Introduction
The external ear is formed by the auricle, external acoustic meatus, and tympanic membrane. The auricle is a concave structure that directs sound waves into the external acoustic meatus. It is also cosmetically important and its anatomical structures are extremely complicated and delicate.
The external ear is a focus of otologic and plastic surgery, but it is also important in neurologic and lateral skull-base surgery. Surgery resulting in cosmetic and functional satisfaction relies not only on the surgeon’s skill and use of advanced technologies but also on their complete understanding of the area’s microsurgical anatomy, which makes surgery gentler and safer.
This chapter examines the microsurgical anatomy of the auricle and external acoustic meatus in cadaveric dissections and organizes the results in the following sections: (1) bone structure, (2) auricle, (3) cartilaginous skeleton of the auricle, (4) external acoustic meatus, (5) muscles, (6) neural innervation, (7) vascular supply, and (8) fascial structure. Finally, there is a short description of clinical considerations.
Bone Structure
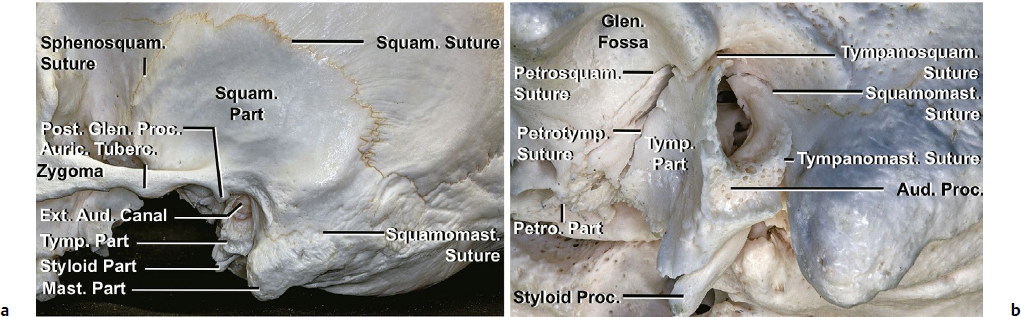
The temporal bone consists of five components: squamous, tympanic, petrous, mastoid, and styloid parts (Fig. 18.1a). The bony canal of the external acoustic meatus is composed of three parts of the temporal bone: squamous, tympanic, and mastoid. The anterior and inferior bony walls are formed by the tympanic part. The superior and posterior bony walls are formed by the squamous and mastoid parts, and the squamomastoid suture can be identified (Fig. 18.1b). The tympanic part produces three sutures: tympanosquamous, tympanomastoid, and petrotympanic. The tympanosquamous suture, between the squamous and tympanic parts, is continuous medially with the petrotympanic and petrosquamous fissures (Fig. 18.1b). Additionally, two spines are identified in the bony portion of the meatus: endomeatal and suprameatal spines. The suprameatal spine (Henle’s spine) is situated at the upper and posterior part of the orifice of the external acoustic meatus. The endomeatal spine is formed by a projection of the tympanosquamous suture into the canal.
The posterior root of the zygomatic arch of the squamous part forms the roof of the external acoustic meatus. At the anterior edge of this roof, the postglenoid process is positioned between the mandibular fossa and anterior wall of the external acoustic meatus. The tympanosquamous suture runs between the postglenoid process and the tympanic part of the temporal bone.
The edge of the tympanic membrane is thickened to form a fibrocartilaginous ring (tympanic annulus) attached to the tympanic sulcus, an incomplete ring of the tympanic bone that is interrupted by the notch of Rivinus. Above the superior end of the tympanic sulcus, the tympanic annulus becomes a fibrous band. The tympanic membrane within the notch of Rivinus, above the anterior and posterior malleolar folds extending to the lateral process of the malleus, is called the pars flaccida. This part is closely related to the anterior and posterior canal for the chorda tympani and the petrotympanic suture.
Auricle
The auricle is the lateral-most part of the external ear and is composed mainly of cartilage and skin. It is divided into two surfaces: lateral and medial.
