Abstract
Atopic dermatitis is a common inflammatory skin condition that affects up to 20–30% of children and 2–10% of adults. It represents a complex genetic disease with environmental influences and an underlying defect in the epidermal barrier as well as associated immune dysregulation. Characteristic clinical features include onset during infancy or early childhood, intense pruritus, and a chronically relapsing course. Acute inflammation and involvement of the cheeks, scalp, and extensor aspects of the extremities predominates in infants, shifting to chronic inflammation with lichenification and a predilection for flexural sites in children and adults. Atopic dermatitis is often accompanied by other atopic disorders such as asthma, allergic rhinoconjunctivitis, and food allergies. This chapter reviews the pathogenesis, epidemiology, clinical manifestations, associated features, complications, and histopathologic findings of atopic dermatitis. A proactive approach to management is highlighted, including avoidance of trigger factors, regular use of emollients, and anti-inflammatory therapy to control subclinical inflammation as well as overt flares.
Keywords
atopic dermatitis, atopy, skin barrier, xerosis, lichenification, keratosis pilaris, Dennie–Morgan lines, pruritus, IgE, Th2, eosinophilia, food allergy, dupilumab, eczema herpeticum, filaggrin
- ▪
Common inflammatory skin condition that typically begins during infancy or early childhood and is often associated with other atopic disorders such as asthma, allergic rhinoconjunctivitis, food allergies, and eosinophilic esophagitis
- ▪
Complex genetic disease with environmental influences
- ▪
Characterized by intense pruritus and a chronic or chronically relapsing course
- ▪
Acute inflammation and involvement of the cheeks, scalp and extensor aspects of the extremities predominates in infants, shifting to chronic inflammation with lichenification and a predilection for flexural sites in children and adults
- ▪
Associated with a predisposition to skin infections, especially with Staphylococcus aureus and herpes simplex virus
- ▪
A proactive approach to management is recommended, including avoidance of trigger factors, regular use of emollients, and anti-inflammatory therapy to control subclinical inflammation as well as overt flares; targeted immunomodulatory therapy is available for more severe disease
Introduction
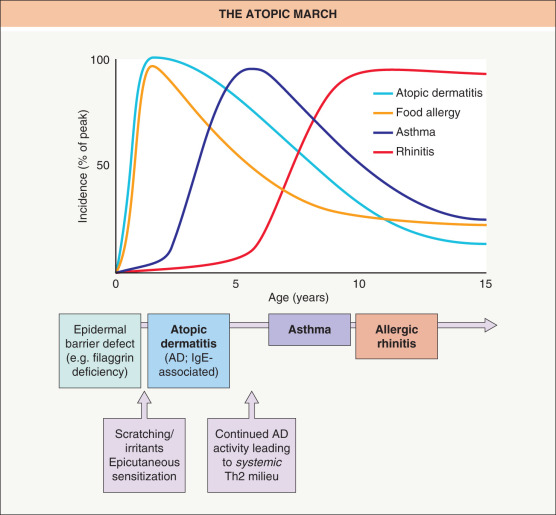
Atopic dermatitis (AD) is the most common chronic inflammatory skin disease, and its increasing prevalence presents a major public health problem worldwide . Characteristic features of AD include pruritus and a chronic or chronically relapsing course, usually beginning during infancy (early onset) but occasionally first developing in adulthood (late onset) . AD is a complex genetic disease and is often accompanied by other atopic disorders such as allergic rhinoconjunctivitis, asthma, food allergies, and less often eosinophilic esophagitis. These conditions may appear simultaneously or develop in succession. AD and food allergy have a predilection for infants and young children, while asthma favors older children and rhinoconjunctivitis predominates in adolescents. This characteristic age-dependent sequence is referred to as the “atopic march” ( Fig. 12.1 ). Given that atopic disease progression starts with AD, management should not be concentrated solely on the treatment of acute flares, but also be directed towards ameliorating the underlying genetically determined epidermal barrier dysfunction and preventing active dermatitis via maintenance therapy. Such an approach could potentially block the sensitizations and ongoing inflammation that drive the atopic march .
