The periarticular sources of pain around the hip joint include, but are not limited to, disorders of
Peritrochanteric space (trochanteric bursitis, external coxa saltans, and abductor tears)
Iliopsoas musculotendinous unit (internal coxa saltans)
Rectus abdominis/pubic symphysis/adductor tendon (athletic pubalgia)
Proximal hamstring tendon (avulsion fractures and tendon tears)
Sciatic, ilioinguinal, obturator, and lateral femoral cutaneous nerves (LFCNs) (compression syndromes)
 Periarticular endoscopic procedures are capable of addressing pathology in all the aforementioned regions.
Periarticular endoscopic procedures are capable of addressing pathology in all the aforementioned regions.
 The snapping/lateral hip (external and internal coxa saltans and trochanteric bursitis), athletic pubalgia, and proximal hamstring injuries have been covered in other sections of this book. This chapter will highlight the use of periarticular endoscopic techniques around the hip by providing a detailed overview of the repair of abductor tears.
The snapping/lateral hip (external and internal coxa saltans and trochanteric bursitis), athletic pubalgia, and proximal hamstring injuries have been covered in other sections of this book. This chapter will highlight the use of periarticular endoscopic techniques around the hip by providing a detailed overview of the repair of abductor tears.
ANATOMY
 The peritrochanteric space is located between the greater trochanter and iliotibial band. The boundaries of this space are formed by tensor fascia lata muscle anteriorly, the insertion of the gluteus maximus tendon to the femur just below the vastus lateralis inferiorly, and the gluteus medius and minimus tendons superiorly.
The peritrochanteric space is located between the greater trochanter and iliotibial band. The boundaries of this space are formed by tensor fascia lata muscle anteriorly, the insertion of the gluteus maximus tendon to the femur just below the vastus lateralis inferiorly, and the gluteus medius and minimus tendons superiorly.
 The greater trochanter of the hip, much like the greater tuberosity of the humerus, has an osseous contour that reflects the attachments of the gluteal muscles.
The greater trochanter of the hip, much like the greater tuberosity of the humerus, has an osseous contour that reflects the attachments of the gluteal muscles.
 Four facets on the greater trochanter have been described7: anterior, lateral, superoposterior, and posterior facets (FIG 1).
Four facets on the greater trochanter have been described7: anterior, lateral, superoposterior, and posterior facets (FIG 1).
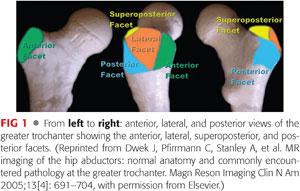
 The gluteus medius is a large, fan-shaped muscle consisting of three equal-sized segments—the anterior, middle, and posterior—that originates from the external surface of the ilium. Each segment is innervated by a separate branch of the superior gluteal nerve. Its tendon attaches at two distinct facets on the greater trochanter. The anterior and most of the central fibers are attached to the lateral facet, and the posterior fibers are attached to the superoposterior facet16 (FIG 2).
The gluteus medius is a large, fan-shaped muscle consisting of three equal-sized segments—the anterior, middle, and posterior—that originates from the external surface of the ilium. Each segment is innervated by a separate branch of the superior gluteal nerve. Its tendon attaches at two distinct facets on the greater trochanter. The anterior and most of the central fibers are attached to the lateral facet, and the posterior fibers are attached to the superoposterior facet16 (FIG 2).
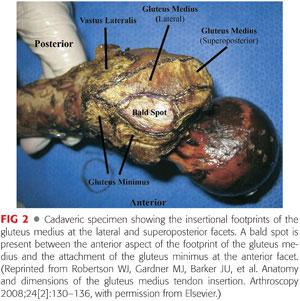
 The anterior and central insertion of the gluteus medius tendon on the lateral facet is rectangular in shape, occupying an area of approximately16 440 mm2. The portion of the tendon inserting into the superoposterior facet is more robust, with a circular shape, and a smaller surface area of approximately16 200 mm2.
The anterior and central insertion of the gluteus medius tendon on the lateral facet is rectangular in shape, occupying an area of approximately16 440 mm2. The portion of the tendon inserting into the superoposterior facet is more robust, with a circular shape, and a smaller surface area of approximately16 200 mm2.
 The fiber orientation of the gluteus medius is thought to correlate with function during the gait cycle. The anterior and middle muscle segments are vertically oriented and aid in initiating hip abduction.8 The anterior segment also externally rotates the pelvis during the swing phase of the contralateral limb.8 The fibers in the posterior segment are more horizontal and act to stabilize the hip joint at heel strike.8
The fiber orientation of the gluteus medius is thought to correlate with function during the gait cycle. The anterior and middle muscle segments are vertically oriented and aid in initiating hip abduction.8 The anterior segment also externally rotates the pelvis during the swing phase of the contralateral limb.8 The fibers in the posterior segment are more horizontal and act to stabilize the hip joint at heel strike.8
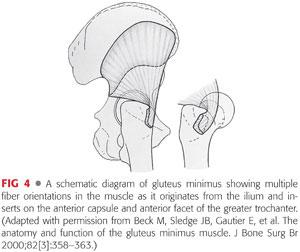
 The gluteus minimus also originates from the external ilium, running between the anterior inferior and posterior inferior iliac spines.1
The gluteus minimus also originates from the external ilium, running between the anterior inferior and posterior inferior iliac spines.1
 Distally, the gluteus minimus tendon attaches via two heads—the capsular head is fascial thickening that inserts into the superior aspect of the hip capsule, just anterior to greater trochanter at the iliofemoral ligament.1 The long head inserts on the inner aspect of the anterior margin of the greater trochanter at the anterior facet. The trochanteric insertion of the gluteus minimus is separated from the gluteus medius tendon footprint on the lateral facet by the trochanteric bald spot (FIG 3).
Distally, the gluteus minimus tendon attaches via two heads—the capsular head is fascial thickening that inserts into the superior aspect of the hip capsule, just anterior to greater trochanter at the iliofemoral ligament.1 The long head inserts on the inner aspect of the anterior margin of the greater trochanter at the anterior facet. The trochanteric insertion of the gluteus minimus is separated from the gluteus medius tendon footprint on the lateral facet by the trochanteric bald spot (FIG 3).

