Key points
- •
Early bacterial infection is typical.
- •
Late infection may be atypical – mycobacteria.
- •
Inflammation may be caused by foreign body reaction.
- •
Non-caseating granulomas may occur after blepharoplasty.
- •
Cutaneous sarcoidosis or chalazion may cause inflammation.
Introduction
Although wound infection rarely occurs following facial aesthetic surgery, there is a rare but not uncommon subset of atypical infections and granulomatous inflammation that has been reported following blepharoplasty. These lesions can be grouped into three categories which are based on post-operative timing that can be helpful with treatment protocols. The first group occurs less than 2 weeks following surgery and is composed of typical infections and hypersensitivity reactions. The second group usually occurs 2–6 weeks following surgery and is largely made up of delayed typical infections, pyogenic granuloma, suture granuloma, foreign body reaction, and suture abscess. The final group presents in a delayed fashion more than 6 weeks following blepharoplasty. This group consists of atypical infections that includes cutaneous mycobacteria, chalazion, cutaneous and subcutaneous non-caseating granulomas which may represent sarcoidosis and lipogranulomas.
While an infectious process is the most common etiology of atypical presentation, the surgeon should always consider skin cancer in the differential diagnosis of nodules occurring after a blepharoplasty. Since the diagnostic and treatment regimen for these typical and atypical processes are distinct from management of underlying infectious processes, appreciation of the entities is essential to optimal patient outcome. We review our shared experience in two busy clinical practices with the atypical lesions and highlight the diagnostic and treatment modalities which have been successfully implemented.
Background
Over 250,000 blepharoplasties were performed in the United States in 2008 making it one of the most common aesthetic surgical procedures performed. However, there is little literature addressing complications related to post-operative infectious and inflammatory lesions. Of particular concern are the subset of late presenting nodules related to atypical mycobacteria. In contrast to early post-operative infection or inflammation, which occurs along a post-operative time line of 4–7 days after surgery and most commonly consists of staphylococcal or streptococcal species, late post-surgical infections occur after more than 6 weeks in an atypical presentation.
It is important to recognize the distinction between typical and atypical infections since the treatment regimen is markedly different. Furthermore, inflammatory and granulomatous processes have a very distinct treatment algorithm usually consisting of steroids rather than antibiotics. The purpose of this chapter is to define an algorithm based on timing as well as management which should alert the surgeon to proper treatment and avoid treatment which may not improve the underlying pathology and in fact may make the process worse. Furthermore, the unique aspect of this chapter is that all of these patients presented after blepharoplasty, and to our knowledge atypical granulomatous processes have not been described following other facial surgical procedures.
Inflammation or infection?
When confronted with a post-operative blepharoplasty patient, the first step is to determine whether this is an infectious or inflammatory process. While the question might seem simple to answer, it is usually not straightforward. It should be assumed that all patients have an infection until proven otherwise. Delayed diagnosis or examination of a patient with infection might lead to peri-orbital cellulitis or rarely necrotizing fasiicitis. While typical infections are uncommon the diagnostic regimen includes empiric oral antibiotics for cellulitis as well as incision and drainage with culture and gram stain for localized abscess.
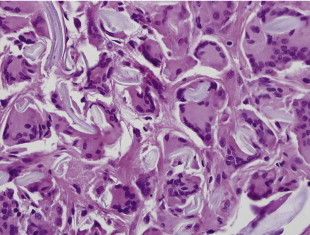
Atypical infections are much more difficult to diagnose and most commonly include mycobacterium fortuitum , mycobacterium chelonae , and mycobacterium abscessus . These atypical infections usually present after 6 weeks and require specific cultures. Any infection occurring more than 2 weeks following blepharoplasty is highly suspicious for an atypical mycobacterial infection ( Figure 15.1 ). During the interim period of 2–6 weeks after surgery, there are a number of inflammatory processes that include reaction to foreign body such as suture material, powder from gloves, ophthalmic ointment, as well as reaction to liquefied fat following blepharoplasty. This is a group of patients from whom it is more difficult to obtain a confirmatory diagnosis and specimens should be reviewed with polarized light to diagnose foreign body material. In addition, this group of patients is made up of individuals with granuloma reaction which appears as multiple subcutaneous nodules both in the upper and lower blepharoplasty incision distinct from the scar, but often involving the scar. There is less redness and drainage when compared to the infectious processes.

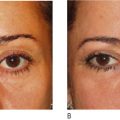
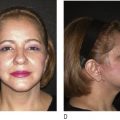
Granuloma after blepharoplasty is seriously debilitating to the patient and represents a complication which, although uncommon, requires extensive follow up and treatment including intralesional and oral steroids as well as conservative management since the process may take 6 months to improve ( Figures 15.2, 15.3 ). The cornerstone of treatment for this group of patients is steroids, which are clearly contraindicated in patients who may have an underlying infectious process. In addition, lesion disruption with an 18-gauge needle can be used to unroof the granuloma as well as complete excision once the process has entered the chronic phase where the subcutaneous nodules have matured into firm, smaller, mobile nodules compared to the initial presentation. Limited excision will minimize periorbital complications related to ectropion and lid malposition.


