23 Bone Flaps and Bone Transport for Lower Limb Reconstruction
Summary
Bone defects of greater than 5 cm are best managed with vascularized bone flaps. The vascularized fibula bone flap is the most commonly used and versatile flap for managing acute bone loss, late nonunions and allograft failure. For extensive soft-tissue loss, vascularized rib grafts used in conjunction with the serratus and latissimus muscle flap can provide soft-tissue coverage and bone reconstruction in one setting. For small recalcitrant defects, the medial femoral condylar flap provides vascularized cortical cancellous graft with vascularized skin.
Keywords: bone defect, bone reconstruction, vascularized bone graft, bone flap, fibula flap, vascularized rib bone, medial femoral condylar flap
23.1 Introduction
Functional restoration of the lower extremity following trauma, infection, or tumor extirpation can be challenging for the reconstructive surgeon; this is particularly true in the cases involving segmental bony loss of the tibia or the femur. For these defects, restoration of function requires bone reconstruction for stable weight bearing and ambulation. In addition, adequate soft tissue must be present to provide coverage of bone and hardware. Amputation of severely traumatized limbs is always an option, but amputation can be associated with morbidity in the form of increased cardiopulmonary and metabolic demands during prosthetic-based ambulation, increase in overall sedentary activity, and a resultant 5-year mortality rate of up to 68%.1
Efforts at limb salvage in the cases of trauma and tumor extirpation have led to the development of several strategies for the reconstruction of segmental bony defects. For defects less than 5 cm, a variety of allograft, synthetic, and nonvascularized autograft options are available. For bone defects that are greater than 5 cm in length and for smaller recalcitrant defects in areas of infection or radiation, vascularized autologous bone flaps and bone transport are reliable means of bony reconstruction. This chapter will review the major bone flaps used for reconstruction in the lower extremity and the principles of bone transport.
23.2 General Principles for Reconstruction of Bone Defects
Small bone defects, up to 5 cm, can often be repaired with shortening or nonvascularized bone grafting, provided there is an adequate soft-tissue envelope and the wound is free of infection.2 Nonvascularized bone grafts are incorporated into defects through the process of creeping substitution and vascular ingrowth. Creeping substitution refers to a process of vascular ingrowth into the bone graft with subsequent resorption and replacement of the donor necrotic bone. Multiple donor sites exist for the harvest of nonvascularized cortical or cancellous autogenous bone; donor sites include the iliac crest, proximal ulna, and distal radius. Cancellous graft is usually preferred, unless there is the need for structural stability, as it is replaced more quickly than cortical bone by the process of creeping substitution. Nonautologous bone and bone substitutes can also be used for small bone defects; nonautologous options include cancellous and cortical allograft, calcium phosphate, and calcium sulfate. Nonautologous bone grafts are replaced more slowly than autologous bone, and often produce an immune response that inhibits complete replacement of the donor bone. A complete discussion of benefits and downsides associated with nonvascularized bone grafts is beyond the scope of this chapter; however, for small defects, it is our preference to use autologous bone if possible.
In contrast to bone graft, vascularized bone flaps allow for primary bone healing instead of depending on creeping substitution initiated by the recipient bone. The process of creeping substitution and bone remodeling may be compromised (or even absent) if the surrounding bone has been affected by radiation and infection or suffers from avascular necrosis.3,4,5 In these situations, vascularized bone grafts have been shown to provide more rapid healing, reduce the risk of subsequent fracture, and have the ability to remodel under physiologic load allowing for early weight bearing and bone hypertrophy.6,7
Keys for successful reconstruction for any bone defect include thorough debridement of nonviable tissue, stable skeletal fixation, and adequate soft-tissue coverage. If these three components are not achieved, then even reconstruction with a vascularized bone flap will fail. For lower extremity reconstruction, it is best to work as a team with the orthopaedic trauma surgeons. The trauma surgeons can assist with bone debridement and fixation, while the microsurgeon provides soft-tissue coverage and bone flap reconstruction.
