Key Points
- •
Resorption may be less with autogenous lower lid spacers.
- •
Ear cartilage is very effective but may be visible over time.
- •
Allogeneic spacers avoid donor site morbidity.
- •
Acellular human dermis should be thick in order to minimize resorption.
- •
Acellular porcine dermis has been used with high success.
- •
Higher rates of infection and extrusion are associated with alloplastic spacers.
- •
Lateral canthoplasty should be combined with spacer placement.
Introduction
Lid malposition is one of the most common complications following lower blepharoplasty. Treatment options are conservative management including liberal use of ophthalmic ointment to prevent corneal exposure as well as massage and taping the eyes closed at night. Corneal exposure evident on slit lamp examination may require a temporary tarsorraphy suture to improve symptoms. Although early severe ectropion with corneal exposure may require immediate re-operation, generally a 6 week period of conservative treatment is recommended since most patients will improve without re-operation. If surgical revision is required, the best timing for surgery is initial placement of a temporary tarsorraphy during the first 2 weeks followed by definitive correction with lower lid spacer after 6 weeks. A minimum period of 2 months should be observed in order to allow reduction in inflammation of the periorbital tissues prior to reoperation.
Traditional autogenous spacer grafts used for posterior lamellar support include ear cartilage, hard palate, rib cartilage, temporalis fascia, and occasionally nasal septum. Allogenic spacers including human and porcine acellular dermal matrix eliminate the disadvantage of morbidity associated with a donor site. The most commonly used allogeneic spacers include AlloDerm® (human) and EnduraGen® (porcine). Alloplastic lower lid spacers are reserved for severe recurrent ectropion which has failed autogenous or allogeneic spacer placement due to tissue resorption.
Patient selection
Patients can be divided into several subgroups. Patients who have primary lower blepharoplasty when combined with lateral canthopexy have a low risk of lid malposition. If scleral show or ectropion occurs after primary lower blepharoplasty, the causes include technical failure of the lateral canthopexy, excessive swelling, hematoma, scar contracture, or over-resection of skin. The majority of these patients will improve with conservative management including lower lid upward massage and taping with flesh colored Steri-Strips® to minimize visibility of the tape ( Figure 16.1 ). Patients with symptomatic corneal exposure may undergo immediate revision of the lateral canthopexy if technical failure is suspected to minimize the time of morbidity associated with conservative management. An alternative includes temporary tarsorraphy placed under local anesthesia in the clinic and left in place for 6 weeks ( Figure 16.2 ).


If lid position does not improve, re-operation can be performed after 6 weeks. The second subgroup includes patients who have had prior blepharoplasty and present for secondary correction of ectropion. These patients have been found to have a significantly higher incidence of reoperation compared to primary patients and should be considered for placement of lower lid spacer grafts. Lateral canthoplasty should be performed at the time of spacer graft placement and may require drill hole canthoplasty to provide stable bony fixation of the lateral canthus. If the integrity of the tarsoligamentous sling is not suitable for lateral canthal sutures due to scarring, the tarsoligamentous sling can be completely reconstructed with a tensor fascia lata sling. This adds additional support to the retracted lower lid.
Indications
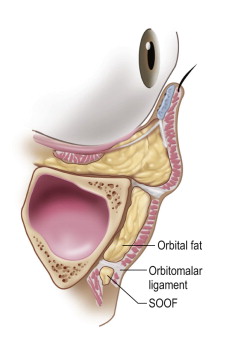
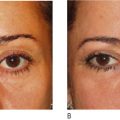
The indications for lower lid spacer graft placement include lower lid malposition and ectropion which require additional vertical elevation of the lid above that which can be created with lateral canthal support alone. The vector of vertical elevation of the central portion of the lower lid is limited by lateral canthoplasty and at a certain point will create an overly corrected lateral canthus with a canthal tilt which is too high and unnatural in appearance ( Figure 16.3 ). At this point, the addition of a posterior lamellar spacer graft for patients without anterior lamellar shortage should be considered. Recruitment of skin into the lower lid to correct mild anterior lamellar shortage is performed at the time of the spacer graft placement with release of the orbitomalar ligament and midface elevation ( Figure 16.4 ).
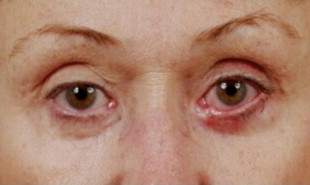
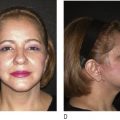
Severe shortage of the anterior lamella may require skin grafting. One additional group of patients who present for aesthetic surgery of the eyelids who may require lower lid spacer grafts includes patients with a negative vector, prominent eyes and Graves’ disease who have developed lid retraction ( Figure 16.5 ). While these patients are primary surgical patients, the risk of lower lid malposition is significantly increased due to the unfavorable morphology of the eyelids and globe, making ectropion high risk after blepharoplasty. These patients should be carefully evaluated for use of primary lower lid spacer grafts at the time of blepharoplasty.

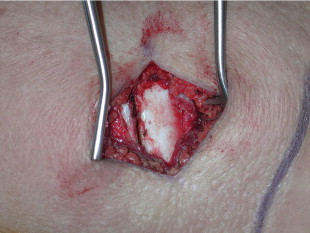
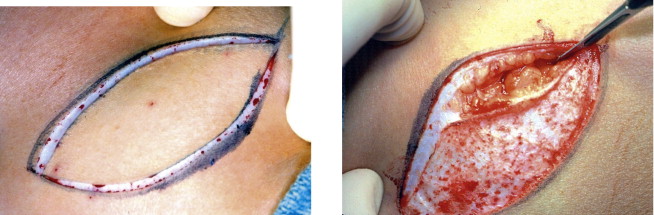
The historical spacer graft that was used in eyelid surgery was preserved banked sclera. A variety of autogenous grafts have been used including rib cartilage, ear cartilage, nasal septal cartilage, hard palate mucosa, dermis, temporalis fascia and tensor fascia lata ( Figures 16.6, 16.7, 16.8 ). A significant advantage of autologous tissue is minimal resorption. However, in some cases the surgeon is limited by the amount of tissue available and the morbidity associated with a donor site. Ear cartilage and tensor fascia lata grafts have evolved over time as the autologous grafts of choice.

In order to avoid donor site morbidity, allogeneic or alloplastic materials, which include human cadaveric acellular dermis (Alloderm®) or porcine acellular dermal matrix (EnduraGen®), have been used with success ( Figure 16.9 ). While the advantages include the lack of a donor site and little graft visibility compared to ear cartilage grafts, the disadvantages include variable resorption and infection. For more severe case, alloplastic lower lid spacers have been used and can span the lower lid and the infraorbital rim. High density polyethylene (Medpor®) has been used with limited experience ( Figure 16.10 ). The risk of infection and exposure requiring revision or removal may occur. In addition, complications include creation of a static lower lid which impairs the inferior visual field on downgaze such as in reading and while walking down stairs.

Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