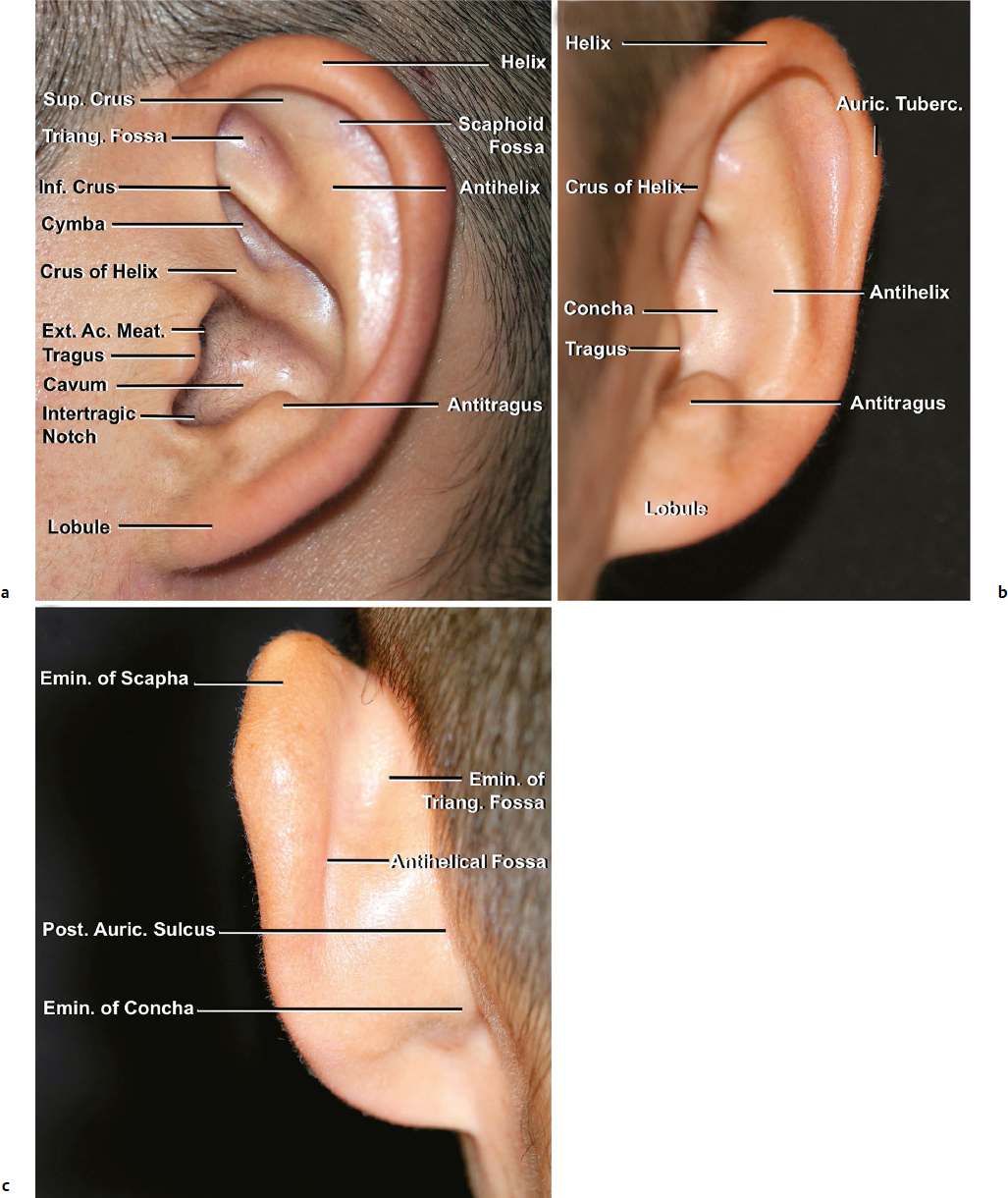
The lateral surface is covered by a thin layer of skin, which is formed mainly by the perichondrium and an extremely fine subcutaneous layer. On this surface, the marginal edge is formed mainly by the helix, which is a smooth and round arch. The helix starts at the crus of the helix, passes anterosuperiorly, turns posteriorly and then inferiorly, and finally ends at the helical tail, which is continuous with the lobule. The scaphoid fossa is located just anterior to the helix along most of its length (Fig. 18.2a,b).