Lesions appearing less than 2 weeks after blepharoplasty
Infections which occur less than 2 weeks after blepharoplasty present with tenderness, warmth, erythema and underlying fluctuance. This is a typical presentation for a staph or strep infection and is most commonly confirmed by cultures. Patients may present with a febrile course with or without leukocytosis. All patients with a documented orbital cellulitis should have blood cultures if febrile. Quick determination of bacterial sensitivities is essential for optimal outcome. Periorbital Group A strep is a very serious infection that can rapidly spread and develop into orbital cellulitis or necrotizing fasciitis within a short period of time following initial presentation. A warm tender eye with proptosis may indicate post-septal extension of the cellulitis. Additionally, these patients may exhibit ptosis, diplopia, or ophthalmoplegia. This is a serious finding and a detailed physical exam, visual acuity examination and CT scan of the orbits should be performed immediately.
Any evidence of impairment of vision requires immediate surgical decompression. This should include a lateral canthotomy as well as opening of the septum. These maneuvers serve to decompress the orbital compartment thereby restoring blood flow to the optic nerve. Hospitalization, wide debridement, and intravenous antibiotics should be considered for this group of patients who have rapidly progressive orbital cellulitis and/or necrotizing fasciitis. ( Figure 15.4 ). Initial presentation of necrotizing fasciitis is indistinguishable from orbital cellulitis, and serial examination is mandated. Group A strep should be treated with ampicillin/tazobactam 4.5 g I.V. every 8 hours. While superficial pre-septal cellulitis is more common than orbital cellulitis, both can also be caused by streptococcus pyogenes as well as Staphylococcus aureus and Haemophilus influenzae type B. Management includes broad spectrum antibiotics with attention to rule out methicillin-resistant S. aureus (MRSA).

Antibiotic recommendations for orbital cellulitis includes ampicillin, sulbactam, cefuroxime, metronidazole or, if the patient has an allergy to penicillin, clindamycin and ciprofloxacin for 7–10 days. In patients where MRSA is suspected, intravenous vancomycin should be initiated prior to confirmation of the culture. Vancomycin is the treatment of choice for MRSA. In addition to antibiotic treatment, canthotomy and wide drainage for orbital cellulitis and necrotizing fasciitis may require surgical debridement of involved tissue as well as consideration for hyperbaric oxygen. The index of suspicion for orbital cellulitis and necrotizing fasciitis should be elevated in patients with insulin dependent diabetes mellitus or prior history of necrotizing fasciitis.
While inflammatory processes or hypersensitivity to suture can occur during the first 2 weeks, typical presentation is redness around the suture particularly when sutures have been left in place for more than 7 days. Epithelialized tracks can also occur as well as subcutaneous epidermoid cyst following blepharoplasty. These typically have very mild presentation and the epithelialized tracks can be simply unroofed with local anesthesia and an 18-gauge needle. Close follow-up of these patients is an essential diagnostic tool during the first 2 weeks. Typical bacterial infections generally respond to antibiotics and thereby can eliminate a branch from the differential diagnosis tree.
Lesions appearing 2–6 weeks after blepharoplasty
The majority of patients presenting 2–6 weeks after blepharoplasty with erythema and nodules in the peri-orbital region consist of delayed typical infections or reactions. One of the most common causes is an underlying suture abscess associated with dissolvable suture material. However, during this time period other potential processes may occur.
Pyogenic granulomas can occur during this period of time presenting as tender smooth pedunculated masses commonly associated with transconjunctival blepharoplasty. We have recommended that the conjunctiva should not be closed following transconjunctival blepharoplasty to avoid an increased risk of pyogenic granuloma formation. In addition, lateral canthoplasty sutures or transcanthal incisions can be associated with pyogenic granuloma in the lateral canthal region. These lesions can be simply excised under local anesthesia with cauterization of the base and removal of any exposed underlying suture. These lesions tend to be an isolated process without any other periorbital signs of inflammation and resolve following local excision. A specimen should be sent to pathology for final diagnosis.
Additional causes of localized inflammation in addition to suture granuloma include granuloma formation from foreign body ( Figure 15.5 ). Common causes include powder from surgical gloves, makeup including eye shadow and mascara, retained ophthalmic ointment, or liquefied fat following blepharoplasty. These are typically diagnosed at the time of biopsy with confirmation by appearance of foreign body on polarized light. Additionally, lipogranulomas can form which are different than non-caseating granulomas with respect to localized inflammatory processes around fat cells. Oil cyst can also occur either from liquefied fat or localized fibrosis and inflammation around ophthalmic ointment. Treatment includes conservative management and the majority of patients spontaneously resolve with time and treatment of underlying inflammation with low dose steroids including a Medrol Dose Pack.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


