10 Asian facial cosmetic surgery
Synopsis




Introduction
The face, while only a single part of the body, is the icon of self-identity and can be easily recognized among hundreds of thousands of faces. Asian and Caucasian faces each have unique features. It is generally accepted that Asians have small, puffy eyes with an epicanthal fold, shallow orbits, a low profile nasal dorsum with thick skin, flat faces with large cheekbones and broad width. This is especially true for East Asians, including people from China, Japan, Mongolia, North Korea, South Korea and Taiwan.1 Asia is the largest continent, and has numerous ethnic groups.1,2 Southern Asians have darker, thicker skin, larger eyes with double folds and smaller, narrower facial skeletons compared to northern Asians, whereas western Asians have quite different facial features from other Asians. Although there are some constants, the standard of beauty varies among countries. Anatomic characteristics and cultural differences, including trends in each ethnic group, should be considered before performing facial cosmetic surgery.
Much controversy surrounds the concept of universal beauty. Humans, even babies, have an innate affinity for beautiful people.3 Symmetry and a healthy, young-looking appearance make a face more attractive, regardless of ethnic background. A key feature of beautiful faces is the quality known as youthfulness.4 In Caucasian women, high cheekbones are an important factor, whereas Asian women with round or oval-shaped faces are considered more beautiful. When Asians see facial photographs of themselves alongside Caucasians, they, especially younger individuals, are sometimes disappointed with their appearances. In general, Asian faces tend to look broader with a flatter contour to their eyes, nose, and face. We live in a three-dimensional world, and the faces we observe directly are three-dimensional. Facial cosmetic surgery is a three-dimensional procedure, and more emphasis is being placed on facial contour changes.
Young female Asians have become acutely interested in their appearance, creating a boom in cosmetic surgery. This phenomenon has created a new standard of beauty. Females in East Asia seek larger eyes, a higher nose, and a smaller face, which are not traditional to “Asian” beauty but have been influenced by Western countries. It is incorrect to simply assume that Asians seek to “westernize” their faces. Although westernization of the Asian face seemed to be a goal in the past, most patients now want to preserve their ethnic identity, while at the same time improving their appearance.1,2,5 This has reached a point where people wonder if the concept of traditional beauty no longer exists in these Asian countries and traditional beauty is no longer deemed beautiful. Some patients in cosmetic surgery clinics want to look like celebrities in their respective countries. These celebrities have beautiful and attractive faces that are popular not only in their own countries but in neighboring countries. Patients seeking cosmetic surgery must be properly counseled in order to avoid disappointment from unrealistic expectations.
Some Asians have attractive facial traits, including large eyes, a well-balanced nose with a good profile, and small lower faces.6 Individuals who regard their facial features as falling short of the mainstream ideals of beauty are willing to undergo facial cosmetic surgery. Younger individuals, for example, wish to undergo facial bone contouring to make their faces smaller. These individuals do not have “below average faces”.1 Rather, they want to look above average, sometimes chic and stylish, not merely natural. Most patients who want facial cosmetic procedures like double eyelids and augmentation rhinoplasty are women, but these cosmetic procedures are also requested by men.
Asian blepharoplasty
Introduction
Few young Caucasians undergo cosmetic procedures for their upper eyelids. Most of these individuals have large eyes with crisp, tall upper lid creases. In contrast, Asians are described by westerners as having puffy, small eyes, epicanthal folds, and lack of supratarsal folds. However, this is not true of all Asians. About 50% of women in East Asia have these features.1,2 Many Asian women wish to enhance their appearance but they do not want Caucasian eyelids.1,2,7 Asian blepharoplasty or “double eyelid” surgery is the most common cosmetic operation in Asia, with some reports suggesting that 30–60% of Asians undergo this procedure.8 If these women have deep-set, large eyelids with high folds like Caucasians, they look unnatural, as such eyelids do not match the shape of their faces. Therefore, ethnic differences should be considered.