History and Definitions
The association of AD with allergic rhinitis and asthma was recognized by Besnier in 1892. The term “atopy” originates from the Greek word atopos meaning strange or unusual; it was first applied to this triad in the 1920s, including the use of “atopic eczema”. A decade later, Hill and Sulzberger proposed the name “atopic dermatitis”. The list of characteristic features proposed by Hanifin and Rajka in 1980 helped to unify the clinical concept of AD. In 1994, Williams and co-workers simplified Hanifin and Rajka’s criteria to establish the UK Working Party’s Diagnostic Criteria for AD, which were validated for the purpose of clinical studies; these criteria were modified slightly by Williams in 2005 . In 2003, a consensus conference spearheaded by the American Academy of Dermatology suggested revised Hanifin and Rajka criteria that are more streamlined and applicable to the full range of patient ages ( Table 12.1 ).
| DIAGNOSTIC FEATURES AND TRIGGERS OF ATOPIC DERMATITIS (AD) |
| Essential features: must be present and are sufficient for diagnosis |
|
| Important features: seen in most cases, supportive of diagnosis |
|
| Associated features: suggestive of the diagnosis, but less specific (see Figs 12.3 & 12.14 ) |
|
| Triggers |
|
* Stroking the skin leads to a white streak that reflects excessive vasoconstriction.
According to the consensus nomenclature by the World Allergy Organization (WAO) , the term “atopy” is tightly linked to the presence of allergen-specific IgE antibodies in the serum, as documented by positive fluorescence enzyme immunoassays (previously radioallergosorbent [RAST] tests) or skin prick tests. Thus, an IgE-associated or allergic form of dermatitis, formerly known as extrinsic AD , corresponds to AD in the strict sense. The remaining 20–30% of patients with the clinical phenotype of AD who have no evidence of IgE-sensitization are categorized as having a non-IgE-associated or non-allergic form of dermatitis, formerly known as intrinsic AD . However, IgE-associated/allergic “true” AD and non-IgE-associated/non-allergic dermatitis have substantial overlap and cannot be considered as two separate diseases; for example, the latter often represents an early transitional form of IgE-associated AD.
Epidemiology
The current prevalence of AD in most high-income and some low-income countries is approximately 10–30% in children and 2–10% in adults, representing a two- to threefold increase over the past several decades . In general, the prevalence of AD in rural areas and low-income countries is significantly lower than in their urban and high-income counterparts, illustrating the importance of lifestyle and environment in the pathogenesis of atopic disease.
Three subsets of AD based on age of onset have emerged from epidemiologic studies:
- •
early-onset type : defined as AD beginning in the first 2 years of life. This is the most common type of AD, which develops during the first 6 months of life in 45% of affected individuals, during the first year of life in 60%, and before 5 years of age in 85%. Approximately half of children with disease onset during the first 2 years of life develop allergen-specific IgE antibodies by 2 years of age. About 60% of infants and young children with AD go into remission by 12 years of age, but in others disease activity persists into adolescence and adulthood
- •
late-onset type : defined as AD that starts after puberty. There are few epidemiological studies on AD with onset in adulthood. Approximately 30% of AD patients overall are in the non-IgE-associated category, and among adults, the vast majority of such patients are women
- •
senile-onset type : an unusual subset of AD that begins after 60 years of age has been identified more recently .