Next to the entrance of the external acoustic meatus, a well-defined hollow, the concha, leads into the meatus. This hollow has two parts: the cymba and the cavum conchae, separated by the crus of the helix. The antihelix, which has a Y shape, passes upward anterior to the posterior rim of the helix and divides into superior and inferior crura, separated by the triangular fossa. The root of the inferior crus of the antihelix forms the sharp rim of the concha and separates it from the triangular fossa. The superior crus of the antihelix forms the anterior border of the scaphoid fossa. The tail of the antihelix joins the antitragus. The inferior crus, tragus, and antitragus overhang the concha, making it look smaller. The well-defined notch between the tragus and antitragus is called the intertragic notch.
The skin of the medial surface is thicker than that of the lateral surface. On the medial surface, the prominences and sulci follow an obviously inverse pattern to that on the lateral surface (Fig. 18.2c). From the medial view, the concha and fossa on the lateral surface are seen as eminences, and the crura are seen as grooves. Eminences include the scaphoid, triangular, and conchal eminences. The antihelix on the lateral surface forms a depression on the medial surface called the antihelical fossa.
The most inferior part of the auricle is the lobule. The lobule is soft, formed mainly by fatty tissue between two cutaneous layers. The main defining feature of this area is the lack of cartilage, which makes the reconstruction of the lobule difficult because of postoperative retraction.
Cartilage
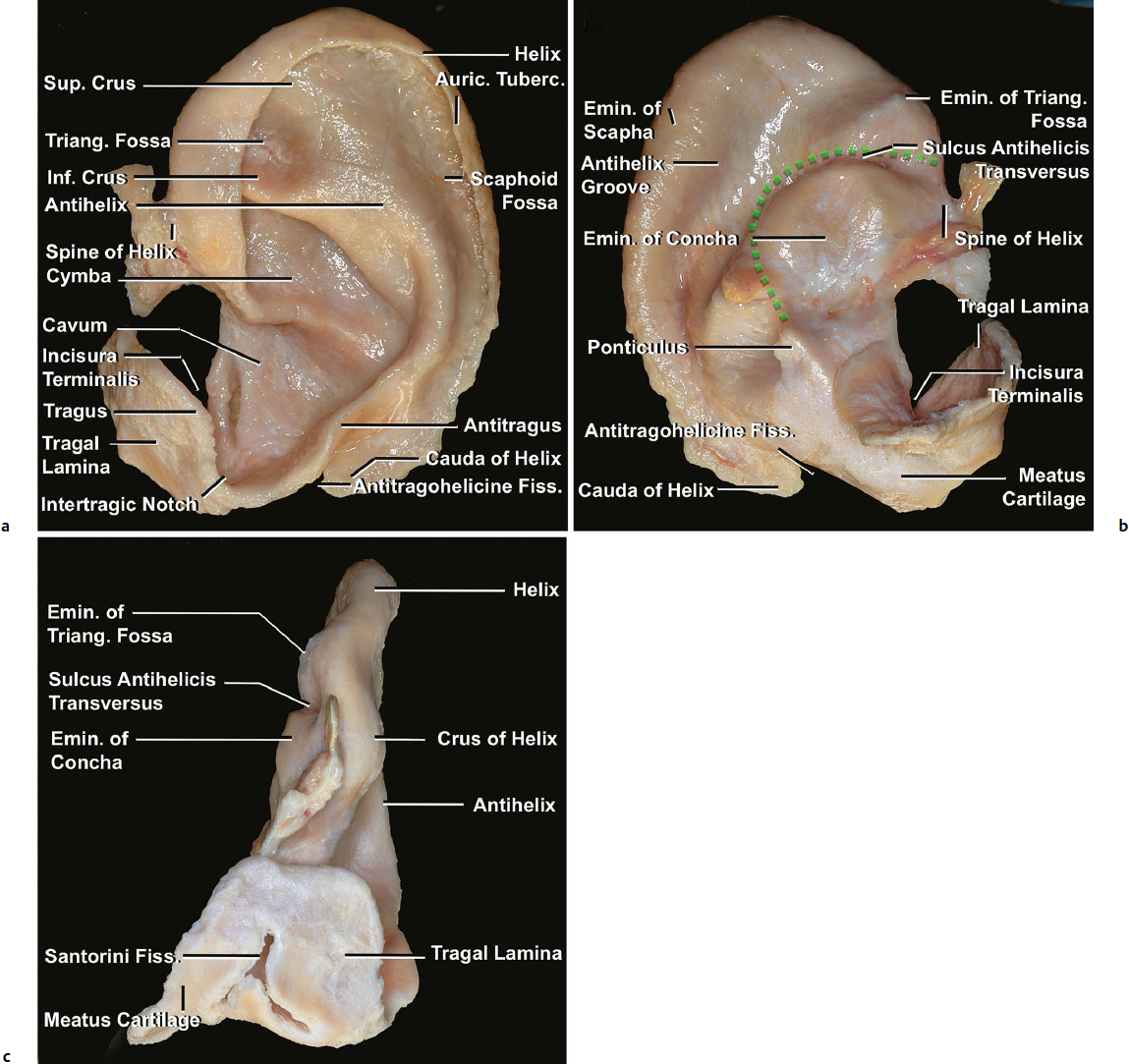
The entire auricle except the lobule has elastic cartilage as its framework (Fig. 18.3). This cartilage allows the auricle to be flattened, bent, and folded. Repair of cartilage defects and reconstruction of the auricle remain challenging because the cartilage is a unique tissue without its own vascularization. A thin, adherent layer of perichondrium covers the auricular cartilage and can be separated from it; however, this perichondrium is more adherent in some lesions to the fossae.