The first procedure to create a supratarsal fold or “double eyelid” was described by Mikamo in 1896.9 The procedure was performed on a patient who lacked a fold in one of her upper eyelids. Shirakabe et al. made a historical review of 32 surgical techniques reported in Japan.10 In the western countries, Sayoc reported anatomic differences of upper eyelids between Caucasians and East Asians. The anatomic differences and their implications regarding double eyelid surgery were discussed.11 Fernadez and Flowers in Hawaii, where East meets West, published papers about double eyelid surgery for Asians.4,12 Newer techniques seeking to be more refined and less invasive while imitating the natural fold are being reported.13
Anatomic considerations
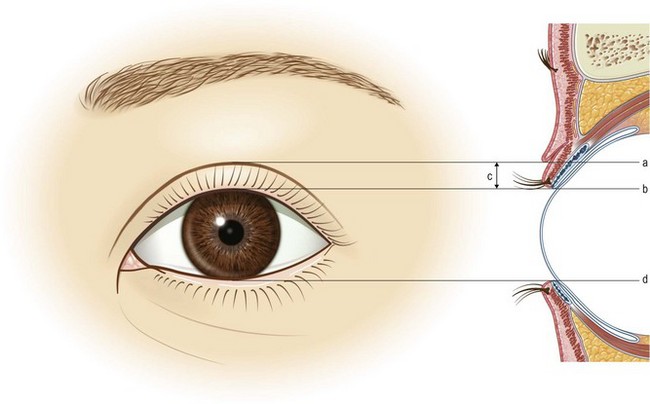
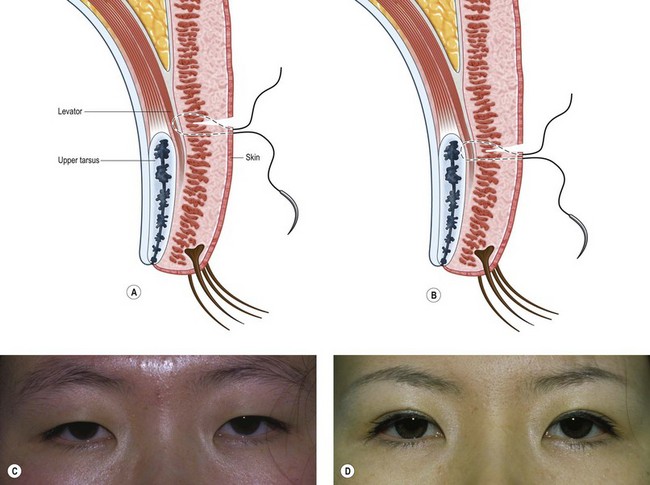
Multiple theories exist regarding the formation of the supratarsal crease or fold (Fig. 10.1). First, Sayoc explained the presence of double fold based on anatomic differences between Caucasian and East Asian eyelids. Expansions of the levator palpebrae superioris muscle penetrating through the septum and orbicularis oculi muscle to the overlying dermis were thought to be present in Caucasian eyelids and less so in Asians (Fig. 10.2A).14 The presence of such attachments between the levator aponeurosis and skin was established by Cheng and Xu through scanning electron microscopy studies.15 Another concept is the role of fibrous septa between the tarsal plate and pretarsal skin. The adherence between the tarsal plate and pretarsal skin is loose in the single eyelid and tight in the double eyelid.4,16 Therefore, both explanations focus on the connection between the levator mechanism and the pretarsal skin.