Pathogenesis
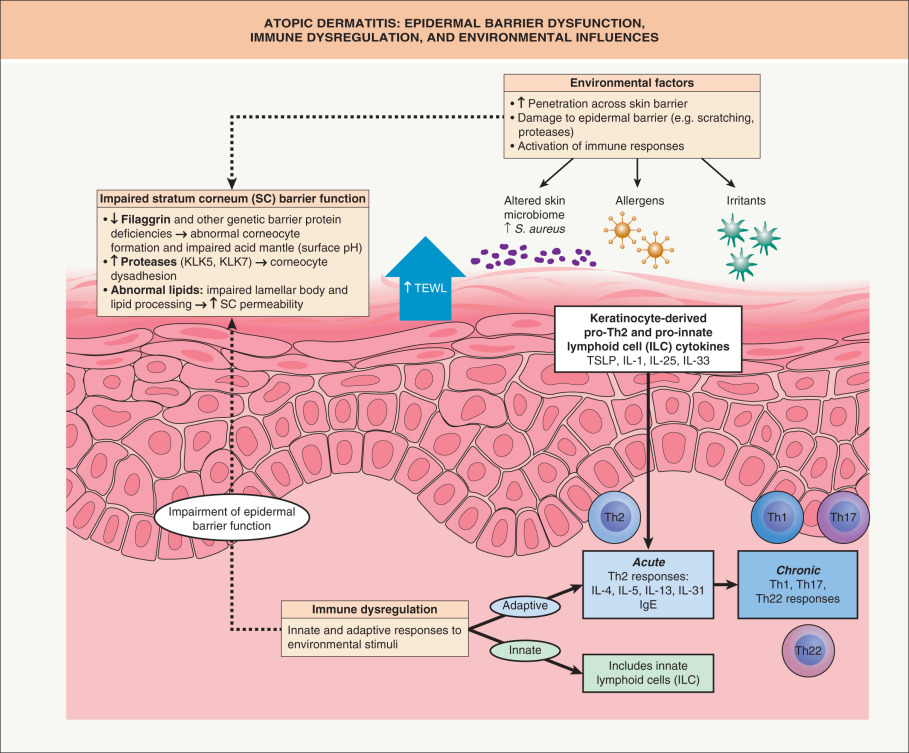
The pathogenesis of AD can be divided into three major categories: (1) epidermal barrier dysfunction ; (2) immune dysregulation ; and (3) alteration of the microbiome. Each of these can be modulated by genetic and environmental factors ( Fig. 12.2 ).
Genetic Factors
Genetic factors account for ~90% of susceptibility to early-onset AD , with a significantly higher concordance rate in monozygotic twins (77%) compared to dizygotic twins (15%) . Although the entities in the atopic triad cluster together in families, a parental history of AD is a stronger risk factor for the development of AD than either asthma or allergic rhinitis, supporting the existence of genes specific to AD susceptibility . Genes that encode proteins important to the epidermal barrier and immunologic functions have been implicated in AD pathogenesis ( Table 12.2 ). AD is a complex genetic disease, and both gene–gene and gene–environment interactions have important roles .
| SELECTED CANDIDATE GENES FOR ATOPIC DERMATITIS | |
|---|---|
| Candidate gene(s) | Defective protein(s) |
| Genes encoding epidermal proteins | |
| FLG | Filaggrin (loss-of-function variants; see text) |
| FLG2 | Filaggrin family member 2 |
| SPINK5 | Serine protease inhibitor LETKI |
| KLK5/SCTE, KLK7/SCCE | Kallikrein-related peptidases 5 & 7/stratum corneum tryptic & chymotryptic enzymes |
| CLDN1 | Claudin-1 |
| SPRR3 | Small proline-rich protein 3 |
| TMEM79 | Transmembrane protein 79 (mattrin) |
| Genes encoding immunologic proteins | |
| FCER1A | Fc fragment of high-affinity IgE receptor I, α chain |
| TLR2, 4, 6, 9 | Toll-like receptor-2, -4, -6, and -9 |
| IRF2 | Interferon regulatory factor 2 |
| IL4, 5, 12B, 13, 18, 31 | Interleukin-4, -5, -12B, -13, -18, and -31 |
| IL4RA, IL5RA, IL13RA | Interleukin-4, -5, and -13 receptors, α subunits |
| GM-CSF | Granulocyte–macrophage colony-stimulating factor |
| CD14 | Monocyte differentiation antigen CD14 |
| DEFB1 | β-defensin 1 |
| GSTP1 | Glutathione S-transferase P1 |
| CMA1 | Mast cell chymase |
| CCL5/RANTES | Chemokine (C-C motif) ligand 5/RANTES |
| TSLP | Thymic stromal lymphopoietin |
| MIF | Macrophage migration inhibitory factor |
| VDR | Vitamin D receptor |
| CYP27A1, CYP2R1 | Cytochrome p450 family members 27A1 and 2R1 |
Epidermal Barrier Dysfunction
A defective epidermal permeability barrier represents a consistent feature of AD and is evident in the nonlesional as well as lesional skin of affected individuals . A higher level of transepidermal water loss (TEWL), an indicator of barrier dysfunction, on day 2 of life predicts an increased risk of AD at 1 year of age . In addition, the level of TEWL in the nonlesional skin of children with AD correlates with disease severity . Epidermal barrier dysfunction permits an easier entry for irritants, allergens and microbes, which trigger immune responses that include the release of proinflammatory cytokines . In infants, greater TEWL is associated with an increased likelihood of epicutaneous sensitization to aeroallergens, which could potentially play a role in the development of asthma and allergic rhinoconjunctivitis . Factors that contribute to the impaired cutaneous barrier in AD are discussed below.