For most bone infections and subacute traumas, we perform debridement back to bleeding bone. In the cases of established osteomyelitis, we will place antibiotic impregnated polymethyl methacrylate cement into the defect in the form of a block spacer or as antibiotic beads for 6 to 8 weeks prior to reconstruction.8 Bone stabilization in these cases is initially achieved with an external fixator. An eternal fixator allows for bony stability, yet places hardware away from the infected site (▶ Fig. 23.1). The polymethyl methacrylate is removed following the 6 to 8 weeks and the defect is filled with vascularized bone. The external fixator can be left in place until bony healing is achieved.
In the cases of acute open trauma, it is our preference to use internal fixation whenever possible for the definitive fixation, as this minimizes the need for external wires or fixators, which can compromise soft-tissue reconstruction and hamper rehabilitation (▶ Fig. 23.2). The concept of definitive fixation and flap coverage in a single setting is ideal to minimize the chances of hardware contamination and has been shown to produce union rates of better than 95%.9 At the time of presentation and following the initial debridement, these patients can be managed with temporary external fixation until definitive soft-tissue and bony debridement is completed. Once the wound is free of nonviable and contaminated tissue, definitive bony fixation is achieved with intramedullary rods or plates and screws, following which the leg is covered with a free or pedicled flap. Regardless of the type of fixation used, stable bone fixation is imperative and is the cornerstone upon which successful limb salvage is based.
Similar principles are followed in the cases of tumor surgery. A multidisciplinary team is used where the oncologic surgeon can guarantee clean margins and assist in bony reconstruction. For intercalary bone reconstruction, there are many options for limb salvage, including tumor prosthesis, total prosthetic joint replacement, and massive cadaveric allograft reconstruction. While these options have all been shown to produce acceptable early limb salvage rates, they can suffer from long-term risks of fracture, nonunion, and infection.10,11 We feel that vascularized bone flaps with or