 The gluteus medius and minimus muscles have been likened to rotator cuff of the shoulder.3,10 The gluteus medius has a moment arm similar to both supraspinatus and infraspinatus with its lateral and superoposterior insertion on the greater trochanter.3 The gluteus minimus inserts on the anterior facet and has several different moments depending on the position of the femur relative to the pelvis—it can affect flexion, abduction, external, and internal rotation; and when these moments are counterbalanced, it acts as a primary stabilizer of the head in the socket.1 Due to the strong internal rotation moment of the gluteus minimus in many functional positions, its action is also analogous to the subscapularis (FIG 4).
The gluteus medius and minimus muscles have been likened to rotator cuff of the shoulder.3,10 The gluteus medius has a moment arm similar to both supraspinatus and infraspinatus with its lateral and superoposterior insertion on the greater trochanter.3 The gluteus minimus inserts on the anterior facet and has several different moments depending on the position of the femur relative to the pelvis—it can affect flexion, abduction, external, and internal rotation; and when these moments are counterbalanced, it acts as a primary stabilizer of the head in the socket.1 Due to the strong internal rotation moment of the gluteus minimus in many functional positions, its action is also analogous to the subscapularis (FIG 4).
 When repairing tears of the gluteus medius, familiarity with the insertional anatomy is essential to prevent overestimation of the size of the true tendon footprint. Incorporation of the bald spot into an anatomic footprint repair of the medius tendon can occur if anchors are mistakenly placed in the bald spot of the trochanter—a situation that should be avoided.17
When repairing tears of the gluteus medius, familiarity with the insertional anatomy is essential to prevent overestimation of the size of the true tendon footprint. Incorporation of the bald spot into an anatomic footprint repair of the medius tendon can occur if anchors are mistakenly placed in the bald spot of the trochanter—a situation that should be avoided.17
PATHOGENESIS
 Tears of the gluteus medius and minimus tendons were first described in the late 1990s and much like rotator cuff tendon tears in the shoulder, most likely result from a degenerative process.3,10,16
Tears of the gluteus medius and minimus tendons were first described in the late 1990s and much like rotator cuff tendon tears in the shoulder, most likely result from a degenerative process.3,10,16
 Tears of the gluteus medius can be interstitial, partial thickness or full thickness, with full-thickness tears tending to be large in size.16
Tears of the gluteus medius can be interstitial, partial thickness or full thickness, with full-thickness tears tending to be large in size.16
 Tears of the gluteus medius are significantly more common than those of the minimus. It follows that most tears occur in the anterior portion of the gluteus medius tendon as it attaches to the lateral facet of the greater trochanter.
Tears of the gluteus medius are significantly more common than those of the minimus. It follows that most tears occur in the anterior portion of the gluteus medius tendon as it attaches to the lateral facet of the greater trochanter.
 Tear propagation occurs by degeneration of the undersurface of the tear progressing posteriorly into a full-thickness tear.
Tear propagation occurs by degeneration of the undersurface of the tear progressing posteriorly into a full-thickness tear.
 Tears were initially identified in the setting of open release of the iliotibial band for recalcitrant trochanteric bursitis,10 total hip arthroplasty,9 and femoral neck fracture treatment.3
Tears were initially identified in the setting of open release of the iliotibial band for recalcitrant trochanteric bursitis,10 total hip arthroplasty,9 and femoral neck fracture treatment.3
 In performing iliotibial band release for trochanteric bursitis, Kagan10 found a partial tear of the gluteus medius in seven patients that was picked up on magnetic resonance imaging (MRI) but not on physical examination. Tears were repaired with nonabsorbable suture through bone tunnels and all patients were pain free at a median follow-up of 45 months.
In performing iliotibial band release for trochanteric bursitis, Kagan10 found a partial tear of the gluteus medius in seven patients that was picked up on magnetic resonance imaging (MRI) but not on physical examination. Tears were repaired with nonabsorbable suture through bone tunnels and all patients were pain free at a median follow-up of 45 months.
 In a series of 176 consecutive patients undergoing total hip arthroplasty for osteoarthritis, Howell et al9 found that 20% of the patients had degeneration of the abductor muscles with majority occurring in elderly women.
In a series of 176 consecutive patients undergoing total hip arthroplasty for osteoarthritis, Howell et al9 found that 20% of the patients had degeneration of the abductor muscles with majority occurring in elderly women.
 In a prospective study of 50 consecutive patients being treated for femoral neck fractures, Bunker et al3 found rotator cuff tears of the hip in 22% of patients. The typical appearance was described as a circular or oval defect in the insertion of gluteus medius and minimus tendons. The tears had a rolled edge and were often associated with free fluid in the trochanteric bursa and an eburnated underlying surface of the greater trochanter.3
In a prospective study of 50 consecutive patients being treated for femoral neck fractures, Bunker et al3 found rotator cuff tears of the hip in 22% of patients. The typical appearance was described as a circular or oval defect in the insertion of gluteus medius and minimus tendons. The tears had a rolled edge and were often associated with free fluid in the trochanteric bursa and an eburnated underlying surface of the greater trochanter.3
 A traumatic etiology in otherwise normal hips in the background of abductor tendinopathy is less common but can occur.13,15
A traumatic etiology in otherwise normal hips in the background of abductor tendinopathy is less common but can occur.13,15
NATURAL HISTORY
 Tendinopathy and tears of the abductor tendons are a common cause for intractable pain along the lateral side of the hip.
Tendinopathy and tears of the abductor tendons are a common cause for intractable pain along the lateral side of the hip.
 In patients with greater trochanteric pain syndrome (GTPS) where conservative management has failed, a high index of suspicion should be maintained for an abductor tear.
In patients with greater trochanteric pain syndrome (GTPS) where conservative management has failed, a high index of suspicion should be maintained for an abductor tear.
 In keeping with a degenerative etiology, patients describe lateral-sided hip pain that is insidious in onset and is usually debilitating.