The cartilage is strikingly similar to the surface of the auricle. Convexities on the lateral surface of the auricle include the helix, antihelix, superior and inferior crura of the antihelix, crus of helix, tragus, and antitragus. Concavities include the triangular fossa, cymbal and cavum conchae, and scaphoid fossa. The depressions and elevations on the lateral surface are aligned with the elevations and depressions on the medial surface.
From the surface of the auricle, some cartilaginous structures that are not seen are the incisura terminalis, ponticulus, antitragohelicina fissure, cauda of the helix, cartilage of the external acoustic meatus, and spine of the helix. The incisura terminalis separates the tragal lamina, which is the vertical curved plate of the tragus, and the cartilage of the external acoustic meatus from the main auricular cartilage. The lower part of the helix continues downward as a process called the cauda of the helix. The cauda of the helix is separated from the antitragus by a deep fissure, the antitragohelicine fissure. The spine of the helix is the anterior extremity of the crus of the helix. The ponticulus is the vertical ridge crossing the eminence of the concha on the medial surface. A deep groove can be identified on the medial surface between the eminences of the triangular fossa and concha. This deep groove is called the transverse sulcus of the antihelix and corresponds to the antihelix and its inferior crus on the lateral surface.
The cartilage of the external acoustic meatus forms a semicanal that extends medially from the lateral lamina of the tragus. This cartilaginous semicanal is usually interrupted by two vertical fissures in the anterior portion of the cartilage (Santorini fissures). These fissures can allow infections and malignant tumors to extend between the external acoustic meatus and parotid gland.
The cartilage of the auricle is attached to the auditory process, which is the lateral edge of the tympanic part of the temporal bone and has an extremely rough surface (Fig. 18.1b), and fixed to the skull by three ligaments: anterior, superior and posterior. The anterior ligament attaches the helix and tragus to the zygomatic process. The superior ligament attaches the spine of the helix to the superior margin of the bony external auditory canal. Furthermore, the posterior ligament is located between the medial surface of the concha and the mastoid process.