without massive cadaveric allograft reconstruction provide the most reliable means of long-term limb salvage. The one caveat in these cases is that additional nonvascularized autologous bone graft should be used to augment the osteosynthesis sites (either the two cut ends of the fibula or the surface beneath the vascularized bone graft). Additional autologous graft has been shown to limit cases of delayed union. The use of vascularized fibular flaps in the setting of malignant tumors has shown union rates of better than 90%.12 In the following sections, we will discuss our workhorse flaps for segmental bone loss in the lower extremity.
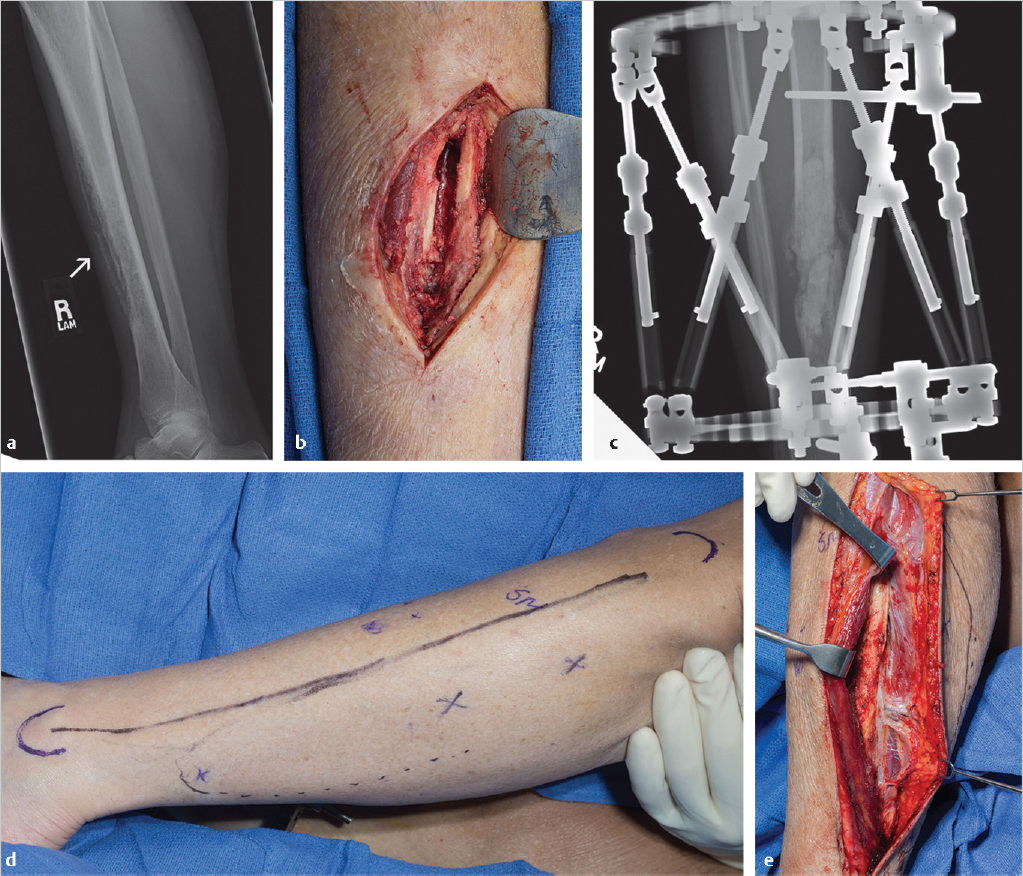
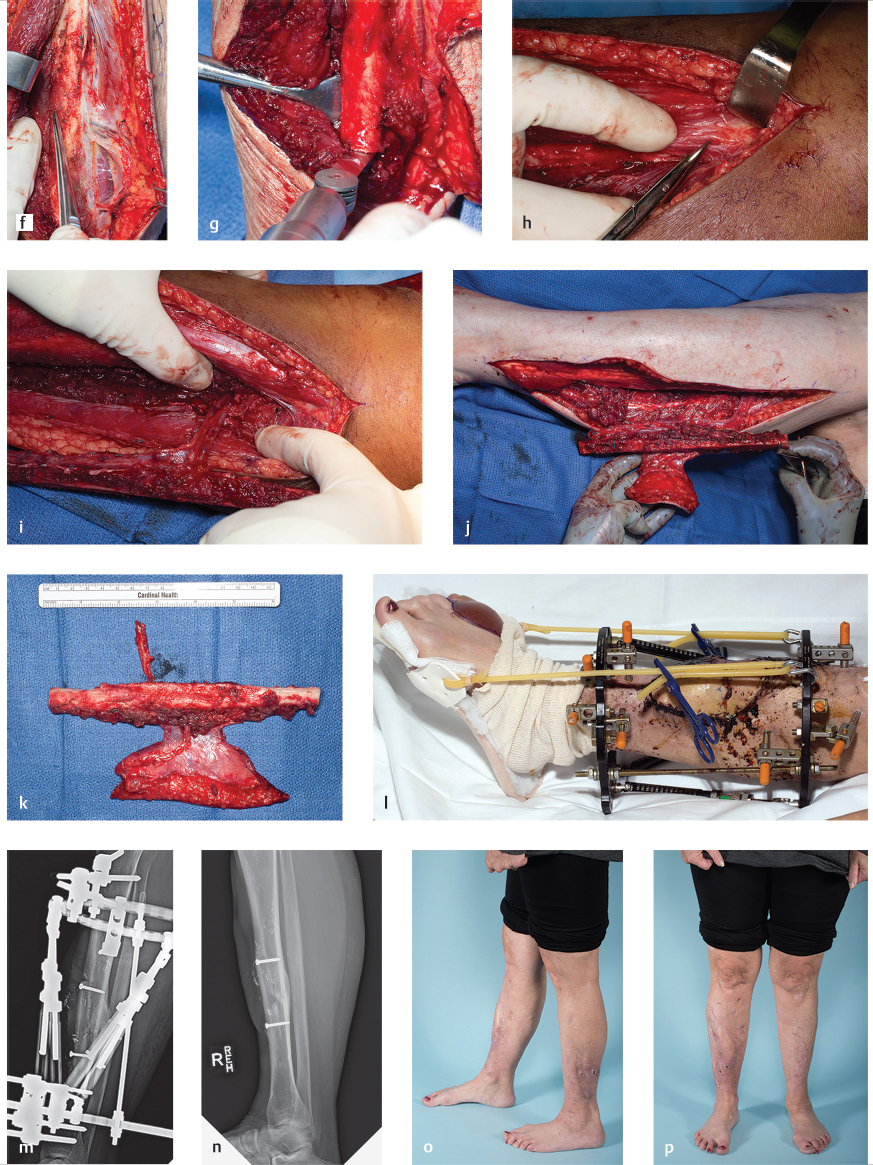
Fig. 23.1 (a) Anteroposterior radiograph of a 59-year-old woman with chronic osteomyelitis (arrow) of her right tibia as a result of an open fracture treated over 10 years ago. (b) Initial management consists of bone debridement, antibiotic bead placement for 6 weeks, and (c) external fixator placement for stability during treatment process. (d) A free fibula flap with a skin paddle is chosen for definitive treatment of the bone defect. Flap design begins by identifying Doppler signals in the skin (marked with X) just posterior to the fibula border, which correspond to cutaneous perforators for designing the skin island. (e) Dissection begins by elevating the anterior aspect of the incision until one identifies the interval between the peroneus muscles and the soleus. The fascia covering the peroneus muscle is elevated to reveal the perforators passing posterior to the fibula in the posterior crural septum. (f) Once the perforators are clearly identified the posterior margin of the skin island can be dissected. The major cutaneous perforator can be seen in this image along with the anterior and lateral dissection over the fibula. (g) The distal osteotomy is made with the aid of a Chandler retractor placed beneath the fibula to protect the peroneal vessels. (h) The common peroneal nerve (shown at the tip of the scissors) is identified at the superior margin of the incision prior to completing the proximal dissection and proximal osteotomy. (i) Once the proximal osteotomy is performed, the peroneal vessels are dissected back to the tibial peroneal trunk. (j) The