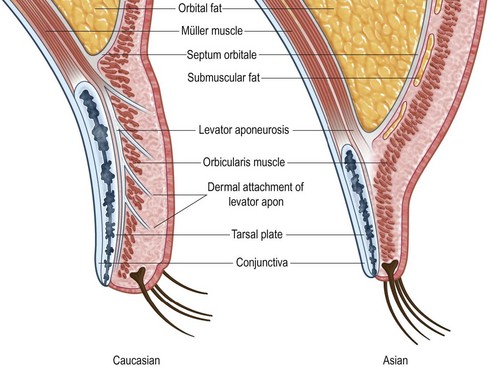
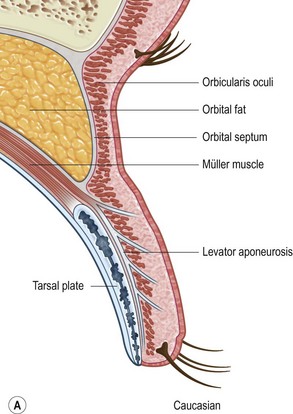
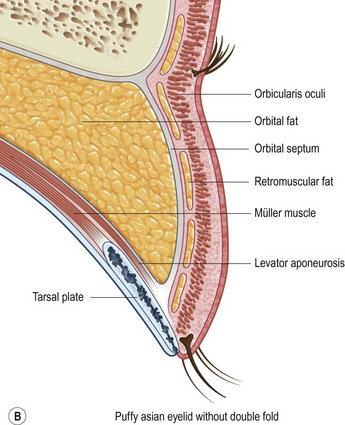
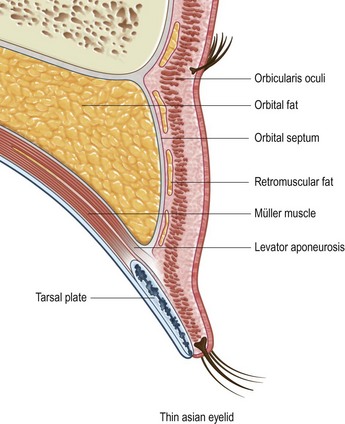
An important factor contributing to supratarsal crease formation is the level of fusion of the orbital septum and the levator aponeurosis. The supratarsal crease is formed by the dermal insertion at the confluence of the septum and levator aponeurosis.13 The level of adhesion between the orbital septum and levator aponeurosis defines the superior palpebral crease in most Caucasian eyelids,17 whereas lower fusion of the orbital septum to levator aponeurosis results in a low lying or absent crease in the Asian eyelid (Fig. 10.2B). Asians with naturally occurring superior palpebral folds have a relatively higher fusion of the orbital septum and levator aponeurosis (Fig. 10.3).18 The preaponeurotic orbital fat present in the pretarsal space eliminates the formation of double fold in Asians. Among Asians, it is not unusual for the upper lids to vary, being double and single in the same individual, depending on such variables as fatigue, diurnal variations of eyelid swelling, and weight change.
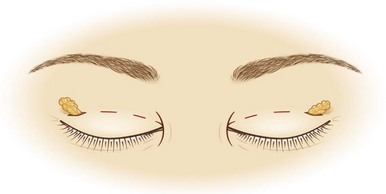
The epicanthal fold is also a characteristic feature of Asian upper lid. It hides the medial part of eye, including the caruncle and lacrimal lake and increases the intercanthal distance. In East Asians, at least 50% of adults have epicanthal fold. If slight traces are included, almost all East Asians retain epicanthal folds, and a mild epicanthus is not an unusual feature for them.1 There has been a recent trend to eliminate or loosen the epicanthal fold as part of the double eyelid operation. This medial epicanthoplasty will decrease the wide intercanthal distance and increase the horizontal width of the palpebral apertures. However, surgeons should be very cautious about total elimination of epicanthal folds, because this can leave a noticeable scar and result in loss of ethnic identity.