External Acoustic Meatus
The external acoustic meatus extends from the bottom of the concha to the tympanic membrane, forming an S shape that is divided into cartilaginous and bony portions (Fig. 18.4). First, it extends medially and slightly anteriorly and superiorly, then it turns medially and slightly posteriorly (cartilaginous part), and finally passes medially, anteriorly and slightly inferiorly (bony part). Pulling the auricle posteriorly and superiorly makes the canal straight and provides better visualization of the tympanic membrane.
The external canal has two narrow portions. One is close to the inner end of the cartilaginous portion (cartilage-bony junction), and the other is the isthmus in the osseous portion. The isthmus is the narrowest point along the canal and is located not at the cartilage-bony junction but in the bony portion.
The cartilaginous portion is continuous with the cartilage of the auricle and attaches to the auditory process, where the cartilage is attached medially to the bony part with dense connective tissue (Fig. 18.1b). The posterior and superior part of the cartilaginous part actually lacks cartilage but is filled with fibrous tissue.
The bony portion is narrower than the cartilaginous portion. The conically shaped tympanic membrane is located at the medial end of the meatus and is titled anteroinferiorly. The angle between the tympanic membrane and the anteroinferior bony wall (anterior tympanomeatal angle) is acute and often obstructed by the bony eminence of the anterior wall.
The tympanic membrane is composed of three layers. The lateral epithelial layer is continuous with the skin of the external acoustic meatus. The middle fibrous layer is called the lamina propria, which is not identified in the pars flaccida. The medial mucosal layer is continuous with the mucosa of the middle ear cavity.
