Chapter 4 Biomechanics of Core and Peripheral Tendon Repairs
Outline
Essential Mechanical Requirements of a Surgical Repair
Forces generated during normal hand action range from 1 to 35 N, except tip pinch, according to in vivo measurements.1 Schuind et al1 measured tendon forces up to 6 N during passive mobilization of the wrist, up to 9 N during passive mobilization of the fingers, and up to 35 N during active unrestricted finger motion. Therefore, a surgically repaired tendon should be able to withstand at least 40 N, with power sufficient to resist gap formation. The repair should be able to withstand cyclic loads under both linear and curvilinear load conditions. In vitro laboratory tests have shown that a conventional two-strand core repair plus running peripheral sutures yields a maximal strength of 20 to 30 N2; this is lower than forces generated during normal hand actions and explains why some such repairs are disrupted during postoperative motion exercise. Studies have shown that forces necessary to cause failure of four-strand repairs are around or beyond 40 N3–5; six-strand repairs fail with loads over 50 to 60 N.6,7
Historical Reviews
The main body of information regarding the biomechanics of tendon repair was accrued over the past few decades; the principal contributing research groups are summarized in Box 4-1. The investigatory topics included (1) development of new repair methods; (2) comparisons of existing repairs; (3) factors affecting strength; and (4) new means to test or to record the mechanical properties of the repairs. Human and porcine tendons are the most common materials used in in vitro tests of repair strength,2–5 though tendons from sheep, rabbits, monkeys, and cows are also reported.7,8 Canine, rabbit, and chicken are used in in vivo investigations.9–12
Box 4-1 Groups Contributing to Major Information of Tendon Repair Biomechanics (Listed in Alphabetic Order of the Leading Investigators)
Amadio-Mayo Group: In vitro model: human, canine tendons; in vitro model: canine tendons
Gelberman–St Louis Group: In vitro and in vivo models: canine tendons
Manske–St Louis Group: In vitro model: human, canine tendons; in vivo model: canine, chicken tendons
Mass-Chicago Group: In vitro model and in vivo models: human tendons
Tang-Nantong Group: In vitro model: human, porcine tendons; in vivo model: chicken tendons
Trumble-Seattle Group: In vitro model: human tendons
Wolfe–Yale–New York Group: In vitro model: human tendons
Current Tendon Repair Techniques
Techniques currently available are, first, repair with core and peripheral sutures. Core suture repairs are further divided according to the number of strands passing through the repair site: two-strand (conventional) and multistrand (including four-strand, six-strand, and eight-strand) repairs.2–8,13,14 Alternatively, suture repairs can be categorized by type of tendon–suture junctions: grasping, locking, and mixed grasping-locking repairs. A repair is often referred to using the type of tendon–suture junctions and the number of strands (e.g., a locking four-strand repair). Peripheral sutures include interrupted, simple running, locking running, cross-stitch (Silfverskiöld),15 locking cross-stitch (Dona),16 interlocking horizontal mattress (IHM),16 and horizontal mattress (Halsted) sutures.17 Second, repair can be completed with devices. The use of devices is not common; methods include tendon splints,18 barbed repair devices,19,20 and the Teno Fix device.21,22
Surgical repairs using sutures are the mainstay of current clinical practice. In experimental settings, repairs with use of the above-mentioned devices have yielded impressive strength. The Teno Fix system, a stainless steel rod connecting stainless steel soft tissue anchors with screw threads in each end, was tested in vitro and shown to have strength similar to or greater than a four-strand repair.21 Clinical use of Teno Fix to repair zone 2 flexor tendons has been reported with good outcomes.22 However, Teno Fix is likely to make the tendon bulky and may even impinge upon the already narrow and swollen pulleys, which is a concern. Implanting a stainless steel rod not only risks increasing the volume of the tendon but also may require another operation to remove. A barbed suture device was reported to produce strength equal to a four-strand core suture.19,20 There are similar concerns regarding repair bulkiness. The idea of placing a splint inside the tendon to bridge the cut ends was tested experimentally by Aoki et al,18 but this method has not yet been used clinically.
Types of Tendon–Suture Junctions and Their Strength
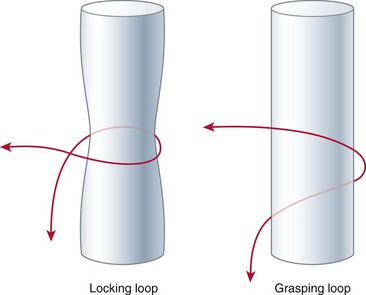
Locking is defined as the configuration that tightens around a bundle of tendon fibers when tensile forces are applied to the suture ends (Figure 4-1).23 In contrast, grasping refers to the configuration that holds the tendon fiber bundles but does not tighten around their entire circumference and tends to pull through the fiber bundles when tensile forces are applied to the suture ends (see Figure 4-1).
