contrast material allows for visualization of the dural sheath around the nerve root, which is not pathognomonic for a root avulsion, but can be suggestive. The absence of a root at a particular level is diagnostic. When obtained at least 1 month post injury, which allows time for the dural sheath to heal improving distribution of the dye, CT myelography is associated with a sensitivity of 95% and a specificity of 98% for root avulsion injuries.
MRI is becoming a more valuable tool for the imaging of the brachial plexus due to newer techniques and protocols. The advantage of MRI is that it can directly visualize the entire brachial plexus and is noninvasive. Soft tissue injury is more easily assessed and three-dimensional imaging is possible.
Electrodiagnostic Studies
It is crucial that all patients presenting with brachial plexopathies receive electrodiagnostic studies, and in many cases serial studies will confer helpful information in the decision to proceed with surgery. Electrodiagnostic studies are not useful before Wallerian degeneration has occurred and fibrillation potentials have appeared, therefore delaying investigation for approximately 6 weeks is beneficial. There are two components to the electrodiagnostic study: nerve conduction and electromyography. Nerve conduction studies are traditionally more useful for compression neuropathies, although they can portray valuable information in the setting of a preganglionic lesion to the brachial plexus. In these injuries, the dorsal root ganglion remains intact and the peripheral sensory nerve does not undergo Wallerian degeneration. The motor nerve, however, arising more proximally in the spinal cord, will still be affected. The resultant nerve conduction studies will demonstrate intact sensory nerve action potentials (SNAPs) but no volitional activity.
The electromyography portion of the study also has several components. On insertion of the needle, a denervated muscle will exhibit spontaneous discharges or fibrillations and positive sharp waves. In contrast, a normal muscle will not have any waveform on insertion alone. When the patient is asked to voluntarily contract the designated muscle, the presence of motor unit potentials (MUPs) signifies that the action potential is reaching the desired motor endplate. Nascent units are representative of connections to the motor endplates from regenerating injured axons, while MUPs signify distal motor sprouting from uninjured axons. Both are good prognosticators of a spontaneous recovery without surgical intervention. Electromyography often precedes clinical signs of recovery by 1–2 months, and the presence of new MUPs and nascent units can be a promising prognostic sign before the patient notices any changes. In addition, electrodiagnostic studies can be valuable in preoperative planning, especially where nerve or tendon transfers are being contemplated.
Patterns of Injury
Brachial plexus injuries can occur in any potential combination, however there are several common patterns of injury that warrant mention, as the approach to treatment can be dictated by the predictable deficits.
Upper Plexus Injuries
These injuries comprise injuries to the C5 and C6 roots or to the upper trunk. This occurs when the shoulder is wrenched away from the head and neck. Classically these patients will present with deficits of shoulder abduction, external rotation, and loss of elbow flexion. There will be a concomitant loss of sensation over the deltoid muscle. A sulcus sign may be present, identifying the inability of the shoulder girdle to support the weight of the arm ( Fig. 53.3 ). Priorities are to reestablish elbow flexion and then to restore shoulder stability and function.