In keeping with a degenerative etiology, patients describe lateral-sided hip pain that is insidious in onset and is usually debilitating.
 Degenerative abductor tear states likely to represent a continuum of pathology with partial-thickness tears eventually progressing to full-thickness tears over time if left untreated, much like the rotator cuff of the shoulder.
Degenerative abductor tear states likely to represent a continuum of pathology with partial-thickness tears eventually progressing to full-thickness tears over time if left untreated, much like the rotator cuff of the shoulder.
 Tears are four times more common in women than men and the prevalence increases with age.18 It is estimated that 25% of middle-aged women will develop a tear of the gluteus medius tendon. The increased incidence in women may partly be related to the wider female pelvis.9
Tears are four times more common in women than men and the prevalence increases with age.18 It is estimated that 25% of middle-aged women will develop a tear of the gluteus medius tendon. The increased incidence in women may partly be related to the wider female pelvis.9
 A full-thickness tear of the abductors is likely to cause severe lateral pain and a significant limp, resulting in a poor prognosis for those left untreated after failure of conservative management.
A full-thickness tear of the abductors is likely to cause severe lateral pain and a significant limp, resulting in a poor prognosis for those left untreated after failure of conservative management.
PATIENT HISTORY AND PHYSICAL FINDINGS
History
 Recalcitrant pain of insidious onset along the lateral side of the hip
Recalcitrant pain of insidious onset along the lateral side of the hip
 Pain may be exacerbated by walking, climbing stairs, lying on the affected hip, or resisted hip abduction.
Pain may be exacerbated by walking, climbing stairs, lying on the affected hip, or resisted hip abduction.
 The patient may report a slight or moderate limp.
The patient may report a slight or moderate limp.
 The symptoms show minimal improvement with conservative forms of treatment for a presumed diagnosis of trochanteric bursitis.
The symptoms show minimal improvement with conservative forms of treatment for a presumed diagnosis of trochanteric bursitis.
Physical Examination
 The patient’s gait should be observed for a limp, antalgia, or a frank Trendelenburg gait.
The patient’s gait should be observed for a limp, antalgia, or a frank Trendelenburg gait.
 If a Trendelenburg gait is suspected, a single-leg stance test should be conducted lasting 30 seconds or longer to look for a Trendelenburg sign—if positive, a distinct drop of the nonsupported pelvis is noted, indicating abductor weakness on the supported (single-leg stance) side. The Trendelenburg sign has been shown to be the most sensitive (73%) and specific (77%) physical sign for detection of abductor tears with an acceptable intraobserver reliability2 of 0.68.
If a Trendelenburg gait is suspected, a single-leg stance test should be conducted lasting 30 seconds or longer to look for a Trendelenburg sign—if positive, a distinct drop of the nonsupported pelvis is noted, indicating abductor weakness on the supported (single-leg stance) side. The Trendelenburg sign has been shown to be the most sensitive (73%) and specific (77%) physical sign for detection of abductor tears with an acceptable intraobserver reliability2 of 0.68.
 The patient should then be examined in the supine position for range of motion of the hip. Range of motion is usually preserved in abductor tears but care must be taken to note positions that provoke pain, particularly to rule out intra-articular causes of hip pain.
The patient should then be examined in the supine position for range of motion of the hip. Range of motion is usually preserved in abductor tears but care must be taken to note positions that provoke pain, particularly to rule out intra-articular causes of hip pain.
 An abduction external rotation test is useful in suspected GTPS. Reproduction of pain with the hip flexed to 45 degrees, in abduction, and external rotation may draw attention to inflamed soft tissue structures and bursae over the posterior facet of the greater trochanter. This examination maneuver brings the posterior facet in close proximity to the ischium and posterior wall of the acetabulum resulting in a crushing over the interposed soft tissues.
An abduction external rotation test is useful in suspected GTPS. Reproduction of pain with the hip flexed to 45 degrees, in abduction, and external rotation may draw attention to inflamed soft tissue structures and bursae over the posterior facet of the greater trochanter. This examination maneuver brings the posterior facet in close proximity to the ischium and posterior wall of the acetabulum resulting in a crushing over the interposed soft tissues.
 The resisted external derotation test is conducted with the patient lying supine, the hip flexed to 90 degrees and externally rotated to 30 degrees. The patient is then asked to internally rotate the hip to neutral against resistance. Reproduction of lateral pain when performing this maneuver has shown an 88% sensitivity and 97% specificity for detecting abductor tendinopathy.12
The resisted external derotation test is conducted with the patient lying supine, the hip flexed to 90 degrees and externally rotated to 30 degrees. The patient is then asked to internally rotate the hip to neutral against resistance. Reproduction of lateral pain when performing this maneuver has shown an 88% sensitivity and 97% specificity for detecting abductor tendinopathy.12
 The examination should then continue with the patient in a lateral decubitus position.
The examination should then continue with the patient in a lateral decubitus position.
 Deep palpation over the greater trochanter may reproduce the lateral-sided pain.
Deep palpation over the greater trochanter may reproduce the lateral-sided pain.
 An abduction strength test may reveal abductor weakness indicative of tendinopathy or tear. This test is performed with the hip in neutral flexion/extension, stabilizing the pelvis with one hand and asking the patient to actively abduct the hip against resistance. The test can be performed with the knees both flexed and extended to allow relaxation and tension of the iliotibial band, respectively.
An abduction strength test may reveal abductor weakness indicative of tendinopathy or tear. This test is performed with the hip in neutral flexion/extension, stabilizing the pelvis with one hand and asking the patient to actively abduct the hip against resistance. The test can be performed with the knees both flexed and extended to allow relaxation and tension of the iliotibial band, respectively.
 Ober test can also be performed to evaluate the hip abductors for tightness or a contracture.
Ober test can also be performed to evaluate the hip abductors for tightness or a contracture.
IMAGING AND OTHER DIAGNOSTIC STUDIES
 An anteroposterior (AP) radiograph of the pelvis and a Dunn lateral radiograph (90 degrees of hip flexion with 20 degrees of abduction and the beam centered on and perpendicular to the hip) are taken for the initial radiographic evaluation of all patients presenting with hip pain.
