Most common bacterial skin infections are caused by coagulase-positive Staphylococcus aureus or group A beta-hemolytic streptococci. Before the widespread availability of antibiotics, many common skin infections resulted in serious illness and even death. In the 1950s following the widespread use of antibiotics, most staphylococcal and streptococcal skin infections responded well to the use of the penicillins. However, scattered cases of methicillin-resistant Staphylococcus aureus (MRSA) were already being reported by the early 1960s. From late 1960s to the mid-1990s, MRSA infections became a major problem especially in large urban hospitals. In the past decade, hospital-acquired MRSA infections began to decrease as hospitals instituted more aggressive infection control measures, but during that same time community-acquired MRSA infections increased.
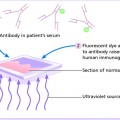
Syphilis has been called “the great masquerader” and “the great imitator” based on the many varied presentations of the cutaneous and other organ system findings. Patients with secondary syphilis usually present with rashes that mimic common papulosquamous skin diseases, but can present with skin findings that mimic almost any cutaneous disorder.
Impetigo is a common, highly contagious, superficial skin infection that presents with either a bullous or nonbullous appearance. Nonbullous impetigo accounts for the majority of cases. It occurs in children of all ages, as well as adults, whereas the bullous form is most common in newborns. Impetigo is limited to the epidermis.
Coagulase-positive Staphylococcus aureus is the most common cause of bullous and nonbullous impetigo. Group A beta-hemolytic streptococci including the nephritogenic strains may also cause impetigo.1,2
Nonbullous impetigo represents a host response to the infection, whereas staphylococcal toxin causes bullous impetigo and no host response is required to manifest clinical disease.3
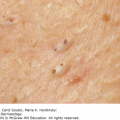
Nonbullous impetigo begins as a single lesion typically manifesting as a red macule or papule that quickly becomes a vesicle. The vesicle ruptures, forming an erosion and the contents dry to form the characteristic honey-colored crust commonly seen with impetigo (Figure 12-1). Nonbullous impetigo usually occurs on the face or extremities. Impetigo may occur concomitantly with herpes simplex and atopic dermatitis.
Bullous impetigo begins as a superficial vesicle that rapidly progresses to a flaccid bulla, with sharp margins and no surrounding erythema. When the bulla ruptures, a moist yellow crust forms. Impetigo is often spread to surrounding areas by autoinoculation. Bullous impetigo usually arises on grossly normal skin and favors moist intertriginous areas, such as the diaper area, axillae, and neck folds.
Ecthyma is an uncommon variant of impetigo that initially presents as a typical impetigo infection that spreads into the dermis. It usually presents on the lower legs with thick crusts overlying superficial ulcers. It is more common in young children, immunosuppressed patients, and in patients with poor hygiene.

Bacterial cultures from the infected areas are usually positive for S. aureus or streptococci.
The key diagnostic clinical features of impetigo are honey-colored crusts or bullae.
✓ Herpes simplex: Presents with grouped vesicles on the lips, perioral, and genital region.
✓ Atopic dermatitis: Presents with pruritic, scaly, or crusted papules and plaques in patients with a history of atopy.
✓ Varicella (chicken pox): Presents with fever and widespread vesicles with surrounding erythema.
✓ Other: Perioral dermatitis, insect bites, tinea infections, abrasions, lacerations, thermal burns, erythema multiforme, dermatitis herpetiformis, burns, bullous fixed drug eruptions, staphylococcal scalded skin syndrome, bullous tinea pedis, and bullous insect bites. In adults, bullous pemphigoid and pemphigus are in the differential.
The superficial crusts should be removed with gentle cleansing with an antibacterial soap. Wet dressings could also be applied to remove thicker crusts (Table 6-5). Localized impetigo can be treated with topical medications including:
Bacitracin ointment 3 times a day for 3 to 5 days.
Mupirocin (Bactroban) ointment 3 times a day for 3 to 5 days.
Retapamulin (Altabax) ointment twice a day for 5 days.
Severe or more widespread impetigo may require oral antibiotics, such as first-generation cephalosporins, dicloxacillin, amoxicillin/clavunate, or azithromycin.1,3 Impetigo usually responds well to treatment, but may be recurrent.
Severe or persistent disease that does not respond to therapy.
PubMed Health: www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001863/
A boil (furuncle) is a deep-seated inflammatory nodule that develops around a hair follicle, often from a preceding more superficial folliculitis. A carbuncle is two or more confluent boils.
Coagulase-positive Staphylococcus aureus (SA) is the most common cause of boils and carbuncles. The organism may be methicillin sensitive (MSSA) or methicillin resistant (MRSA).
MRSA infections may be acquired in health care facilities such as hospitals and nursing homes or now more commonly in the community. In one study of 12 United States’ emergency departments, MRSA infections were responsible for 38% to 84% of purulent skin and soft tissue infections.4
Patients usually give a history of a rapidly enlarging tender “pimple” or boil. The patient may give a history of risk factors such as crowded living conditions, infected family members, diabetes, obesity, atopic dermatitis, or inherited or acquired immune deficiency.
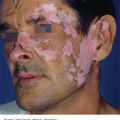
A boil starts as a hard, tender, red, follicular centric nodule. The nodule enlarges and becomes painful and fluctuant after several days (Figure 12-2). Rupture may occur, with extrusion of pus.

Cultures from pus within the lesion or from drainage are usually positive for MSSA or MRSA.
The key diagnostic clinical feature of a boil is a tender, fluctuant cyst or nodule.
✓ Ruptured epidermal inclusion cyst: This may very closely resemble a staphylococcal boil, but when lanced, the cyst contains thick white keratinous material.
✓ Acne cyst: This may also closely resemble a staphylococcal boil, but other signs of acne such as comedones should be present.
✓ Hidradenitis suppurativa: Presents with cysts limited to intertriginous areas of the body.
✓ Other: Deep fungal infections, dental abscess, kerion.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