Filaggrin and other structural proteins
Filaggrin is a keratin fil ament- aggr egating prote in that serves as a major structural component of the stratum corneum. Loss-of-function FLG mutations represent the strongest known genetic risk factor for AD and are also responsible for ichthyosis vulgaris (see Ch. 57 ), with carrier frequencies of up to 10% in European and ~3% in East Asian populations . Approximately 20–50% of European and Asian children with moderate-to-severe AD have at least one FLG mutation; the penetrance of AD is ~40% for one and ~90% for two mutant alleles . This implicates epidermal barrier dysfunction in the initiation of AD, with subsequent development of Th2-biased immune responses . Of note, filaggrin expression is also affected by intragenic copy number variation and reduced by increased local pH, protease activity, and Th2 cytokine levels .
FLG mutations are associated with early-onset AD, greater disease severity, and persistence into adulthood as well as enhanced epicutaneous sensitization and an increased risk of irritant contact dermatitis, hand eczema, herpes simplex virus (HSV) infections, and food allergy . FLG mutations have also been linked to an increased risk for the development of asthma and greater asthma severity; however, these effects are only seen in patients with pre-existing AD . Since filaggrin is not found in the gastrointestinal or bronchial mucosa, the association of FLG mutations with food allergy and asthma strongly suggests that epicutaneous sensitization and/or cutaneous inflammation can contribute to the development of systemic atopic disease .
Filaggrin breakdown products such as histidine contribute to epidermal hydration, acid mantle formation, lipid processing, and barrier function . Gene expression profiling and immunohistochemical analysis of lesional and nonlesional skin from AD patients have shown broad defects in terminal differentiation, with down-regulation of other epidermal barrier proteins such as loricrin, corneodesmosin, involucrin, small prolene rich proteins 3/4 (SPRR3/4), claudin-1, and late cornified envelope protein 2B .
Stratum corneum lipids
The composition, organization, and biochemical processing of stratum corneum lipids are critical determinants of epidermal permeability barrier function (see Ch. 124 ). In AD, a filaggrin-deficient cytoskeletal scaffold contributes to abnormal loading and secretion of lamellar bodies, with subsequent defects in post-secretory lipid organization and processing . Disruption of the skin’s acidic mantle leads to reduced activity of lipid-processing enzymes such as β-glucoscerebrosidase and acid sphingomyelinase . Th2 cytokines also negatively affect generation of stratum corneum lipid components .
Proteases and protease inhibitors
Lesional AD skin demonstrates elevated levels of endogenous serine proteases, e.g. kallikrein 5 and 7 (KLK5/7), due to an imbalance in the activities of these proteolytic enzymes and protease inhibitors such as the lymphoepithelial Kazal-type trypsin inhibitor (LEKTI) encoded by SPINK5 . Biallelic loss-of-function SPINK5 mutations underlies Netherton syndrome, which features profoundly compromised barrier function and atopy (see Ch. 57 ), while SPINK5 polymorphisms have been linked to increased risk of AD in some populations . Other factors that enhance proteolysis include increased skin surface pH and exogenous proteases from allergens (e.g. house dust mites, pollens), Staphylococcus aureus , and Malassezia .
LEKTI deficiency results in excessive degradation of the corneodesmosomal component desmoglein-1 (Dsg1), causing abnormal stratum corneum detachment and thereby disrupting the epidermal barrier . The S. aureus extracellular V8 protease, which has a sequence similar to those of S. aureus exfoliative toxins, is also thought to degrade Dsg1 . In addition, unrestrained protease activity leads to degradation of lipid-processing enzymes and antimicrobial peptides as well as activation of proinflammatory cytokines .
Immune Dysregulation
The innate and adaptive immune systems play dynamic interrelated roles in the pathogenesis of AD. Acute AD lesions have a predominance of Th2 cytokines, but there is subsequent evolution to a chronic phase characterized by Th1 and Th22 cytokine profiles, as well as variable levels of Th17 cytokines in both acute and chronic AD . The acute phase features IL-4, IL-5, and IL-13; activation of eosinophils and mast cells; and production of allergen-specific IgE . Keratinocyte-derived cytokines including IL-1, thymic stromal lymphopoietin (TSLP), IL-25 (IL-17E), and IL-33 promote a Th2 immune response. Th2 cytokines inhibit expression of major terminal differentiation proteins such as loricrin, filaggrin, and involucrin as well as β-defensin-2/3 antimicrobial peptides .