An anteroposterior (AP) radiograph of the pelvis and a Dunn lateral radiograph (90 degrees of hip flexion with 20 degrees of abduction and the beam centered on and perpendicular to the hip) are taken for the initial radiographic evaluation of all patients presenting with hip pain.
 Plain radiographs are usually normal in a patient with abductor tears in the setting of a nonarthritic hip, although enthesopathic calcifications may be seen in the region of the abductor insertions at the greater trochanter.
Plain radiographs are usually normal in a patient with abductor tears in the setting of a nonarthritic hip, although enthesopathic calcifications may be seen in the region of the abductor insertions at the greater trochanter.
 High-quality MRI is the investigation of choice for diagnosing abductor tears and should be requested based on clinical suspicion.
High-quality MRI is the investigation of choice for diagnosing abductor tears and should be requested based on clinical suspicion.
 Both noncontrast MRI and gadolinium-contrast magnetic resonance arthrogram (MRA) can be used to evaluate the hip joint, using coronal inversion recovery and axial proton density sequences.
Both noncontrast MRI and gadolinium-contrast magnetic resonance arthrogram (MRA) can be used to evaluate the hip joint, using coronal inversion recovery and axial proton density sequences.
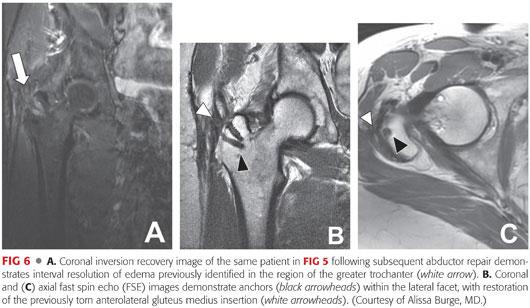
 Suspected gluteus medius tendon tears in patients with trochanteric bursitis may be confirmed with MRI.11 MRI has a high sensitivity and specificity for the diagnosis of gluteus medius and minimus tendons tears (FIG 5A–C).
Suspected gluteus medius tendon tears in patients with trochanteric bursitis may be confirmed with MRI.11 MRI has a high sensitivity and specificity for the diagnosis of gluteus medius and minimus tendons tears (FIG 5A–C).
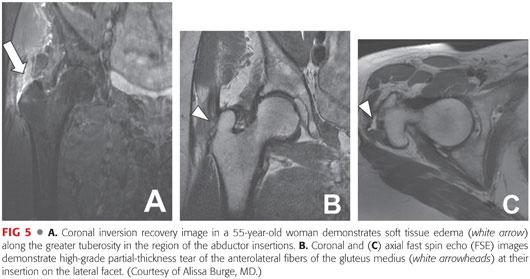
 MRI can differentiate between partial- and full-thickness abductor tears as well as identify calcific tendinitis and fatty atrophy within the muscle substance.
MRI can differentiate between partial- and full-thickness abductor tears as well as identify calcific tendinitis and fatty atrophy within the muscle substance.
 MRI can also be used to assess the healing and quality of repair tissue after surgical repair of the abductor tendons (FIG 6A–C).
MRI can also be used to assess the healing and quality of repair tissue after surgical repair of the abductor tendons (FIG 6A–C).
 Ultrasound can be used to evaluate gluteus medius and minimus tendinopathy and provide information about disease severity and tear size.4
Ultrasound can be used to evaluate gluteus medius and minimus tendinopathy and provide information about disease severity and tear size.4
DIFFERENTIAL DIAGNOSIS
 Greater trochanter bursitis
Greater trochanter bursitis
 Calcific tendinitis of the abductor tendons
Calcific tendinitis of the abductor tendons
 Greater trochanteric fracture
Greater trochanteric fracture
 Hip dysplasia
Hip dysplasia
 External coxa saltans (external snapping hip secondary to thickened iliotibial band)
External coxa saltans (external snapping hip secondary to thickened iliotibial band)
 Internal coxa saltans (internal snapping hip secondary to iliopsoas tendon pathology)
Internal coxa saltans (internal snapping hip secondary to iliopsoas tendon pathology)
 Piriformis syndrome (sciatic nerve compression)
Piriformis syndrome (sciatic nerve compression)
 Lumbar radiculopathy
Lumbar radiculopathy
 Sacroiliac joint pain
Sacroiliac joint pain
NONOPERATIVE MANAGEMENT
 Nonoperative treatment options can help alleviate pain and improve patient lifestyle.
Nonoperative treatment options can help alleviate pain and improve patient lifestyle.
 Conservative management begins with patient education regarding the diagnosis and natural history of the condition. All options are discussed, and a nonoperative approach is typically taken initially in treating abductor tears.
Conservative management begins with patient education regarding the diagnosis and natural history of the condition. All options are discussed, and a nonoperative approach is typically taken initially in treating abductor tears.
 This approach includes rest, ice, anti-inflammatory medication, and physical therapy focused on range-of-motion exercises, strengthening, and gait mechanics.
This approach includes rest, ice, anti-inflammatory medication, and physical therapy focused on range-of-motion exercises, strengthening, and gait mechanics.
 If symptoms persist despite the previous interventions, we consider ultrasound-guided injections of local anaesthetic and platelet-rich plasma in MRI-confirmed abductor tears. Corticosteroid injections are reserved for patients with GTPS in the setting of a normal abductor insertion.
If symptoms persist despite the previous interventions, we consider ultrasound-guided injections of local anaesthetic and platelet-rich plasma in MRI-confirmed abductor tears. Corticosteroid injections are reserved for patients with GTPS in the setting of a normal abductor insertion.
SURGICAL MANAGEMENT
 Surgical intervention is indicated for patients who have failed conservative treatment and remain symptomatic with lateral pain and weakness.
Surgical intervention is indicated for patients who have failed conservative treatment and remain symptomatic with lateral pain and weakness.
 Abductor repairs can be performed open or endoscopically.
Abductor repairs can be performed open or endoscopically.