The skin covering the meatus is visibly thin, though slightly thicker on the cartilaginous portion than the bony portion, and it adheres closely to the cartilaginous and osseous portions of the meatus. The skin of the bony portion has no hair or glands. In the cartilaginous part, the subcutaneous tissue has hair follicles and ceruminous and sebaceous glands, which secrete the yellowish brown earwax.1,2 In the auricle, the sebaceous glands are predominant in the concha and triangular fossa; ceruminous glands are located around the orifice of the external acoustic meatus.3,4
In three regions, the skin is more firmly adherent to the bony canal: (1) supra meatal spine (Henle’s spine), (2) tympanomastoid suture, and (3) endomeatal spine and tympanosquamous suture. These sutures and spines make elevating a tympanomeatal flap from the bony canal difficult.
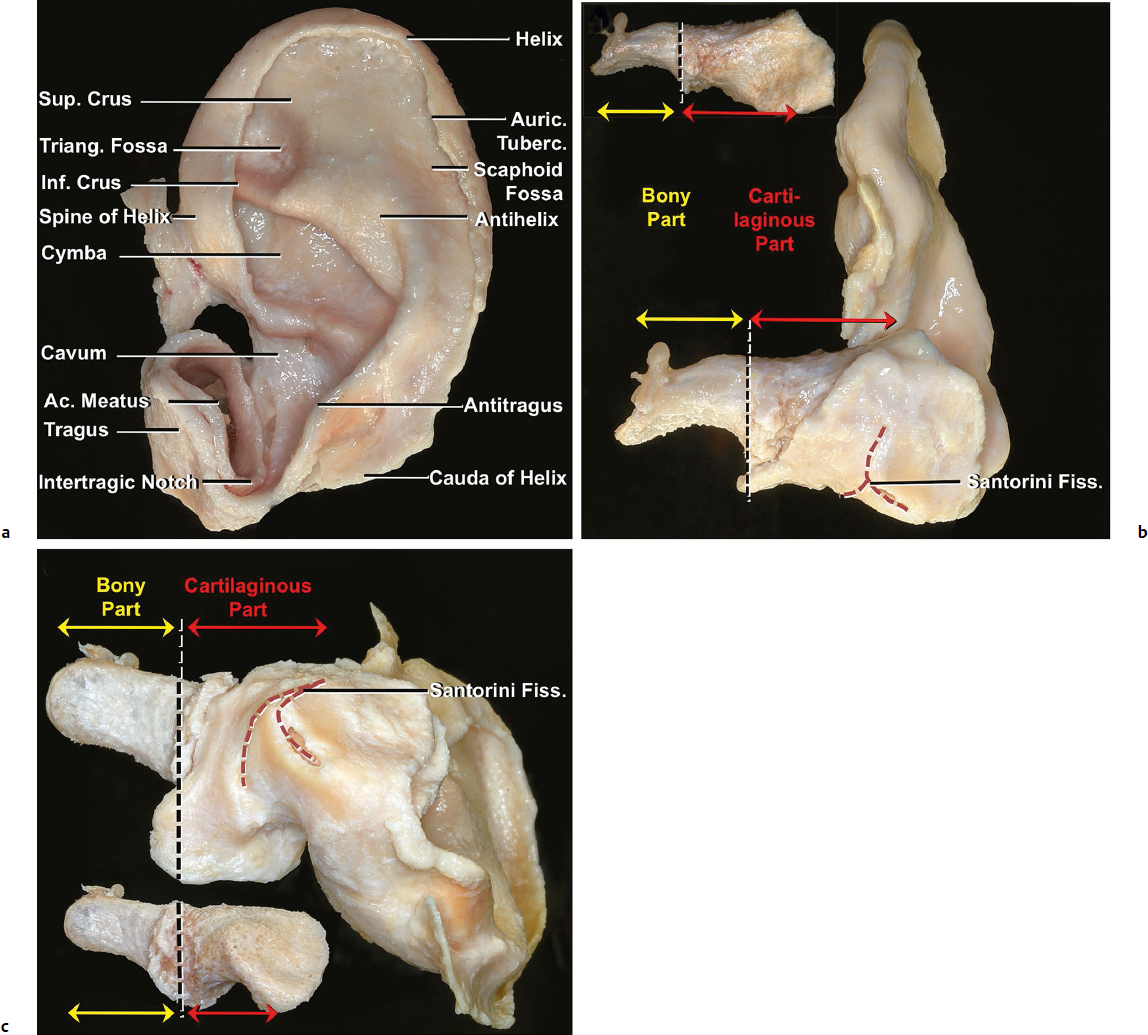
Fig. 18.4 Anatomy of the external acoustic meatus. (a) Lateral view; (b) anterior view; (c) inferior view. Ac., Acoustic; Auric., auricular; Fiss., fissure; Inf., inferior; Sup., superior; Triang., triangular; Tuberc., tubercle.
Muscle and Facial Nerve
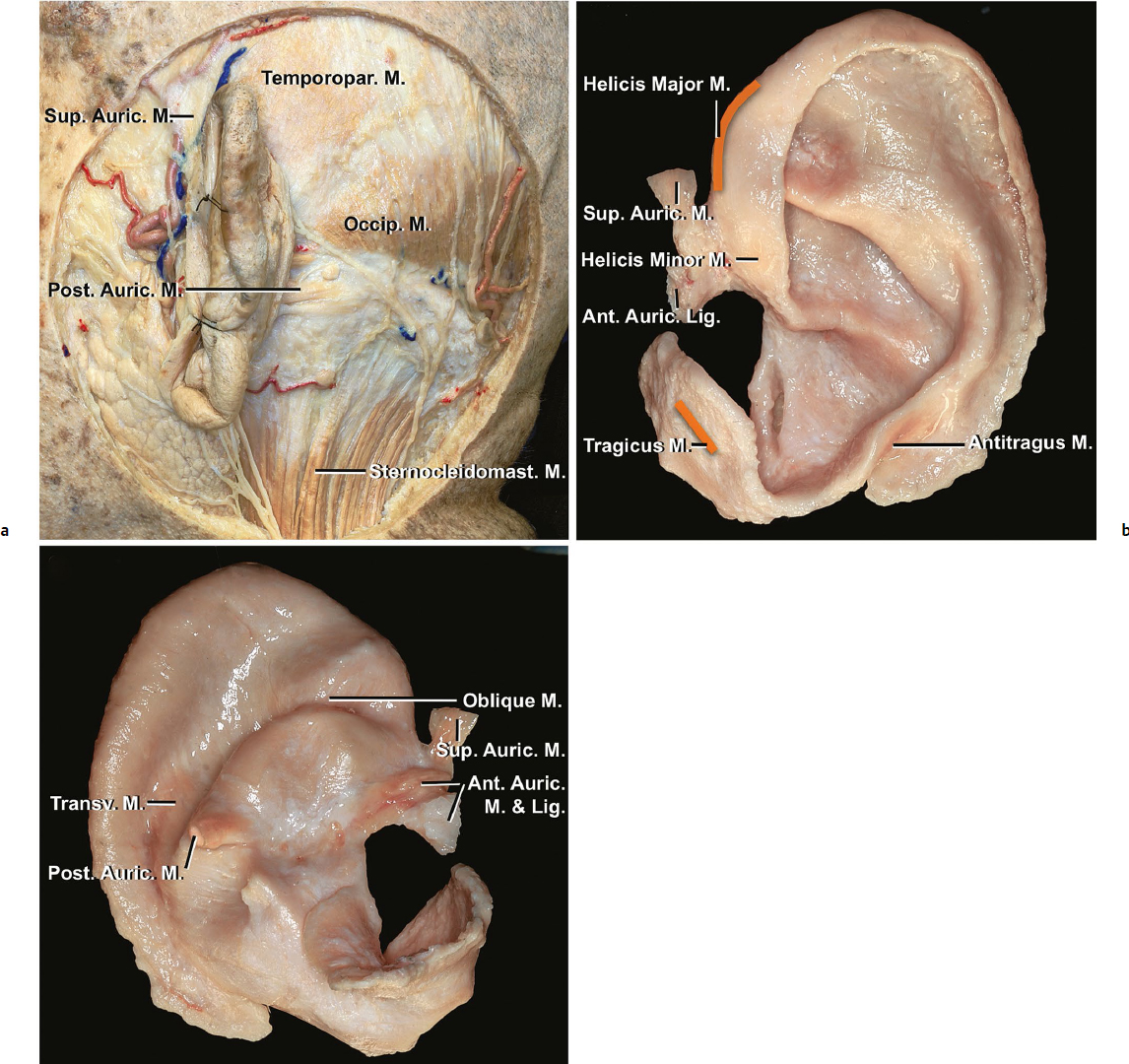
The muscles and ligaments that attach to the auricle are divided into two types: extrinsic and intrinsic (Fig. 18.5). The extrinsic muscles include the posterior, superior, and anterior auricular muscles. These muscles are small but hold the auricle firmly in place. The intrinsic muscles include the helicis major, helicis minor, tragicus, antitragicus, transverse