Thymic stromal lymphopoietin (TSLP)
TSLP is an IL-7-like cytokine that is known as the “master-switch of allergic inflammation” due to its central role in evoking a Th2 response via dendritic cell activation . Exposure to allergens, viral infections, trauma, and other cytokines (e.g. IL-1β, TNF) can trigger TSLP production by keratinocytes, fibroblasts, and mast cells . TSLP is highly expressed in acute and chronic lesions of AD, but not in the nonlesional skin of patients with AD or in unaffected individuals .
IL-4 and IL-13
IL-4 has a key role in driving Th2 cell differentiation, IgE production, and eosinophil recruitment . Transgenic mice overexpressing IL-4 in their epidermis develop atopic dermatitis-like lesions, pruritus, an altered microbiome, and elevated IgE levels . The heterodimeric receptors for IL-4 and IL-13 both contain the IL-4 receptor α subunit (IL-4Rα; see Fig. 128.9C ) and activate signal transducer and activator of transcription 6 (STAT6), which promotes the differentiation of naive T cells into Th2 effector cells . Although IL-4 and IL-13 share 25% sequence homology and effector functions, studies in human subjects and human keratinocyte cell lines support an independent role for IL-13 in AD pathogenesis. Anti-IL-4/13 therapy with dupilumab, a monoclonal antibody that targets the IL-4Rα, is FDA-approved for the treatment of AD (see Ch. 128 and below).
Other cytokines
Th17 cells are important in the regulation of innate immunity, in particular neutrophil recruitment, and have also been implicated in allergic disorders . Th17 cells are found in acute as well as chronic AD lesions , and production of IL-17 and IL-19 is especially characteristic of new-onset pediatric AD .
IL-31 is a Th2 cytokine that is highly expressed in lesions of AD and other pruritic skin disorders such as prurigo nodularis . Cutaneous exposure to staphylococcal superantigen rapidly induces IL-31 expression in atopic individuals, establishing a link between staphylococcal colonization of the skin and pruritus. The heterodimeric receptor for IL-31 is expressed by keratinocytes, eosinophils, activated macrophages, cutaneous C nerve fibers, and dorsal root ganglia (see Ch. 5 ) . A randomized, placebo-controlled study showed that nemolizumab, a humanized monoclonal antibody against the IL-31 receptor A subunit, can significantly reduce pruritus in patients with moderate to severe AD .
IL-33, a member of the IL-1 cytokine family, protects against helminth infection by promoting a Th2-type immune response. IL-33 expression is increased in AD lesions compared to the skin of unaffected individuals .
Innate lymphoid cells
The innate lymphoid cell (ILC) family includes natural killer cells and three groups of non-cytotoxic ILCs that orchestrate immunity, inflammation, and homeostasis in multiple tissues . The group 2 ILC (ILC2) population is expanded in AD lesions and stimulated by TSLP, IL-25 (IL-17E), and IL-33 . ILC2s interact with other immune cells (e.g. mast cells, eosinophils) in the skin to promote Th2-type inflammation in a T-cell independent manner.
The Cutaneous Microbiome
The cutaneous microbiome represents a complex and highly diverse community of pathogenic and commensal bacteria, fungi, and viruses that play a critical role in epidermal homeostasis. More than 90% of patients with AD have skin colonized with S. aureus , compared to about 5% of unaffected individuals, presumably reflecting the disrupted acid mantle, decreased antimicrobial peptides (e.g. cathelicidins, defensins), and altered cytokine milieu of AD skin . During AD flares, bacterial diversity decreases and the proportion of the microbiome accounted for by Staphylococcus spp. increases from ~35% to ~90% .
Superantigens can promote the development of a Th2 immune response, and exotoxins with superantigenic properties are produced by up to 65% of the S. aureus strains that colonize AD patients . In addition, the S. aureus δ-toxin stimulates mast cell degranulation and Th2 inflammation . Filaggrin deficiency also increases the susceptibility of keratinocytes to S. aureus α-toxin-induced cytotoxicity .