 We reserve open repairs for complete avulsions of the abductor tendons from the greater trochanter with retraction on MRI. We believe that an open repair can afford a more durable repair in the setting of complete tendon avulsion with retraction but that repair of larger tears may be feasible endoscopically as techniques improve.
We reserve open repairs for complete avulsions of the abductor tendons from the greater trochanter with retraction on MRI. We believe that an open repair can afford a more durable repair in the setting of complete tendon avulsion with retraction but that repair of larger tears may be feasible endoscopically as techniques improve.
 Endoscopic repair of the abductor tendons can be performed reproducibly and results in resolution of pain and return to activity in a predictable manner in the short term.
Endoscopic repair of the abductor tendons can be performed reproducibly and results in resolution of pain and return to activity in a predictable manner in the short term.
 Entry into the peritrochanteric space typically follows routine evaluation and treatment of pathology in the central and peripheral compartments.
Entry into the peritrochanteric space typically follows routine evaluation and treatment of pathology in the central and peripheral compartments.
 Irrespective of technique, a working knowledge of the anatomy of the abductor tendon footprint on the greater trochanter is critical to identify the site of injury at the time of endoscopy and to subsequently execute an anatomic repair.
Irrespective of technique, a working knowledge of the anatomy of the abductor tendon footprint on the greater trochanter is critical to identify the site of injury at the time of endoscopy and to subsequently execute an anatomic repair.
Preoperative Planning
 Preoperative planning consists of a thorough history and physical examination confirming that the symptoms are originating from the lateral compartment of the hip.
Preoperative planning consists of a thorough history and physical examination confirming that the symptoms are originating from the lateral compartment of the hip.
 Any pathology in the central and peripheral compartments that can be treated arthroscopically has been identified and surgical intervention planned based on clinical and radiologic findings.
Any pathology in the central and peripheral compartments that can be treated arthroscopically has been identified and surgical intervention planned based on clinical and radiologic findings.
 A recent plain radiograph is available, as progressive joint space deterioration may contraindicate an arthroscopic procedure.
A recent plain radiograph is available, as progressive joint space deterioration may contraindicate an arthroscopic procedure.
 A recent MRI scan is available, confirming the presence of an abductor tear that is amenable to endoscopic repair.
A recent MRI scan is available, confirming the presence of an abductor tear that is amenable to endoscopic repair.
Positioning
 As a peritrochanteric space endoscopy typically follows routine arthroscopy of the central and peripheral compartments, the patient should already be set up on a standard operating room (OR) table with specialized lower extremity attachment.
As a peritrochanteric space endoscopy typically follows routine arthroscopy of the central and peripheral compartments, the patient should already be set up on a standard operating room (OR) table with specialized lower extremity attachment.
 No distraction is required, and therefore, the perineal post is removed.
No distraction is required, and therefore, the perineal post is removed.
 Both feet are secured in well-padded boots.
Both feet are secured in well-padded boots.
 The nonoperative hip is placed in slight abduction, neutral extension, and full extension at the knee.
The nonoperative hip is placed in slight abduction, neutral extension, and full extension at the knee.
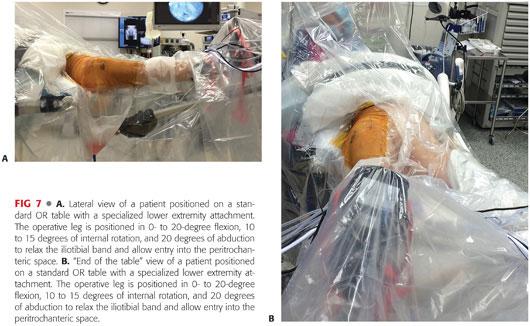
 The operative lower extremity is placed in 0 to 20 degrees flexion, 10 to 15 degrees internal rotation, and 20 degrees abduction to relax the iliotibial band and allow entry into the potential space between the greater trochanter and iliotibial band (FIG 7A,B).
The operative lower extremity is placed in 0 to 20 degrees flexion, 10 to 15 degrees internal rotation, and 20 degrees abduction to relax the iliotibial band and allow entry into the potential space between the greater trochanter and iliotibial band (FIG 7A,B).
Approach
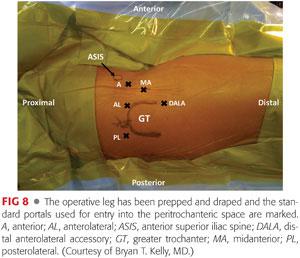
 The anterior and midanterior (MA) portals can be both used to access the peritrochanteric space (FIG 8).
The anterior and midanterior (MA) portals can be both used to access the peritrochanteric space (FIG 8).
 Both these anterior portals are placed lateral to the anterior superior iliac spine (ASIS) to avoid injury to the LFCN and pass through the interval between the tensor fascia latae and sartorius.
Both these anterior portals are placed lateral to the anterior superior iliac spine (ASIS) to avoid injury to the LFCN and pass through the interval between the tensor fascia latae and sartorius.
 We routinely use the MA portal to enter the peritrochanteric space. This portal is 2 cm distal and lateral to the standard anterior portal.
We routinely use the MA portal to enter the peritrochanteric space. This portal is 2 cm distal and lateral to the standard anterior portal.
 The MA portal has two distinct advantages over the standard anterior portal:
The MA portal has two distinct advantages over the standard anterior portal:
It further reduces the risk of injury to the LFCN, as it is placed even more lateral to the ASIS compared to the standard anterior portal.16
It lies directly over the lateral flare of the greater trochanter and therefore is just distal to the gluteus medius muscle belly and proximal to the vastus lateralis. This position avoids injury to the abductor muscle mass when passing instruments to facilitate repair.
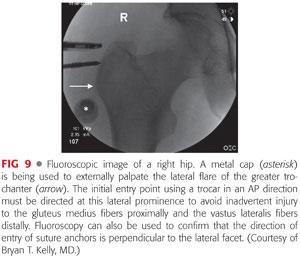
 Fluoroscopy is used to aid in proper placement of the MA portal by confirming placement directly over the lateral flare of the greater trochanter and proximal to the vastus ridge (FIG 9). This placement prevents inadvertent proximal gluteus medius and distal vastus lateralis muscular injury.
