(1)
Department of Anatomy, Medical School Democritus University of Thrace, Alexandroupolis, Evros, Greece
Abstract
The auricle is a morphologically unique, highly variable in size and shape structure and a predominant feature of the face. Along with the external acoustic meatus, it constitutes the external ear. The auricle consisted of a cartilaginous skeletal structure that is covered by a cutaneous investor, which conforms to its shape.
The auricle is supplied by a rich anastomotic network that is formed by branches of the posterior auricular and the superficial temporal vessels. Only a few, simply designed flaps can be derived from the auricle, and these are provided to reconstruct small defects of the auricle itself.
The auricle (pinna) together with the external acoustic meatus constitutes the external ear. It is a morphologically unique, highly variable in size and shape structure and a predominant feature of the face.
7.1 Anatomy of the Auricle
The auricle consisted of an elaborate cartilaginous skeletal structure that is covered by a cutaneous investor, which conforms to its shape.
The convex and concave elements of the cartilaginous framework are responsible for the configuration of the auricle and correspond to the landmarks of the auricle (Fig. 7.1).
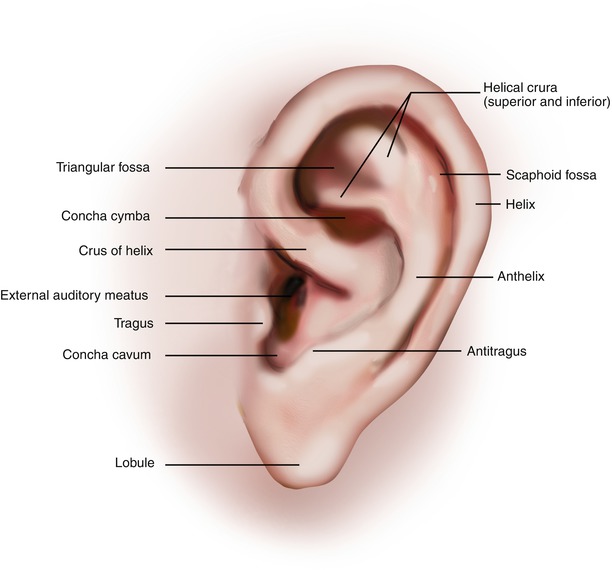
Fig. 7.1
Topographic landmarks of lateral surface of auricle
7.1.1 Skin and Subcutaneous Tissue
The skin that covers the auricle is very thin with minimal subcutaneous tissue. It attaches to the underlying cartilage and exhibits surgically important differences between the lateral and cranial (medial) surfaces of the auricle. The skin of the lateral surface firmly adheres to the perichondrium with reduced mobility, and the subcutaneous tissue is scant (Fig. 7.2). The attachment of the skin to the cartilage increases as it passes across the concha to continue into the external auditory meatus.
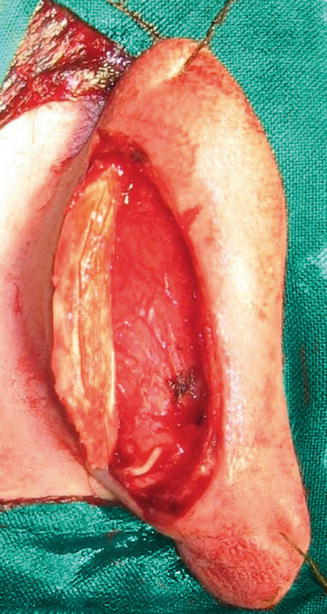
Fig. 7.2
The skin of the lateral surface of the auricle is almost devoid of subcutaneous tissue
At the cranial surface of the auricle, the skin is thicker and less adherent to the perichondrium, with greater mobility, and more subcutaneous tissue is present (Fig. 7.3). The lobule contains no cartilaginous structure and consisted solely of skin and subcutaneous fatty tissue.

Fig. 7.3
At the medial surface of the auricle, the skin is thicker and more subcutaneous tissue is present
7.1.2 Muscles
The musculature of the external ear includes extrinsic and intrinsic muscles. The extrinsic muscles are three very thin fans of muscle fibers that form the auricularis anterior, auricularis superior, and auricularis posterior muscles (Fig. 7.4). They are encompassed by the temporoparietal fascia and connect the auricle to the scalp and the skull (see Chap. 2). The anterior and posterior ligaments reinforce the attachment of the external ear to the skull.