auricular, oblique auricular, pyramidal auricular, and incisurae helicis muscles (Table 18.1). These intrinsic muscles contribute to creating the complex folded configuration of the cartilage. In humans, the auricular muscles are considered vestigial remnants and thus useless structures.
Theoretically, the superior, posterior, and anterior auricular muscles function to pull the auricle, upward, backward, and forward, respectively; however, these muscles are generally too weak to do so. In our dissection, we did not identify the helicis major, incisurae helicis, and pyramidal auricular muscles.
The superior auricular muscle arises from the galeal aponeurosis, which is continuous with the temporoparietal fascia, and inserts into the area around the spine of the helix. The posterior auricular muscle usually has two or three fascicles and is supported by the posterior auricular ligament. These muscles and ligament arise from the mastoid periosteum and are attached to the eminence of the cymbal concha and the ponticulus. The posterior auricular ligament supports this muscle and runs parallel to it. The anterior auricular muscle attaches to the zygomatic arch and temporoparietal fascia at the anterior end, and the spine of the helix at the posterior end. This muscle is supported by the anterior auricular ligament, which tethers the tragus and the spine of the helix to the zygomatic arch and temporoparietal fascia. In addition to these three extrinsic muscles, the temporoparietal muscles and part of the occipital muscle are also attached to the medial surface of the auricle by a fibrous ligament, which is part of the temporoparietal fascia.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