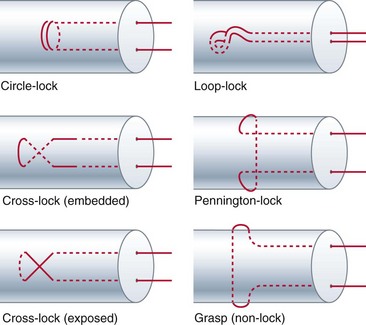
Grasping junctions are either open circle or open loop. Locking junctions include cross-locks (either exposed or embedded), circle-locks (looped or double-circled), and Pennington locks (original or modified) (Figure 4-2). Mechanically, the effectiveness of grasps or locks of a core suture is greatest when (1) suture materials are sufficiently strong—allowing the sutures to grasp or lock the tendon substance tightly without disruption of sutures; (2) the anchor point is sufficiently distant from the tendon laceration—so grasps or locks will not slip; and (3) grasp or lock sizes are sufficient—so the suture anchors to ample tendon substance.
When all the above conditions are met, grasping and locking junctions provide reliable anchors for the suture in the tendon, although a locking repair is generally somewhat stronger than a grasping repair. In practice, when the primary requirements of the repairs are met, the differences in the strength between locking and grasping repairs are actually narrow or insignificant. Depending on the locks or grasps used, the strength of repairs changes (usually less than 10 N).23–29 The increase in strength brought about by incorporation of locking anchors is much smaller than increases in strength through other means—such as increasing the strength of suture materials or the number of suture strands passing through the repair site.2–7 From this perspective, surgeons should pay ample attention to factors that exert the greatest influence on strengths and ensure that these requirements are met primarily. It is not appropriate to rely on incorporating locks, hoping that this measure alone increases strength, while neglecting other more influential factors.
Whether various locks have different mechanical strengths is under question. We tested the strength of the different locks and found they have essentially the same holding power.27 A cross-lock and a circle-lock are identical in holding power; an exposed cross-lock and an embedded cross-lock are the same as well.27 However, our in vitro tests showed that the Kessler-type repairs with the original Pennington locks are weaker than repairs with cross- or circle-locks.28
Pennington locks are frequently incorporated in Kessler-type repairs. Most surgeons believe that Pennington locks help secure the repair. However, this consideration actually lacks sufficient experimental support. According to the definitions of Pennington30 in 1979, in the locking configuration of the Kessler repair, “the transverse suture component passes superficial to the longitudinal component so that the sutures lock a bundle of tendon fibers when tensile forces are applied to the suture.” Pennington did not present its strength data when describing this repair.30 In a letter communication directed to Pennington,31 Silfverskiöld commented regarding this locking repair: “As to Dr. Pennington’s claim that the locking loop design is crucial to the tensile strength of the suture, I agree that in theory this should be true, but in actual practice this may not be the case. … Another practical consideration is that even if one attempts to place the transverse part superficial to the longitudinal part, to create the locking design, it is often difficult to be certain of success.” Practically, we agree that it is difficult for surgeons to ascertain the relation of transverse and longitudinal sutures in the repaired digital tendon clinically.
Hatanaka and Manske9,24 modified the Pennington locking repair by placing some of the longitudinal strands over the dorsal tendon surface, making locked tendon–suture junctions confirmatively. The modified repair is stronger than the grasping Kessler repair when the suture calibers are 2-0 and 3-0 but not 4-0.24 It is noteworthy that in an in vivo setting,9 the strength gained by this modified locking repair was noted only at days 3 and 21, not at days 7 and 14, even with the 2-0 suture. In other words, modified Pennington locks do not improve repair strength during the second week (days 7 to 14), when the tendon stumps usually soften and most ruptures occur. We should be cautious in relying upon Pennington locks to increase strength.
Recently we examined the effectiveness of the original Pennington lock in a four-strand repair; we detected no differences in strength between repairs with the Pennington locks and those with random assignment of grasping and locking. When a two-strand Kessler repair with original Pennington locks was compared with the repair with grasping anchors using 4-0 suture, our tests indicated a modest difference (12%) in gap resistance but no difference in ultimate strength.29 When comparing two grasping anchors (open circle and open loop), we found no difference in their gap resistance and ultimate strength. Taken together, the evidence above leads us to believe that differences between the grasping and the original Pennington’s locking tendon–suture junctions may not be substantial in a clinical setting, and incorporating Pennington locks in multistrand repairs does not appear to affect strength.
Strengths of Core Sutures
Strengths of core sutures have been tested extensively both in vitro and in vivo and in single cycle load-to-failure test2–14,23–28,32–34 or cyclic test setup.35–37 Using a 4-0 nylon suture, a two-strand repair has a strength of about 20 to 25 N, a four-strand repair has a strength of about 35 to 45 N, and a six-strand repair has a strength of about 50 to 70 N. Thus we see the strength is roughly proportionate to the number of strands (Table 4-1).2–8,13,14,32–35 Strength is greatly increased when suture caliber increases36–38 or stronger suture material is used (see Table 4-1).38,39