fibula is now entirely isolated on its vascular pedicle. (Continued) (k) An image of the flap prior to insetting. (l) The leg is maintained in external fixator until definitive bony union. An elastic band attached to the fixator is used to prevent Achilles contracture. (m) Lateral radiograph showing insetting of the fibula using two compression screws. (n) Lateral radiograph of healed bone. (o, p) Clinical appearance of the salvaged limb and resultant donor site scar on the left leg at 2 years postoperatively.

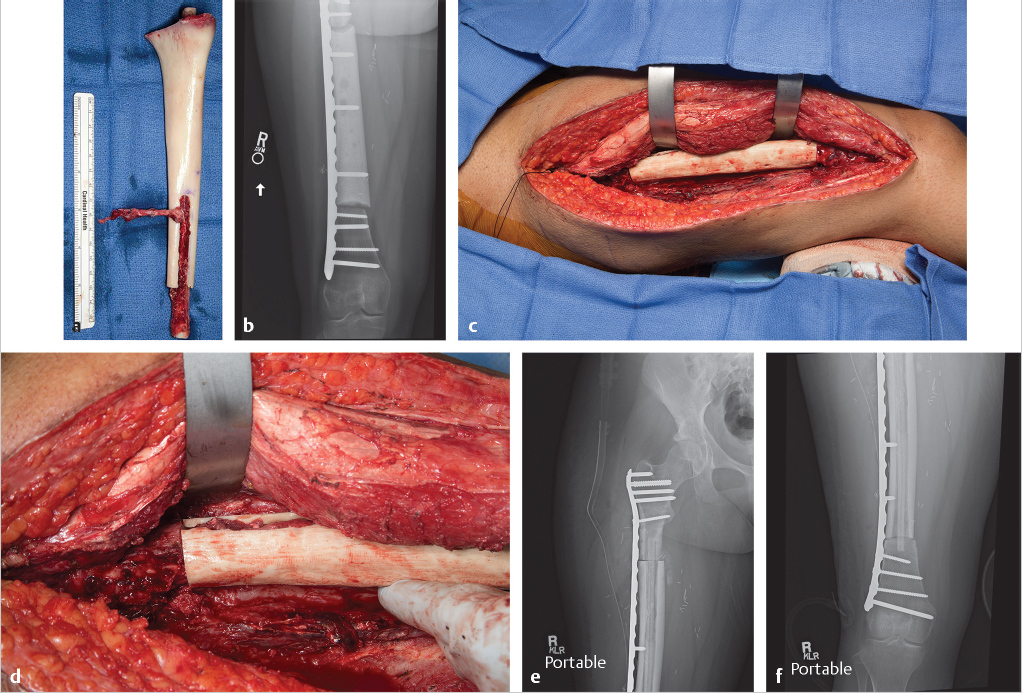
Fig. 23.2 (a) Anteroposterior radiograph of a 28-year-old man who suffered an open compound fracture of his tibia and fibula. (b) Reconstruction is started with debridement of the bone defect and (c) extensive debridement of the surrounding dead muscle and soft tissue. (d) A single rib is harvested with the serratus and latissimus for soft-tissue coverage and bony reconstruction. (e) This intraoperative image shows the vessel loops surrounding branches of thoracodorsal vessels. The arrowhead points to the rib and the arrow points to the pleura. The chest defect can be covered with synthetic mesh or acellular dermal matrix. (f) The chimeric flap is transferred to the leg where an end-to-side anastomosis is performed between the thoracodorsal artery and the posterior tibial artery. The long pedicle length allows for easy insetting of the rib. (g) The rib is secured to the tibia with sutures placed (h) through bone tunnels. The fracture is also stabilized with an intramedullary rod. (i) Postoperative radiograph at 5 months showing early consolidation and at 2 years (j) showing bony union with hypertrophy of rib graft. (k, l) Clinical appearance of the leg at 5 months postoperatively.
23.3 Fibula Flap
23.3.1 Introduction
The fibula flap was originally described by Taylor et al in 1975 as a vascularized bone flap for augmented osteoinduction in a large tibial defect.13 The flap was then modified by Chen and Yan in 1983 to include a skin paddle. The fibula osteocutaneous flap has remained a workhorse flap for segmental and intercalary bony defects in combination with soft-tissue reconstruction.14 The ubiquitous use of this flap for long bone reconstruction is due to the length of bone one can obtain (over 25 cm) and the ability to reliably carry a cutaneous paddle with the flap. Multiple reports have demonstrated excellent rates of union, with up to 80% primary union rates and as high as 97% following supplemental bone grafting.12