Preoperative considerations and diagnosis
Most Asian patients desiring double eyelids no longer want a westernized appearance, but rather an appearance more appropriate for Asians. Because the anatomy of the orbit differs greatly between Asians and Caucasians, Asian blepharoplasty should be performed in accordance with the orbital anatomy of Asians. Previously, most young Asians seeking upper blepharoplasty have done so only for double fold formation. More recently, Asians have undergone upper blepharoplasty to achieve a more attractive eyelid shape by reducing the puffiness in their eyelids, obtaining a double fold, and increasing the palpebral fissure length.18 These patients also prefer a flat upper eyelid which looks young and stylish, not sunken or deflated.4
The height of double eyelid is an important issue. In young Caucasians, the superior palpebral fold is small and the height of the pretarsal skin exposure is similar to te height of the superior palpebral crease.18 In contrast, the Asian lid crease is generally 2–3 mm lower, and a large superior palpebral fold hangs over the pretarsal skin.7 Thus, exposure of pretarsal skin is less than in Caucasians. The lower border of the fold is called the double eyelid line, and the distance between this line and the margin of the lid at primary gaze is pretarsal exposure (Fig. 10.4). After blepharoplasty, the pretarsal exposure is determined by several factors, such as the height of incision, the amount of pretarsal skin excision, the height of fixation, and levator function.18 Currently, the preference for most Asians is a pretarsal exposure <3 mm, and as little as 1 mm.7 These desires have geographical variation (Fig. 10.4).
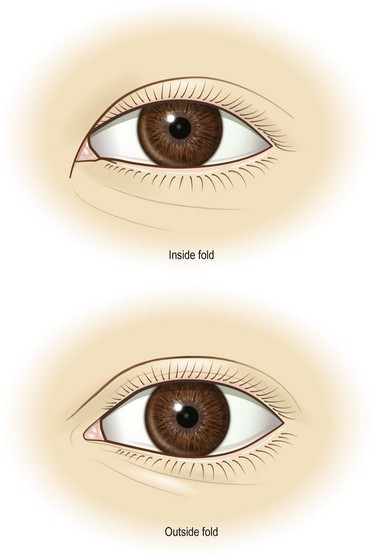
Another preoperative consideration is the shape of the desired crease. Caucasians typically have a semilunar shaped crease where the central third of the crease lies farther from the lash line than the medial and lateral thirds.19 Most Asians are uncomfortable with this configuration, since it appears unnatural to them. They prefer a fold that for most part is parallel to the lid margin. Laterally, the crease may have a slight flare, in that the crease lies farther from the lash line than the central third. Medially, the crease may taper toward the medial canthus (“inside fold”) or run outside the epicanthus (“outside fold”) (Fig. 10.5).20
Treatment/surgical technique
Incisional versus nonincisional methods
Nonincisional methods
Numerous nonincisional methods have been described.21–26 These methods are used primarily for young people who do not require skin excision and for patients with thin upper eyelid tissue who do not have an excess of fat. The advantages of these minimally invasive techniques must be balanced against the knowledge that the fixation may not be as durable over time when compared with the incisional methods. Non-incisional methods can be categorized as single stitch and multiple stitch methods, both of which have advantages and disadvantages.
 Video 1
Video 1 Video 2
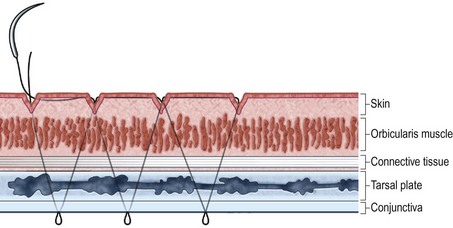
Video 2• Single stitch nonincisional methods have many modifications.21 Figure 10.6 shows a nonincisional single stitch method. Fixation through the levator aponeurosis can result in a more natural appearance and minimal postoperative edema, but relapse can sometimes occur. Fixation through the upper portion of the tarsal plate can result in a more definite eyelid crease with minimal relapse, but postoperative edema can occur more frequently than in levator fixation methods.