Fluoroscopy is used to aid in proper placement of the MA portal by confirming placement directly over the lateral flare of the greater trochanter and proximal to the vastus ridge (FIG 9). This placement prevents inadvertent proximal gluteus medius and distal vastus lateralis muscular injury.
 Three portals are usually sufficient to complete an endoscopic abductor repair (MA, anterolateral, and distal anterolateral accessory [DALA]). Occasionally, the posterolateral portal is also used (see FIG 8).
Three portals are usually sufficient to complete an endoscopic abductor repair (MA, anterolateral, and distal anterolateral accessory [DALA]). Occasionally, the posterolateral portal is also used (see FIG 8).
TECHNIQUES
 Establishing Primary Viewing Portal
Establishing Primary Viewing Portal
After establishing the position for the MA portal under fluoroscopic guidance, a blunt plastic cannula is directed into the peritrochanteric space in an anterior to posterior direction.
The cannula is swept back and forth between the trochanteric bursa and iliotibial band to release any adhesions in a fashion similar to that used when entering the subacromial space of the shoulder.
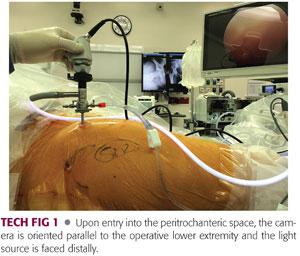
Once the appropriate plane is identified, the space is distended with 50 mm Hg of fluid pressure and a 70-degree scope is introduced and locked into the plastic cannula.
The light source and camera are oriented such that the light source is facing distally and the camera is parallel to the operative leg (TECH FIG 1).
 Bursectomy and Establishing Visualization
Bursectomy and Establishing Visualization
Upon entry into the peritrochanteric space, the DALA portal is established using a standard Seldinger technique (see FIG 8). This portal is in line with the anterolateral portal, 4 to 5 cm directly distal to it.
A motorized shaver is inserted into the peritrochanteric space through this portal, and the trochanteric bursa is thoroughly cleared (TECH FIG 2).
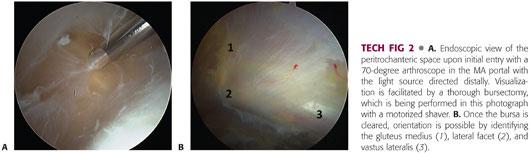
The bursectomy begins distally at the gluteus maximus insertion into the femur and progresses proximally in a systematic fashion. This should allow easy visualization of the iliotibial band and greater trochanter, which define the lateral and medial borders of the peritrochanteric space, respectively.
The standard anterolateral portal can then be used as a third working or viewing portal, improving proximal access or distal visualization.
 Establishing Orientation in Peritrochanteric Space
Establishing Orientation in Peritrochanteric Space
The first structure that must be identified on establishing adequate visualization is the gluteus maximus tendon inserting on the femur just below the vastus lateralis (TECH FIG 3A).
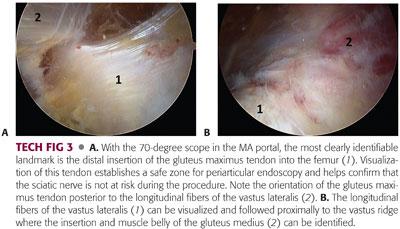
This is a reproducible landmark that establishes a safe zone—the sciatic nerve lies 3 to 4 cm posterior to the gluteus maximus insertion, and therefore, exploration posterior to the tendon should be avoided. Working distal to this tendon insertion is usually unnecessary.
The light source is then directed to the lateral aspect of the femur where the longitudinal fibers of the vastus lateralis can be visualized and followed proximally to the vastus ridge. Proximal to the vastus ridge, the insertion and muscle belly of the gluteus medius is identified by directing the light source anterosuperiorly (TECH FIG 3B).
 Evaluation of the Abductor Attachment
Evaluation of the Abductor Attachment
The gluteus medius muscle and insertion are then evaluated at the lateral facet. The entire tendon should be inspected and carefully probed.
The gluteus medius muscle and tendon are best visualized with arthroscope in the proximal anterolateral portal, which gives a global view of the abductors. The light source is rotated to visualize anterosuperiorly.
The working instruments can then be placed in the MA and DALA portals.
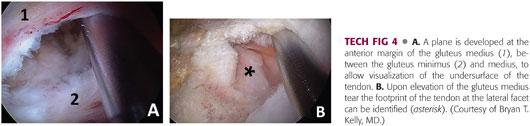
The gluteus minimus is often covered by the gluteus medius muscle and can be difficult to visualize. A switching stick can be used to gently retract medius muscle to see the tendinous insertion of the gluteus minimus onto the anterior facet (TECH FIG 4).
Most commonly, the gluteus medius is degenerated and torn off its distal insertion on the lateral facet of the greater trochanter.
Undersurface partial tears can also occur, but in case of significant thinning of the tendon insertion, the tear should be completed and repaired.
 Preparation for Endoscopic Abductor Repair
Preparation for Endoscopic Abductor Repair
If a tear in the gluteus medius is identified, it must be assessed for retraction and repairability similar to tears of the rotator cuff of the shoulder (TECH FIG 5A,B).
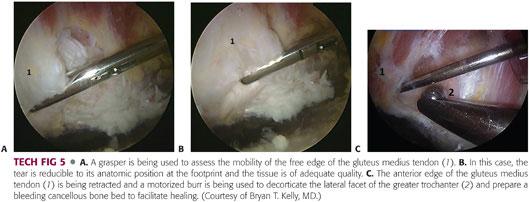
A probe or grasper is used to manually reduce the tear to its anatomic position in the footprint in order to determine the tissue quality as well as the tendon mobility.
A mechanical shaver is used to débride the edges of the tear to healthy, robust tissue.
A motorized burr is used to decorticate the lateral facet of the greater trochanter and prepare a bleeding cancellous bone bed to facilitate healing (TECH FIG 5C).