23.3.2 Attributes
• Bicortical bone for increased mechanical strength and potential weight bearing.
• Longest available piece of vascularized bone for reconstruction (~25–30 cm).
• It can be osteotomized to fit recipient defect.
• Multiple configurations include longitudinal strut, double-barreled, onlay, and as a hybrid used in conjunction with massive cadaveric allograft.
• Large diameter vascular pedicle based on peroneal artery and comitantes.
23.3.3 Detriments
• It sacrifices a major blood vessel to the lower leg.
• Proximal and distal osteotomies must be carefully placed to avoid injury to the common peroneal nerve (CPN) or ankle mortise.
• Skin paddle design inclusion frequently results in the need for skin grafting at the donor site.
• Dissection through the flexor hallucis can result in a stiff or contracted toe.
• It can result in chronic ankle instability.
23.3.4 Anatomic Considerations
The fibula receives its blood supply from the peroneal, anterior interosseous, and lateral geniculate arteries15; however, the majority of flaps are designed to utilize the peroneal artery as the flaps’ major blood supply. All of the vessels supplying the fibula originate from the popliteal artery. After passing beneath the popliteus muscle, the popliteal artery divides into two major terminal branches: the anterior tibial artery and the tibioperoneal trunk. The anterior tibial artery branches proximal to the tibioperoneal trunk and perforates the interosseous membrane to travel within the anterior compartment of the leg. After passing through the interosseous membrane, the anterior tibial artery gives off several branches that supply the fibular head and fibular physis in children. These branches include the circumflex fibular artery as well as the first and second recurrent epiphyseal arteries.15 Distal to the anterior tibial artery’s branch point, the popliteal artery terminates in the tibioperoneal trunk, which divides into the posterior tibial artery (coursing medial) and peroneal artery passing laterally to run along the posterior medial surface of the fibula.