Fig. 7.4
Extrinsic auricular muscles
The intrinsic muscle group includes the helicis major, helicis minor, tragicus, antitragicus, transversus auriculae, and obliquus auricular muscles. These muscles are highly variable and often underdeveloped. Seldomly, they can be seen grossly as very thin and scattered muscle fibers. All of these muscles are innervated by the temporal and the posterior auricular branches of the facial nerve.
7.1.3 Vascular Anatomy
The arterial supply of the auricle is provided by a rich anastomotic network that is formed by branches of the posterior auricular and the superficial temporal arteries (Fig. 7.5). The posterior auricular artery has been found to be the dominant blood supply for the auricle (Park et al. 1992; Imanishi et al. 1997; Pinar et al. 2003).
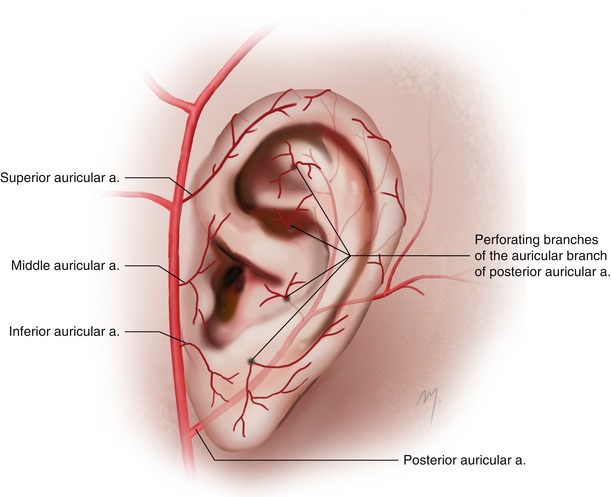
Fig. 7.5
Arterial vascularization of the auricle
The superficial temporal artery gives rise to three small branches that travel to the anterior part of the lateral auricular surface. These branches are the superior, middle, and inferior auricular arteries and are distributed to the anterior and lateral aspects of the auricle. The superior auricular artery enters the helical root and continues along the margin of helix (“helical artery”) and communicates with the posterior auricular artery forming an arterial arcade (“helical arcade”) (Song et al. 1996; Moschella et al. 2003; Erdmann et al. 2009).
The posterior auricular artery after branching from the external carotid artery ascends and divides into the occipital and auricular branches. The auricular branch courses along the retroauricular sulcus passing beneath the posterior auricular muscle and gives off three branches to the cranial surface of the auricle. These branches further subdivide giving off twigs that run to the free margin of the helical rim and pass round it to the lateral surface and others that penetrate the cartilage reaching also the lateral surface. Through these perforators the posterior auricular artery participates in a great degree in the vascularization of the lateral surface of the auricle. Park et al. (1992) found out that major perforators of the posterior auricular artery appear at the anteroauricular surface at the triangular fossa, the cymba cocha, the helical root, the cavum cocha, and the earlobe.
Venous drainage of the auricle accompanies the arterial supply. The posterior auricular veins drain into the external jugular vein, while the anterior auricular veins drain into the superficial temporal and posterior facial veins.
7.1.4 Sensory Innervation
The auricle is innervated from the great auricular nerve, the lesser occipital nerve, and the auriculotemporal nerve (Fig. 7.6).
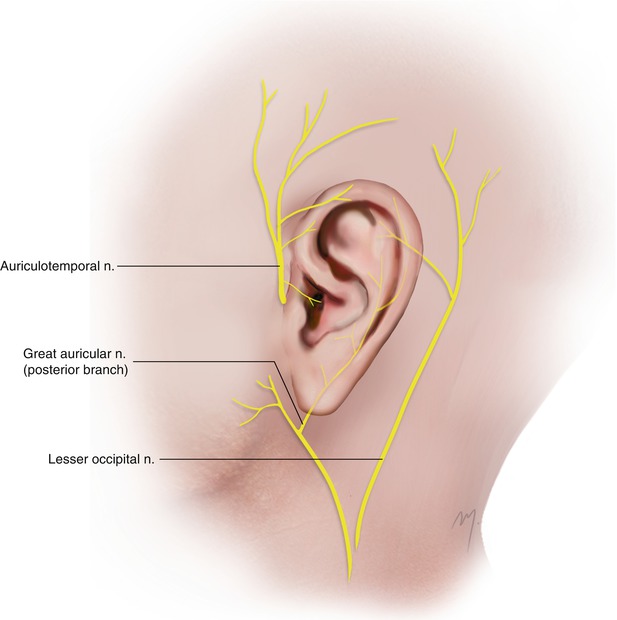
Fig. 7.6
Sensory innervation of the auricle
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