Alterations in the skin microbiome of AD patients related to the use of cleansers and topical immunomodulatory or antimicrobial agents may have potential effects on cutaneous inflammation and barrier function. In addition, topical administration of coagulase negative Staphylococcus strains with antimicrobial activity has been shown to markedly reduce S. aureus colonization in AD patients , providing the basis for bacteriotherapy as a potential AD treatment.
Clinical Features
Disease Course
AD has a broad clinical spectrum that varies depending upon the age of the patient. It is divided into infantile, childhood, and adolescent/adult stages ( Fig. 12.3 ). In each stage, patients may develop acute, subacute, and chronic eczematous lesions, all of which are intensely pruritic and often excoriated. Acute lesions predominate in infantile AD and are characterized by edematous, erythematous papules and plaques that may exhibit vesiculation, oozing, and serous crusting. Subacute eczematous lesions display erythema, scaling, and variable crusting. Chronic lesions, which typify adolescent/adult AD, present as thickened plaques with lichenification as well as scale; prurigo nodule-like lesions can also develop (see below). Perifollicular accentuation and small, flat-topped papules (papular eczema) are particularly common in patients with African or Asian heritage. In any stage of AD, a generalized exfoliative erythroderma may develop in the most severely affected patients (see Ch. 10 ). All types of AD lesions can leave postinflammatory hyper-, hypo-, or occasionally depigmentation upon resolution ( Fig. 12.4 ).
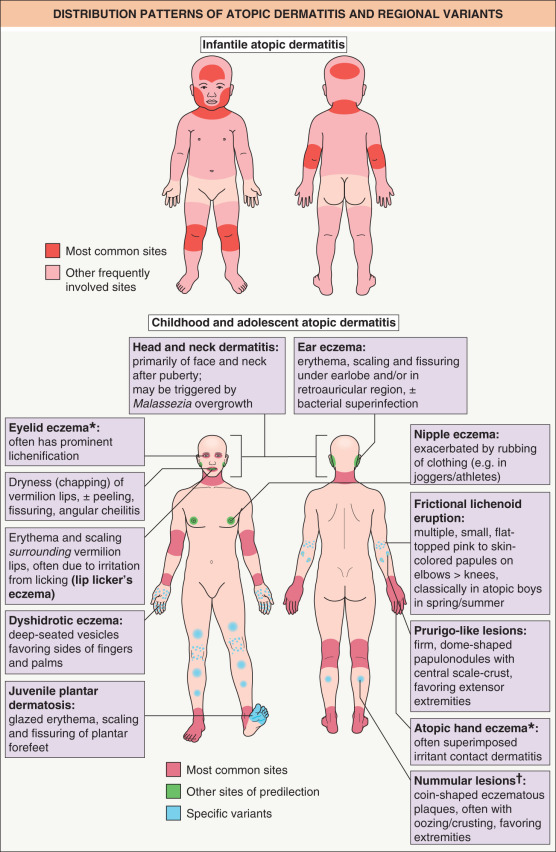

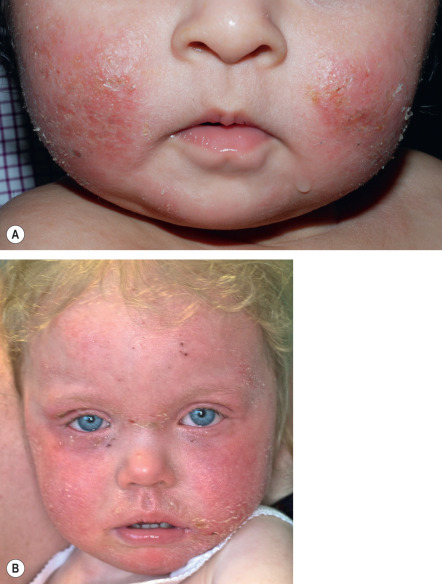
Infantile AD (age <2 years) typically develops after the second month of life, often initially appearing as edematous papules and papulovesicles on the cheeks, with sparing of the central face; the lesions may evolve to form large plaques with oozing and crusting ( Fig. 12.5 ). The scalp, neck, extensor aspects of the extremities, and trunk may also be involved, usually with sparing of the diaper area ( Fig. 12.6 ). In the first 6 months of life, the face is affected in >90% of patients with AD . Young infants may attempt to relieve itch through rubbing movements against their bedding, whereas older infants are better able to directly scratch affected areas.