After branching to the fibula, the peroneal artery runs in close proximity to the medial surface of the fibula between the tibialis posterior muscle and the flexor hallucis muscle. The peroneal artery provides both a nutrient vessel for endosteal blood flow and multiple periosteal perforating branches. The nutrient artery to the fibula diaphysis enters in the middle third of the bone and should be preserved during dissection. Additionally, the peroneal artery gives off several perforators to the lateral leg skin. These perforators pass along the posterior margin of the fibula, within the septum of the deep posterior compartment, also referred to as the posterior crural septum. A pooled analysis of 1,710 peroneal perforators was performed to evaluate the location and frequency of these cutaneous perforators along the axis of the fibula. The authors found that if the total length of the fibula is marked off into tenths from proximal to distal, the area with the highest density of perforators was localized in the sixth interval from the fibular head, with 19% of all perforators being found in this region. There was a 79% positive predictive probability of finding a skin perforator in this region. More proximal along the fibula, perforators are more likely to travel through the muscle belly of the soleus prior to irrigating the skin, whereas distal perforators are more likely to be septocutaneous due to the Achilles musculotendinous interface.16
Finally, the surgeon should be aware of the course of the CPN, as it runs close to the proximal limits of the fibula dissection (▶ Fig. 23.1). The nerve originates from the apex of the popliteal fossa after splitting from the sciatic nerve, which continues distally as the tibial nerve. The CPN then travels between the head of the lateral gastrocnemius and the medial margin of the biceps femoris. At the fibular head, the CPN will often be encountered in the plane of dissection of the fibular flap as it moves from the popliteal fossa to the lateral compartment. At the level of the peroneus longus, the nerve divides into the superficial branch and deep peroneal branch. To protect the nerve and its branches, the proximal osteotomy is typically made 5 to 7 cm distal to the fibular head; however, if necessary, the head of the fibula may be taken for added length or for cases that require a growth plate transfer. In such cases, the nerve should be identified and protected during flap elevation.
23.3.5 Anatomic Variations and Potential Pitfalls
The complications seen with the fibular flap are often related to lower leg anatomic variation and fibula donor site morbidity. Due to the limited skin laxity, intramuscular dissection, and ankle mortise changes, removal of the fibula can be associated with several donor site complications. Momoh et al17 evaluated 157 consecutive patients who underwent a free fibula flap for head and neck reconstruction, in order to determine the risk factors for acute and long-term morbidity following use of the flap. They found a 31.2% incidence of perioperative complications, most commonly due to local wound disruptions, including skin graft loss at the closure site (15%), cellulitis (10%), and dehiscence (8%). Additionally, long-term complications were identified in 17% of patients, and were commonly related to gait disturbances, with decreased ankle mobility (12%), hallux contracture (9%), leg weakness (8%), and ankle instability (4%). Despite these complications, the authors reported that 96% of patients returned to their preoperative level of ambulatory activity.
From a vascular standpoint, in patients with normal three-vessel runoff the harvest of the peroneal artery appears to have minimal impact to the overall vascularity and viability of the distal leg and foot. To demonstrate this, near-infrared spectroscopy has been utilized pre- and postoperatively following the removal of the fibula flap and the corresponding peroneal artery. The study found that the distal oxygen saturation decreased less than 5% in the first 8 hours postoperatively; however, the oxygen saturation subsequently recovered to the baseline after 8 hours.18
In rare instances, the posterior tibial or anterior tibial arteries can be hypoplastic or injured, and the peroneal artery subsequently becomes a dominant arterial supply to the lower leg and foot. In rarer instances, both the posterior tibial and the anterior tibial are aplastic, creating a hypertrophied peroneal artery, referred to as a peronea arteria magna. To determine the incidence of these rare variations, a systematic review was conducted among 26 studies, which examined a total of 5,790 limbs.19 The study found that abnormal branching patterns with at least one hypoplastic artery have been reported in 5% of patients. The most frequent variation reported was a hypoplastic posterior tibial artery, whereas the incidence of the peronea arteria magna was only found in 0.4% of limbs.
While the incidence of anatomic variation is low, we still recommend preoperative evaluation of the lower extremity prior to flap elevation. In the cases of lower extremity trauma, this may be even more important for the recipient limb, where single vessel traumatic occlusion can be seen in greater than 25% of patients requiring free tissue transfer.20 A CT angiogram can provide detailed anatomic arterial information of both lower limbs and can be obtained with little risk to the patient. Finally, during flap elevation, the surgeon should carefully verify that the peroneal artery is the selected vessel, as retractors or dissection within the posterior compartment can place the posterior tibial artery in close proximity to the fibula, potentially resulting in injury to the posterior tibial artery or common tibioperoneal trunk.