 Endoscopic Rotator Cuff Repair of the Hip
Endoscopic Rotator Cuff Repair of the Hip
Due to the hard nature of bone in the greater trochanter, metallic or peek anchors are usually used for repair. The position of metallic anchors can be confirmed with fluoroscopy.
Typically, two anchors will suffice to repair the anatomic footprint of a gluteus medius tendon tear off the lateral facet. Adequate spacing of anchors must be allowed for good bone stock to be present between anchors.
To obtain the optimal trajectory for anchor placement, a spinal needle is placed first, and positioned with arthroscopic and fluoroscopic guidance. Anchors are then placed into the footprint through percutaneous stab incisions followed by confirmation of anchor position by fluoroscopy (TECH FIG 6A).
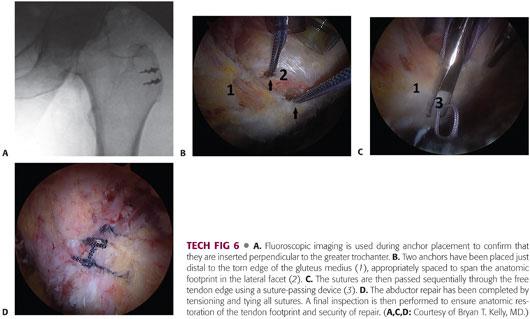
After anchor placement, sutures are passed sequentially through the free tendon edge using a suture-passing device (TECH FIG 6B,C). The tendon edge can be captured with a needle-penetrating device placed through the DALA portal. Sutures are then parked in the MA portal.
All sutures should be passed through long hip cannulas to avoid soft tissue entrapment.
After all the sutures have been passed, arthroscopic sliding, locking knots are placed with a knot pusher to secure the gluteus medius and minimus back to their native footprint on the greater trochanter (TECH FIG 6D). We prefer to place two mattress stitches that are perpendicular to one another from a single suture anchor.
Careful evaluation of the tendon repair should be performed to confirm anatomic restoration of the tendon footprint and security of repair.
 Surgical Management of Partial-Thickness Abductor Tears
Surgical Management of Partial-Thickness Abductor Tears
Partial-thickness undersurface tears that are seen on MRI are often difficult to see arthroscopically.
These tears are analogous to an articular-sided rotator cuff tear of the shoulder, which extends posteriorly and may become a full-thickness tear.
In contrast to rotator cuff tears of the shoulder, there is no space in the peritrochanteric compartment analogous to the intra-articular space of the shoulder from where the undersurface of a gluteus medius partial-thickness tear can be visualized.
These tears may be better visualized by developing a plane at the anterior margin of the gluteus medius, between the gluteus minimus and medius.
If they are high-grade lesions, they may be converted to a full-thickness tear and repaired using the previously described technique.
A transtendinous repair is also possible and the technique has been described.6
A longitudinal split in the gluteus medius insertion at the lateral facet is made.
The undersurface tearing of the tendon is visualized through the split.
The arthroscope is inserted through the split to better visualize the undersurface tearing.
A shaver is used to débride pathologic tissue and a burr is used to decorticate the lateral facet.
Anchors are then placed through the tendon split under fluoroscopic guidance.
Suture-passing devices are used to pass one limb of each suture through the anterior and posterior parts of the tendon.
All sutures are tied down to effect a side-to-side repair of the tendon split while securing the tendon to the lateral facet.
PEARLS AND PITFALLS | |
Pearls |
|
| |
| |
| |
| |
Pitfalls |
|
| |
| |








POSTOPERATIVE CARE
 Twenty pounds of foot-flat weight bearing is permitted for the first 6 weeks with the aid of crutches.
Twenty pounds of foot-flat weight bearing is permitted for the first 6 weeks with the aid of crutches.
 Abduction brace locked at 10 degrees of hip abduction
Abduction brace locked at 10 degrees of hip abduction
 Continuous passive motion initiated immediately for 4 hours per day and stationary biking for 20 minutes per day for the first 6 weeks to prevent adhesions.
Continuous passive motion initiated immediately for 4 hours per day and stationary biking for 20 minutes per day for the first 6 weeks to prevent adhesions.
 No active abduction and internal rotation or passive adduction and external rotation for the first 6 weeks to preserve repair integrity.
No active abduction and internal rotation or passive adduction and external rotation for the first 6 weeks to preserve repair integrity.
 Passive hip flexion to 90 degrees and passive abduction as pain allows are permitted for the first 6 weeks.
Passive hip flexion to 90 degrees and passive abduction as pain allows are permitted for the first 6 weeks.
 Passive hip flexion beyond 90 degrees is permitted after the first 6 weeks.
Passive hip flexion beyond 90 degrees is permitted after the first 6 weeks.
 Sutures are removed in 10 to 14 days and scar massage of the portals is commenced thereafter.
Sutures are removed in 10 to 14 days and scar massage of the portals is commenced thereafter.
 Isometric strengthening of the hip adductors, extenders, and external rotators is commenced after the first 2 weeks.
Isometric strengthening of the hip adductors, extenders, and external rotators is commenced after the first 2 weeks.
 Active strengthening is commenced at 6 weeks postoperatively, starting with isometric submaximal hip flexion and quadriceps strengthening.
Active strengthening is commenced at 6 weeks postoperatively, starting with isometric submaximal hip flexion and quadriceps strengthening.
 Progression to weight bearing as tolerated with crutches is permitted at 6 to 8 weeks postoperatively.
Progression to weight bearing as tolerated with crutches is permitted at 6 to 8 weeks postoperatively.
 Progressive hip range-of-motion exercises with passive internal and external rotation are commenced at 8 weeks postoperatively.
Progressive hip range-of-motion exercises with passive internal and external rotation are commenced at 8 weeks postoperatively.
 After 10 weeks, lower extremity and core strengthening are progressed as tolerated.
After 10 weeks, lower extremity and core strengthening are progressed as tolerated.
 Between 3 and 6 months, patients should be pain free, demonstrate quadriceps and hamstrings peak torque strength within 15% of the contralateral extremity, and demonstrate a normal stepdown test.