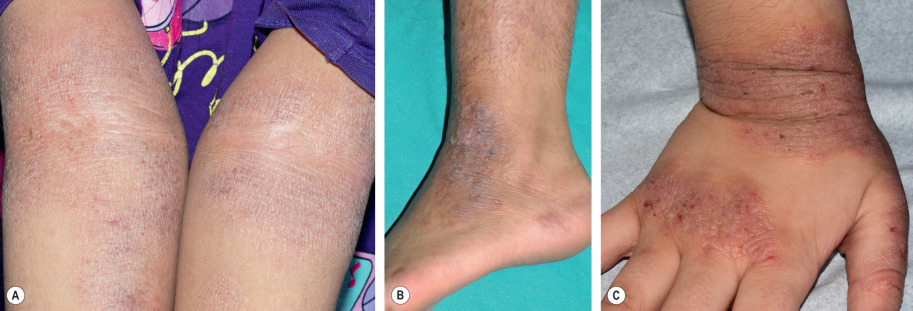
In childhood AD (age 2 to 12 years) , the lesions tend to be less exudative and often become lichenified. The classic sites of predilection are the antecubital and popliteal fossae (flexural eczema) ( Fig. 12.7 ). Other common locations include the wrists, hands, ankles, feet, neck, and eyelids, although any area can be involved ( Fig. 12.8 ). Xerosis typically becomes pronounced and widespread.


Adult/adolescent AD (age >12 years) also features subacute to chronic, lichenified lesions, and involvement of the flexural folds typically continues ( Fig. 12.9 ). However, the clinical picture may also change. Adults with AD frequently present with chronic hand dermatitis that has both endogenous and exogenous components ( Fig. 12.10 ), while others have primarily facial dermatitis ( Fig. 12.11 ), often with severe eyelid involvement (see below). Patients who have suffered from continuous AD since childhood are more likely to have extensive disease that is resistant to treatment. Such individuals may also have severe excoriations and chronic papular skin lesions because of habitual scratching and rubbing ( Fig. 12.12A ).



Senile AD (age >60 years) is characterized by marked xerosis. Most of these patients do not have the lichenified flexural lesions typical of AD in children and younger adults.
AD has a profound adverse impact on the quality of life of affected children and adults, with intense pruritus and stigmatization often resulting in sleep disturbances, psychological distress, social isolation, disrupted family dynamics, and impaired functioning at school or work. Children with AD experience greater impairment in their quality of life than those with diabetes mellitus or epilepsy .
Regional Variants of Atopic Dermatitis
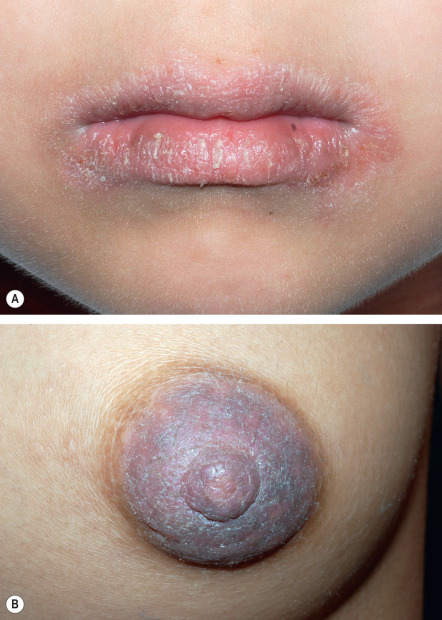
Several regional variants of AD can occur in isolation or together with the classic age-related patterns of involvement described above (see Fig. 12.3 ). The face is a frequent location for site-specific manifestations. Eczema of the lips, referred to as cheilitis sicca , is common in AD patients, especially during the winter ( Fig. 12.13A ). It is characterized by dryness (“chapping”) of the vermilion lips, sometimes with peeling and fissuring, and may be associated with angular cheilitis. Patients try to moisten their lips by licking, which in turn may irritate the skin around the mouth, resulting in so-called lip-licker’s eczema. Another common feature of childhood AD is ear eczema , presenting as erythema, scaling, and fissures under the earlobe and in the retroauricular area, sometimes in association with bacterial superinfection. Eyelid eczema can represent the only manifestation of AD, especially in adults. In contrast to eyelid eczema due to other causes, it is characterized by lichenification of the periorbital skin.