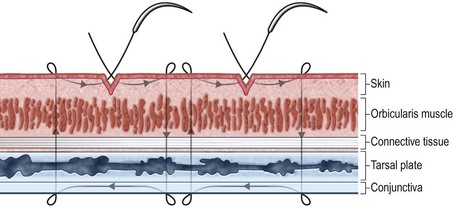
• Multiple stitch nonincisional methods can be performed, usually with 3–5 stitches on each side (Fig. 10.7).27
Partial incisional methods
Partial incisional methods (Fig. 10.8) are being used more frequently.28,29 These procedures have evolved to overcome disadvantages of the above two methods. Partial incisional methods can result in moderate tissue adhesions, preventing the early relapse observed using nonincisional methods. Moreover, partial incision can result in a more natural appearance, minimizing scarring of the upper lid. Using the partial incisional approach, preaponeurotic fat can be easily removed to correct puffy eyelids.
Incisional methods
For double fold formation in the upper lid, traditional tarsodermal fixation through incisional methods (Fig. 10.9A,B) has been an effective standard method.30 In patients with redundant eyelid skin, the incisional approach is unavoidable. There are as yet no definite standards for incisional blepharoplasty, but the common procedures will be described. The placement of the double fold on the upper lid should be decided preoperatively according to each patient’s appearance and preference utilizing forceps or a probe.
The skin incision marking tapers closer to the lash line as it progresses medially towards the epicanthal fold. Some patients may prefer that the medial portion of the crease lies outside the epicanthus. The superior incision is marked such that the skin to be excised will also taper, usually measuring 1 mm medially, 2 mm centrally, and 3 mm laterally. The skin incision is then made and the strip of skin excised. A strip of orbicularis oculi wider than the skin strip is then removed in order to create a sharp lid crease. Leaving excess orbicularis can result in a puffy appearance. The septum is then entered, and a variable amount of retroseptal fat may be either excised or released, allowing it to ride up superiorly. The levator aponeurosis is exposed as it approaches the tarsal plate. The Asian tarsal plate typically measures 6–7 mm in height. Fixation of the new upper lid crease is then done. Various methods of suture fixation involving internal buried sutures have been described. One method is to use 3–7 sutures passing through the aponeurosis and the