Between 3 and 6 months, patients should be pain free, demonstrate quadriceps and hamstrings peak torque strength within 15% of the contralateral extremity, and demonstrate a normal stepdown test.
OUTCOMES
 Outcomes data of endoscopic gluteus medius repairs are limited to small case series at short-term follow-up.
Outcomes data of endoscopic gluteus medius repairs are limited to small case series at short-term follow-up.
 Voos et al18 reported on the outcomes of 10 patients (mean age 50 years) who underwent endoscopic repair of full-thickness gluteus medius tears, with a mean follow-up of 25 months. All patients had complete resolution of pain with mean modified Harris hip scores of 94 points and hip outcomes scores of 93 points at final follow-up.
Voos et al18 reported on the outcomes of 10 patients (mean age 50 years) who underwent endoscopic repair of full-thickness gluteus medius tears, with a mean follow-up of 25 months. All patients had complete resolution of pain with mean modified Harris hip scores of 94 points and hip outcomes scores of 93 points at final follow-up.
 Domb et al5 reported on 15 patients with an average age of 58 years at a mean follow-up of 28 months. Their series included six partial-thickness and nine full-thickness tears. Satisfaction with the surgery was good to excellent for 14 of 15 patients and outcomes scores improved by more than 30 points on four different hip-specific scoring scales.
Domb et al5 reported on 15 patients with an average age of 58 years at a mean follow-up of 28 months. Their series included six partial-thickness and nine full-thickness tears. Satisfaction with the surgery was good to excellent for 14 of 15 patients and outcomes scores improved by more than 30 points on four different hip-specific scoring scales.
 McCormick et al14 studied 10 patients with an average age of 66 years at a mean follow-up of 23 months. All patients underwent endoscopic repair of full-thickness abductor tears. All patients had good to excellent outcomes with improved strength. They also noted that younger patients achieved better outcomes.
McCormick et al14 studied 10 patients with an average age of 66 years at a mean follow-up of 23 months. All patients underwent endoscopic repair of full-thickness abductor tears. All patients had good to excellent outcomes with improved strength. They also noted that younger patients achieved better outcomes.
COMPLICATIONS
 In comparison to central and peripheral compartment hip arthroscopy, periarticular endoscopy of the peritrochanteric space has a lower complication rate.
In comparison to central and peripheral compartment hip arthroscopy, periarticular endoscopy of the peritrochanteric space has a lower complication rate.
 No serious complications have been reported in the literature.14,18
No serious complications have been reported in the literature.14,18
 Potential risks of LFCN neurapraxia and significant fluid extravasation into the thigh do exist, but the incidence is not known.
Potential risks of LFCN neurapraxia and significant fluid extravasation into the thigh do exist, but the incidence is not known.
REFERENCES
1. Beck M, Sledge JB, Gautier E, et al. The anatomy and function of the gluteus minimus muscle. J Bone Joint Surg Br 2000;82(3):358–363.
2. Bird PA, Oakley SP, Shnier R, et al. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum 2001;44(9):2138–2145.
3. Bunker TD, Esler CN, Leach WJ. Rotator-cuff tear of the hip. J Bone Joint Surg Br 1997;79(4):618–620.
4. Connell DA, Bass C, Sykes CA, et al. Sonographic evaluation of gluteus medius and minimus tendinopathy. Eur Radiol 2003;13(6):1339–1347.
5. Domb BG, Botser I, Giordano BD. Outcomes of endoscopic gluteus medius repair with minimum 2-year follow-up. Am J Sports Med 2013;41(5):988–997.
6. Domb BG, Nasser RM, Botser IB. Partial-thickness tears of the gluteus medius: rationale and technique for trans-tendinous endoscopic repair. Arthroscopy 2010;26(12):1697–1705.
7. Dwek J, Pfirrmann C, Stanley A, et al. MR imaging of the hip abductors: normal anatomy and commonly encountered pathology at the greater trochanter. Magn Reson Imaging Clin N Am 2005;13(4):691–704.
8. Gottschalk F, Kourosh S, Leveau B. The functional anatomy of tensor fasciae latae and gluteus medius and minimus. J Anat 1989;166:179–189.
9. Howell GE, Biggs RE, Bourne RB. Prevalence of abductor mechanism tears of the hips in patients with osteoarthritis. J Arthoplasty 2001;16(1):121–123.
10. Kagan A II. Rotator cuff tears of the hip. Clin Orthop Relat Res 1999;(368):135–140.
11. Lequesne M, Djian P, Vuillemin V, et al. Prospective study of refractory greater trochanter pain syndrome. MRI findings of gluteal tendon tears seen at surgery. Clinical and MRI results of tendon repair. Joint Bone Spine 2008;75(4):458–464.
12. Lequesne M, Mathieu P, Vuillemin-Bodaghi V, et al. Gluteal tendinopathy in refractory greater trochanter pain syndrome: diagnostic value of two clinical tests. Arthritis Rheum 2008;59(2):241–246.
13. Lonner JH, Van Kleunen JP. Spontaneous rupture of the gluteus medius and minimus tendons. Am J Orthop 2002;31(10):579–581.
14. McCormick F, Alpaugh K, Nwachukwu BU, et al. Endoscopic repair of full-thickness abductor tendon tears: surgical technique and outcome at minimum of 1-year follow-up. Arthroscopy 2013;29(12):1941–1947.
15. Ozcakar L, Erol O, Kaymak B, et al. An underdiagnosed hip pathology: a propos of two cases with gluteus medius tendon tears. Clin Rheumatol 2004;23(5):464–466.
16. Robertson WJ, Gardner MJ, Barker JU, et al. Anatomy and dimensions of the gluteus medius tendon insertion. Arthroscopy 2008;24(2):130–136.
17. Voos JE, Rudzki JR, Shindle MK, et al. Arthroscopic anatomy and surgical techniques for peritrochanteric space disorders in the hip. Arthroscopy 2007;23(11):1246.e1–e5.
18. Voos JE, Shindle MK, Pruett A, et al. Endoscopic repair of gluteus medius tendon tears of the hip. Am J Sports Med 2009;37(4):743–747.
< div class='tao-gold-member'>



