Arterial Reconstruction with an Aortic Conduit
Amit K. Mathur
Theodore H. Welling
DEFINITION
Hepatic artery reconstruction during liver transplantation is rarely required to the recipient aorta for use as arterial inflow.
PATIENT HISTORY AND PHYSICAL FINDINGS
Recipients may have significant celiac arterial or hepatic arterial occlusive disease. This may present during evaluation of first-time recipients either preoperatively or during the liver transplant.
Recipients may have an anatomically diminutive hepatic artery with respect to the donor hepatic artery.
Recipients may have significant hepatic arterial insufficiency related to a prior liver transplant.
Recipients may have a history of prior neoadjuvant radiotherapy to the porta hepatis (e.g., hilar cholangiocarcinoma protocols).
IMAGING AND OTHER DIAGNOSTIC STUDIES
The recipient may have undergone preoperative cross-sectional imaging (computed tomography [CT] or magnetic resonance imaging [MRI]) to evaluate for possible malignancy or portal vein thrombosis whereupon celiac or hepatic arterial stenosis is noted.
SURGICAL MANAGEMENT
Preoperative Planning
If hepatic arterial reconstruction is thought to be likely, consideration of donors with suitable arterial conduit is advised such that donor iliac artery is relatively free of atherosclerotic or other arterial disease.
If aortic conduit creation is being considered, recipient preoperative cross-sectional imaging of the aorta may be helpful to determine if areas of calcification or plaque are present in areas where vascular clamps would be applied.
TECHNIQUES
BACKBENCH OF THE DONOR CONDUIT
The donor iliac artery or vein can be used for conduit; however, the artery is least prone to kinking and therefore is most preferred (FIG 1).
The conduit is prepared by removing any excess tissue and ligating any branches with silk ties.
Examination for any evidence of intimal dissection or ruptured atherosclerotic plaque should be made.
 FIG 1 • Preparation of aortic conduit from donor iliac artery. |
AORTIC EXPOSURE
The supraceliac recipient aorta is most commonly used for the site of the proximal anastomosis. In cases where a conduit is already known to be required, this may be exposed prior to completion of hepatectomy if desired (FIG 2).
The crural fibers are divided, overlying the aorta just above the celiac artery.
Palpation of the aorta is performed to verify relative absence of atherosclerotic disease.
The infrarenal aorta can also be used for inflow if the supraceliac aorta is prohibitive.
Aortic dissection such that appropriate aortic clamps can be applied to allow access to the anterior surface of the aorta. Circumferential vascular control of the aorta is not needed and only increases the risk of injury to the lumbar arteries. If injured, these can be difficult to control.
A Weitlaner or Beckman-Adson retractor is often useful to provide exposure.
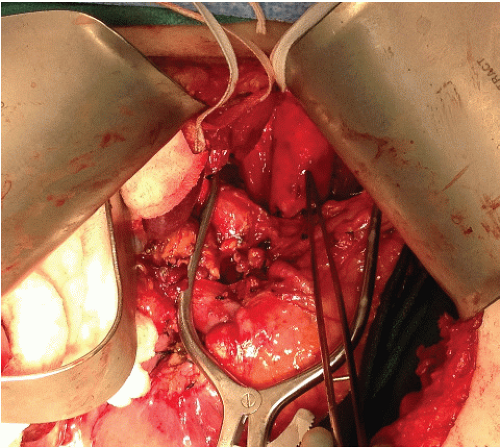 FIG 2 • Supraceliac aortic exposure. Forceps are pointing to the anterior aspect of the aorta. Preaortic tissue is being retracted with a Weitlaner retractor.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