“Head and neck dermatitis” represents a variant of AD that typically occurs after puberty and primarily involves the face, scalp, and neck. When older children and teenagers present with this form of AD, it usually persists into adulthood. Malassezia yeasts, which are members of the skin microbiome in the head and neck area, may be an aggravating factor for this presentation , and systemic antifungal treatment with itraconazole or fluconazole may be of benefit.
Eczema variants also occur in acral sites. Juvenile plantar dermatosis presents with “glazed” erythema, scale, and fissuring on the balls of the feet and plantar aspect of the toes in children with AD (see Ch. 13 ). Atopic hand eczema (see Fig. 12.10 ) affects ~60% of adults with AD and may be the only manifestation of the condition. FLG mutations are associated with increased likelihood of hand eczema in children and adults , and frequent exposure to water and other irritants in household or occupational settings represents another risk factor. Atopic hand eczema typically involves the volar wrists and dorsum of the hands. The palms and sides of the fingers may develop the deep-seated vesicles of dyshidrotic eczema (see Ch. 13 ).
The prurigo form of AD favors the extensor aspects of the extremities and is characterized by firm, dome-shaped papules and nodules with central scale-crust, similar to prurigo nodularis lesions in non-atopic patients ( Fig. 12.12B ). Nummular (discoid) lesions also tend to develop on the extremities in children and adults with AD, appearing as coin-shaped eczematous plaques, usually 1 to 3 cm in diameter and often with prominent oozing and crusting ( Fig. 12.12C ). They are similar in appearance to nummular dermatitis occurring outside the setting of atopy (see Ch. 13 ). Frictional lichenoid eruption has a predilection for atopic children and presents as multiple small, flat-topped, pink to skin-colored papules on the elbows and (less often) knees and dorsal hands. Lastly, chronic nipple eczema can develop in children and adults with AD ( Fig. 12.13B ).
Associated Features
Pruritus
Intense pruritus is a hallmark of AD. The itch is often worse in the evening and may be exacerbated by exogenous factors such as sweating or wool clothing. Rubbing and scratching in response to pruritus can initiate flares or exacerbate existing dermatitis, explaining why AD is known as the “itch that rashes”. Excoriations (linear or punctate) are frequently present, providing evidence of scratching ( Fig. 12.14 ; see Figs 12.7–12.9 ). With repeated rubbing and scratching, the skin becomes thickened and leathery with exaggerated skin markings, referred to as lichenification (see Figs 12.9 and 12.10 ).
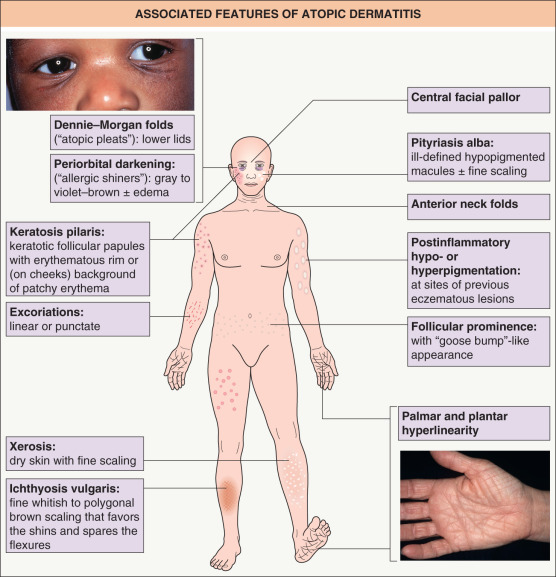
Atopic stigmata
Physical findings other than dermatitis that are frequently observed in patients with AD are presented in Table 12.3 and Figs 12.15–12.17 .
| ASSOCIATED FEATURES OF ATOPIC DERMATITIS (“ATOPIC STIGMATA”) | |
| Xerosis |
|
| Ichthyosis vulgaris |
|
| Keratosis pilaris |
|
| Palmar and plantar hyperlinearity |
|
| Dennie–Morgan lines |
|
| Periorbital darkening (“allergic shiners”) |
|
| Anterior neck folds |
|
| Hertoghe sign |
|
| White dermographism |
|
| Follicular prominence |
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