dermis-muscle of the inferior skin edge. The skin is thus anchored to the levator mechanism, creating the new lid crease, which will be hidden by the overhanging tissue of the palpebral fold. Alternatively, fixation can be done to the superior edge of the tarsal plate, a procedure which is thought to create a more static and defined upper lid crease (Fig. 10.9B–D).
Subclinical ptosis repair
Many Asian people who want more attractive looking eyelids are not satisfied with the creation of a simple double crease.31 They may have a low resting level of their eyelids, which if corrected will give them a more open and attractive palpebral fissure.32 These patients have a tendency for upper eyelid ptosis, and are defined as having “subclinical ptosis”. They may be candidates for the same procedures utilized in cases of mild ptosis, including Müllerectomy, or levator aponeurosis plication or advancement.33–35
Medial epicanthoplasty
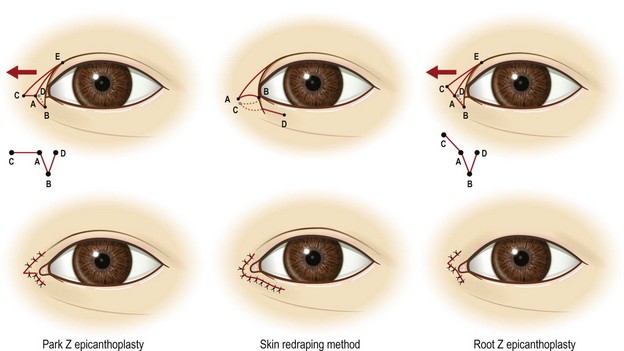
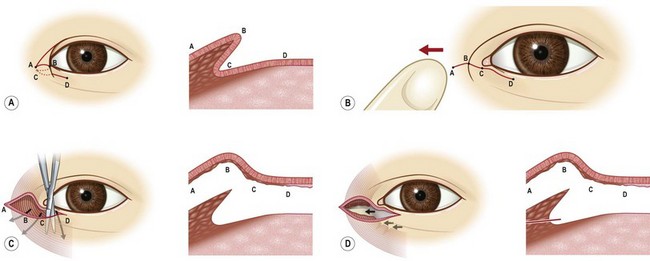
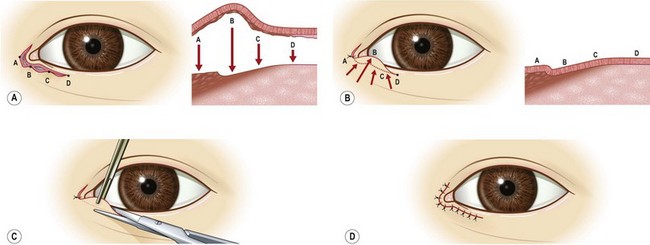
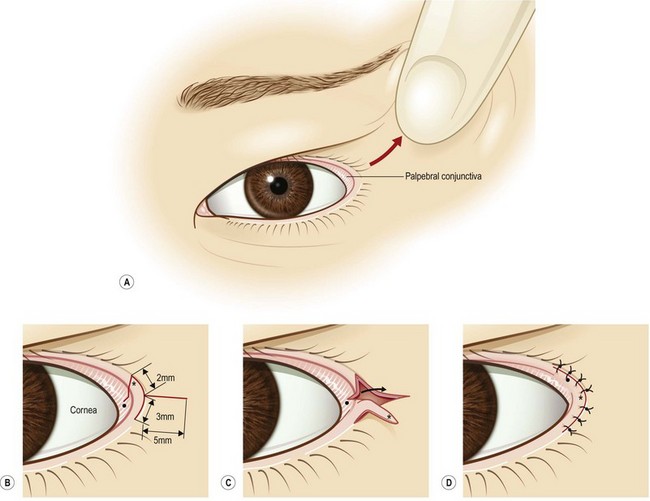
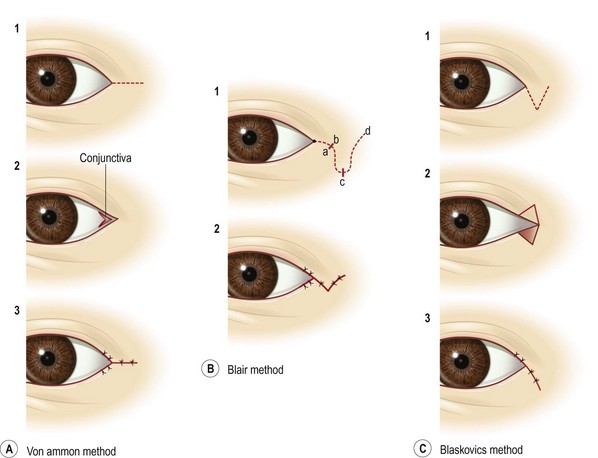
Medial epicanthoplasty (Figs 10.10–10.12) is a very important component of Asian eyelid surgery.36 Various methods were originally introduced for the correction of blepharophimosis in Western countries. In Asia, however, these procedures have been used for the correction of average Asian medial epicanthal folds. Although traditional methods, including the Mustarde technique,37,38 have been used, these procedures may result in bad scars on the medial canthal area. These problems may be overcome by the half Z-plasty technique.37,39,40 Nevertheless, the amount of release is limited and a moderate scar remains. Many Asian patients have complained about these scars. New methods, including skin redraping methods, have therefore been developed to eliminate the possibility of scarring of the medial canthal area.36,41 These skin redraping methods, which have become very popular in Asia, include a medial subciliary incision on the lower eyelid which makes a nonvisible scar and resection/releaser of medial epicanthal adhesions, procedures that can minimize medial epicanthal scars and correct medial epicanthus quite well (Figs 10.11 and 10.12).