23.3.6 Flap Design
The fibula can be either oriented as a single longitudinal flap or osteotomized to create a “double-barreled” paired configuration (▶ Fig. 23.3). The paired endosteal, or “internal,” and periosteal (“external”) circulations allow the segments to remain well vascularized if the intervening periosteal sleeve is left intact without injury. The double barrel may be especially useful when reconstructing large metaphyseal defects or areas subjected to high axial strain and weight bearing. However, in order to have sufficient bone for reconstruction, the double-barrel configuration should be limited to defects less than 13 cm in length, based on the average available length of the fibula.

Fig. 23.3 Intraoperative image of a double-barreled fibula flap construct. The peroneal artery is carefully left in continuity as a portion of the fibula is excised or osteotomized to allow for folding of the fibula. This configuration allows for easier reconstruction of metaphyseal defects.
Some authors have advocated for the use of the longitudinal vascularized fibular strut with a combination of rigid plating, as the fibular flap will eventually hypertrophy following repetitive load. Sainsbury reported on 18 patients with fibula flap interposition following resection for sarcoma. In this group, the mean time to union was 24 months (range, 9–72 months), and the authors found that the fibula underwent significant hypertrophy following axial loading, with resultant diameters of 71% of the recipient bone.21
Alternatively, in the cases of chronic nonunion, the fibula can be utilized to augment primary bone healing in combination with autograft or allograft. The “onlay” technique describes a technique where the fibula is used to span the site of nonunion to increase osteogenesis and primary bone healing; this technique is especially useful in the cases of chronic infection, failed massive allograft, or irradiated avascular bone.22 Friedrich et al evaluated the outcomes of 25 patients who received an onlay fibular flap, and found fracture union in 21 patients at an average of 11 months postoperatively, 22 of these patients having received prior bone irradiation. The authors noted that 21 of the fractures were pathologic secondary to irradiation and avascular necrosis. Prior to fibular flap treatment, 10 patients had failed operative fixation of the fracture with a nonunion for an average of 14 months, and the remaining 15 had trialed and failed cast immobilization.23
In oncologic cases where the intercalary bone defect exceeds the length requirements of a double-barreled design, or in those that may require more rigid osteosynthesis, the fibula flap can be placed within the center of an allograft. This hybrid technique was originally described by Capanna in 1993 for reconstruction of large oncologic intercalary bone defects of the tibia, and utilizes an allograft that has been cored or hallowed to allow the passage of the fibula flap internally (▶ Fig. 23.4). The fibula can be slotted into the intramedullary canal of the allograft. A channel is then created within the allograft with a rotary burr to allow access and passage of the vascular pedicle (▶ Fig. 23.4). The Capanna technique allows for immediate rigid fixation as large plates, or double plating can be applied to the allograft, while the fibula remains protected from injury during hardware fixation. In the long term, the fibula allows for accelerated healing at the osteosynthesis sites. In addition, the fibula helps revascularize the allograft leading to lower rates of infection and late fracture.11
Studies evaluating the outcome of the Capanna technique have demonstrated improved time to bone healing and subsequent weight bearing. Houdek et al evaluated their outcomes with the technique in 18 pediatric patients who underwent limb salvage following oncologic tibial resections. In this group, the overall limb salvage rate was 94% and despite 6 patients requiring a secondary procedure for a symptomatic nonunion, 17 of these patients had good or excellent outcome as indicated by their Mankin score.24,25 Similar findings were demonstrated by Schwarz et al. In their retrospective review of 13 patients, 8 required secondary bone grafting for nonunion, but the median time to union was 10 months (range, 3–40 months) and of the surviving patients, 91% achieved full weight bearing by 2 years and were able to participate in sports.26
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Nonflap Wound Closure Alternatives: Skin Graft, Skin Substitute, Skin Stretch, and Negative-Pressure Wound Therapy
Nonflap Wound Closure Alternatives: Skin Graft, Skin Substitute, Skin Stretch, and Negative-Pressure Wound Therapy
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


