Fig. 70.1
BPDCN: Clinical manifestation with contusiform macules on the trunk
Pathology
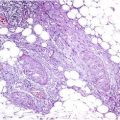
In fully developed skin lesions, there is a dense dermal monomorphous infiltrate of blasts. The infiltrate is separated from the epidermis by a grenz zone (Fig. 70.2). The blastic tumor cells display nuclei with fine-dispersed chromatin and a sparse cytoplasm (Fig. 70.3). Extravasated erythrocytes are a characteristic finding which leads to the contusiform clinical aspect of the skin lesions. In early lesions, only subtle perivascular infiltrates composed of smaller blasts, lymphocytes, and histiocytes may be present (Fig. 70.4).
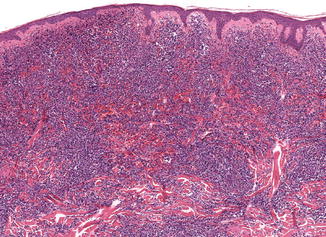
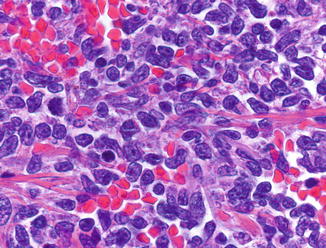
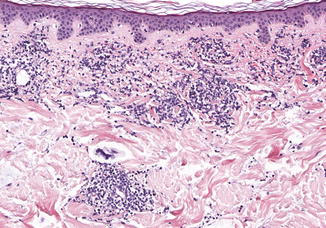
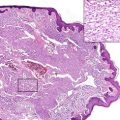
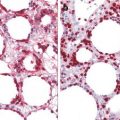
Fig. 70.2
BPDCN: Dense dermal infiltrates of blasts
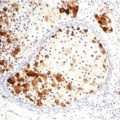
Fig. 70.3
Blasts representing neoplastic Plasmacytoid dendritic cells. Note the extravasated erythrocytes
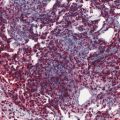
Fig. 70.4
BPDCN: Superficial perivascular infiltrates of blasts, lymphocytes, and histiocytes in a patient with leukemic spread
The tumor cells display a characteristic phenotype with expression of CD4, CD56, CD123, CD303, and TCL-1. Apart from CD123, expression of additional PDC markers such as BDCA-2, BCL11a, and CD2AP can be demonstrated. There is variable expression of TdT. Incomplete phenotypes with loss of markers have been observed. There is no reactivity for B- and T-cell markers except for very rare cases expressing CD3. T-cell receptor genes and immunoglobulin genes are not rearranged. The 9p21.3 (CDKN2A/CDKN2B), 13q13.1-q14.3 (RB1), 12p13.2-p13.1 (CDKN1B), 13q11-q12 (LATS2), and 7p12.2 (IKZF1) regions are commonly deleted in BPDCN.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