Asian rhinoplasty
Introduction
Augmentation rhinoplasty is one of the most common aesthetic plastic surgery procedures in Asian countries. Whereas most Western literature addresses issues related to rhinoplasty in Caucasians, such as reduction and corrective rhinoplasty procedures, augmentation of the nasal dorsum and tip remain key issues for Asian plastic surgeons.43 In the past, most of these operations consisted of simple augmentation rhinoplasty. More recently, however, the needs of patients have become more complex, requiring more meticulous preoperative diagnosis and more involved surgical techniques. Ideally, rhinoplasty should enhance the harmony between the nose and face, thus requiring general evaluation of the entire face. For this purpose, the entire face must be evaluated. The general principles for rhinoplasty in Asians are quite similar to those in Caucasians. However, rhinoplasties in Asians and Caucasians have different characteristics. This section will describe various aspects of rhinoplasty in Asians, as well as commonly encountered problems and solutions.
Differences in nasal soft tissue and skeletons between Asian and Caucasian noses
The nasal profile of Asians is quite different from that of Caucasians. The Asian nose has a shorter height, less tip projection, and a wider nasal base when compared to the Caucasian nose. The Asian nose has a similar height and narrower width than the African nose.44 The overlying soft tissue enveloping Asian noses consists of a dense fibromuscular layer along with a fatty layer, especially over the alar lobule. The linear dimensions of the nose are smaller in Asians than in Caucasians, but their noses are wider, although their nostril floor widths are quite similar. These findings can be attributed to the thicker, flaring alar lobule in Asians.45 A comparison of the aesthetic proportions of Asian and Caucasian noses found that Asian noses projected less from the face and were broader at the intercanthal level and alar base, but not at the bony base. Moreover, Asian noses projected less at all levels, including the nasion projection and tip projection.46
Although there are racial variations among Asians, nasal skeletons are generally smaller and weaker in Asians than in Caucasians.47 The shape of the nasal bone in Germans has been classified into eight types, whereas the width of the nasal bones was shorter and the width of the pyriform aperture was wider in Asians than in Germans. The nasal base width in Asians is greater than in Caucasians but less than in Africans. Asian noses have been found to be wider at the nasal base, but similar or shorter in the height of the nasal base (tip projection), than in Caucasians.48 Contrary to popular thought, the alar cartilage in Asians is not markedly smaller than in Caucasians, although there are differences in the configuration and thickness of the cartilage and the length of the foot plate of the medial crus. Moreover, nostril shape was found to be affected mainly by the volume of the dilator naris anterior/posterior muscular components, the depressor septi nasi muscle, the shape of the lateral crus and the footplate segment ratio.49 In Asians, there is also a loose connection between the domes of the middle crura and the absence of attachment of the medial crura to the caudal septum. This might explain, at least in part, why the nasal tip is broad, and underprojected, while its base is wide. Moreover, the lateral crus is usually concave in Asians, but convex in Caucasians.50 Findings such as these have led to significant advancements in Asian rhinoplasty.
History
Rhinoplasty in Asians was first reported in 1964 by Khoo Boo-Chai.51 He demonstrated augmentation rhinoplasty in Asians using autogenous materials and silicone implants. He proposed the “golden point”, midway between the orbital ridge and the intercanthal line, which is the optimal starting point for the end of a silicone implant on the nasal dorsum. He also proposed the importance of both dorsal and nasal tip augmentation in Asian rhinoplasty. In 1974, Furukawa summarized the important aspects of Asian rhinoplasty.16 He reported anthropometric data of Japanese, identified the ideal Asian profile and described unique techniques for the Asian nose. Moreover, diverse-shaped silicone dorsal implants were introduced. In 1986, McCurdy showed the aesthetic goals of rhinoplasty in the non-Caucasian nose are similar to those in the Caucasian nose.52 He also noted that technical modifications are needed when performing a non-Caucasian rhinoplasty. In 1990, Parsa’s report showed nasal augmentation with split calvarial grafts in Orientals.53 Shin and Lee reported, in 1993, columella lengthening in nasal tip plasty of Orientals.54






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


