Biliary Reconstruction in Children
Ronald T. Cotton
Jacfranz J. Guiteau
John A. Goss
Christine A. O’Mahony
DEFINITIONS
Biliary reconstruction is the final anastomosis performed during liver transplantation, which recreates biliary continuity. In the pediatric population, the choice of reconstructive technique is dependent on many factors including the recipient’s size and anatomy, the type of allograft implanted, as well as the recipient’s underlying disease process.
Duct-to-duct biliary reconstruction is defined as creation of either a hepaticocholedochostomy or choledochocholedochostomy. Most commonly, this technique is used with whole organ allografts but can also be employed with split and reduced-size grafts.
A hepaticojejunostomy is the creation of a Roux-en-Y hepaticojejunostomy during implantation of a whole or partial allograft. This is performed when the patient’s underlying disease process renders the common bile duct either absent or unsuitable for anastomosis, a significant size discrepancy exists between donor and recipient bile ducts, or the recipient is small (<10 kg) with a resultant small native common bile duct.
A split graft refers to either the in situ or ex vivo separation of the right and left lobes of the donor liver for implantation into two separate recipients. Most commonly, the left lateral segment is used in pediatric recipients. Biliary reconstruction for left lateral segment grafts is performed via Roux-en-Y hepaticojejunostomy. Right-sided grafts can be reconstructed via hepaticojejunostomy or duct-to-duct anastomosis.
Similarly, reduced-size grafts are divided in situ or ex vivo into right and left lobes. Here, the left lobe is implanted into the pediatric or small adult recipient, and the remaining allograft is discarded. Biliary reconstruction is performed using Roux-en-Y hepaticojejunostomy for left-sided grafts and either Roux-en-Y hepaticojejunostomy or duct-to-duct anastomosis on the right.
In living related donor transplantation, either a left lobectomy or lateral segmentectomy is performed in the donor, and the procured lobe or segment is implanted into the recipient. Similar to the reduced-size and split grafts, left hepaticojejunostomy is used for biliary reconstruction.
DIFFERENTIAL DIAGNOSIS
Orthotopic liver transplantation is the definitive management of a wide variety of pediatric liver diseases. Current indications in this population include acute and chronic hepatic failure, inborn errors in metabolism, secondary liver disease, and primary hepatic malignancy.1 A summary of associated diseases leading to transplantation in this population is provided in Table 1. The suspected etiology of liver dysfunction may determine selection of the technique for biliary reconstruction in the recipient.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Laboratory studies including serum chemistries, complete blood count, liver function tests, blood and body fluid cultures, blood typing, and viral serologies are useful in the evaluation of the deceased donor. Additionally, liver biopsy is used selectively to evaluate an organ’s suitability for transplantation.
With the exception of select indications including trauma and known choledochocele, dedicated liver imaging or cholangiography is rarely necessary prior to organ procurement to assess biliary anatomy.
Similar to the recipient, the potential living donor receives an extensive diagnostic workup prior to consideration for transplantation. Cross-sectional imaging including computed tomography (CT) and magnetic resonance imaging (MRI) are used to delineate liver size and arterial and biliary anatomy. Intraoperative cholangiography is occasionally performed during liver donor hepatectomy to clearly define plains of transection.2 Information gathered from these tests is invaluable in preoperative planning of biliary reconstruction.
SURGICAL MANAGEMENT
The abdomen is approached via a bilateral subcostal (chevron) incision. Occasionally, midline extension is necessary for larger children.
A self-retaining retractor, commonly a Thompson liver transplant retractor (Thompson Surgical Instruments Inc, Traverse City, MI), is placed to aide in exposure.
Biliary reconstruction is the final step of a liver transplant. Prior to the biliary anastomosis, the patient would have received a total hepatectomy as well as caval, portal, and hepatic arterial reconstructions.
Table 1: Indications for Pediatric Liver Transplantation | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TECHNIQUES
DUCT-TO-DUCT BILIARY RECONSTRUCTION
Cholecystectomy and Transection of the Donor Biliary Tree
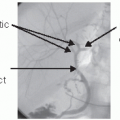
Prior to biliary reconstruction, perform a retrograde donor. Trim the common bile duct with Metzenbaum scissors to healthy, well-vascularized tissue. The length of duct remaining should comfortably reach the recipient’s native common bile duct without tension or redundancy (FIG 1). If there is tension or difficulty with reach, the abdominal wall retractors should be relaxed slightly to move the liver inferiorly. Alternately, laparotomy pads can be placed above the liver to push the allograft down.
The blood supply to the hepatic and common bile ducts run at the 3 o’clock and 9 o’clock positions. Once the duct is divided, these vessels are ligated with 8-0 Prolene suture applied in an interrupted figure-of-eight fashion. Electrocautery is avoided to prevent tissue injury and resultant stricture.
Choledochocholedochostomy
The vascular anastomoses are again inspected to assure both hemostasis and adequate flow. Excessive manipulation of the allograft after biliary reconstruction can injure the ductal anastomosis.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree