Fig. 21.1
Incision and suture of the blood vessels. (a) Incision of vascular wall. (b) Incision extension. (c) Excision of the lesion. (d) Suture start. (d) Suture completion
The vascular suture materials are necessary for repair and reconstruction of the blood vessels, which need to maintain tension for a long time, and the nonabsorbable suture lines should be used. Currently, more commonly used suture lines include polypropylene line (Prolene), nylon line, and various polyethylene (dacron) noninvasive lines. The silk thread should not be used to suture the artificial blood vessels. For different vessels, it is very important to choose the right type of vascular suture line; generally, the 3-0 suture lines are used to suture the thoracic aorta; the 4-0 suture lines are used to suture the abdominal aorta; the 5-0 suture lines are selectively used to suture the iliac artery; the 6-0 suture lines are selectively used to suture the femoral artery and brachial artery; the 7-0 suture lines are selectively used to suture the visceral arteries, lower extremity arteries, and forearm arteries; and the 8-0 to 10-0 suture lines are selectively used to suture the arteries in foots and hands.
The artificial blood vessels are the commonly used method for repair and reconstruction of the blood vessels; the nylon material will be absorbed in the body, and thus it has been eliminated. Currently, more commonly used artificial blood vessels are polyester artificial blood vessels, ePTEF artificial blood vessels.
2.2 The Basic Operations for the Repair and Reconstruction of Blood Vessel
2.2.1 Basic Principles
- 1.
Avoid damages to the vascular intima due to surgical instruments, and the vascular intima which has been damaged must be removed.
- 2.
The vascular adventitia is clearly separated as far as possible; it should be avoided that the vascular adventitia is brought into the vessel lumen.
- 3.
When the vascular intima is exposed, it should be avoided that the vascular intima is dry or has blood or blood clot, and it should be washed cleanly with heparin saline.
- 4.
After the blood vessel is occluded, 0.5 mg/kg unfractionated heparin should be used to achieve partial heparinization and prevent the thrombosis when the blood flow is slow.
- 5.
When the blood vessels are repaired and reconstructed, the vascular intimas must be aligned completely and are sutured with the suture line of proper size and the stitch length, and margin distance should be properly mastered; when there is a tension, the blood vessel transplantation must be carried out to eliminate the tension.
2.2.2 Basic Methods
- 1.
Separation and exposure of the blood vessels. During repair and reconstruction of the blood vessels, the first step is to separate and expose the blood vessels. Under normal conditions, the vessel sheath is exposed firstly, and there is a vascular sheath or arterial sheath constituted by a thin layer of tissue around the blood vessels. The difficulty of separating the blood vessels often depends on whether the sheath is normal. The arterial sheath can be longitudinally incised; the blunt dissections along both sides of the blood vessel are carried out successively; when the rear wall is separated, special attention should be paid to avoid damage to the rear wall or the branch issued from this site, which leads to uncontrolled bleeding. The performer must not be too hasty, after passing through the rear wall of the blood vessel; the vascular blocking belt is used to penetrate through and is lifted, and the artery sidewall can be separated toward the proximal and distal ends under direct vision.
When the tumor involves the perivascular tissue, due to perivascular fibrosis or tumor wrapping, the blood vessels are often difficult to identify or separate. A few milliliters of normal saline or procaine solution can be injected into the superficial layer of the vascular sheath, which is conducive to the separation of the vascular sheath. If the tissues surrounding the artery have lesions, extensive fibrosis, or significant inflammatory hyperemia, it will be difficult to separate the arterial trunk, and it is easy to damage its branches during the separation.
- 2.
Temporary vascular occlusion. The temporary vascular occlusion includes the transverse vascular occlusion, partial vascular occlusion, and endovascular balloon occlusion. The vascular blocking belt or noninvasive vascular clamp is used to clamp the vascular wall to occlude the artery, the sidewall clamp can partially occlude the artery, and some blood can still flow through the blood vessel. Because there exist no completely noninvasive artery forceps, the medium-sized arteries such as the femoral artery, popliteal artery, and brachial artery can be occluded with the vascular blocking belt or rubber belt, and the large arteries such as the aorta and iliac artery can be occluded with the noninvasive vascular clamp. When the artery is incised or ruptured, the balloon catheter or Foley catheter can be inserted into the bleeding blood vessel, and the balloon is filled to occlude the blood vessels.
The times of occlusion tolerances of the arteries are different owing to the different tissues and locations: the brain and kidney are most sensitive to hypoxia; the occlusion time of the thoracic aorta should not exceed 15–30 min, unless the sufficient collateral circulation has been originally formed; otherwise, it may cause paralysis; the abdominal aorta under the level of the renal artery cannot be occluded for a long time, because long-term striated muscle ischemia can lead to the serious myonephropathic-metabolic syndrome, thereby forming the myoglobinuria, renal failure, and even lower limb gangrene. In principle, the occlusion times of the main arteries should be minimized to the greatest extent; the internal bypass or external bypass and low temperature measure or extracorporeal circulation are applied if necessary.
- 3.
The dissociation and harvesting of the great saphenous vein. The situation of the involved blood vessels to be repaired and reconstructed should be confirmed; simultaneously, it is required to confirm whether the great saphenous vein has lesions. According to the length of the blood vessel to be reconstructed, the skin incision is made along the running course of the great saphenous vein, and the great saphenous vein of proper length is harvested. When the great saphenous vein is dissociated, the operation must be gentle, even the very thin branches should also be ligated and cut off, and the ligation sites of the branches should have a distance 2–3 mm from the great saphenous vein; in order to avoid that, after the great saphenous vein is transplanted to the artery, the local stenosis is formed due to the expanded blood vessel diameter. After the great saphenous vein is harvested, it is infused slowly with heparin saline or plasma to expand it; if the leakage points are found, the 6-0 noninvasive vascular suture line is used for longitudinal repair. Attention must be paid to the direction of the venous valve during transplantation, or the venous valve is destroyed by the valvulotome.
- 4.
Vascular suture technique. The methods for vascular suture include continuous suture ligation, interrupted suture, interrupted mattress suture, continuous mattress suture, and endovascular suture, and the selection of various anastomosis methods should be determined according to specific situation:
- (1)
Direct vascular anastomosis: This surgical method does not require the use of blood vessel transplantation, including vascular incision anastomosis, end-to-end vascular anastomosis, and end-to-side vascular anastomosis. The end-to-end anastomosis of the blood vessels of above average diameter can be performed with annular continuous suture ligation; the end-to-end anastomosis of the small blood vessels can be performed with continuous suture ligation or interrupted suture. The blood vessels of large and medium size can be sutured with 3-0 to 6-0 vascular suture lines; the suture needle distance and margin distance are 2–3 mm, which are determined according to the thickness of the blood vessel wall and the situation of the lesions in blood vessels and surrounding tissue. The small vascular anastomosis must overcome vasospasm, the method of mechanical expansion is preferably adopted, the 6-0 to 9-0 suture lines can be selected, and both the needle distance and margin distance are less than 0.5–1 mm (Figs. 21.1, 21.2, and 21.3). The method for end-to-side anastomosis of the blood vessels is essentially the same method as described above (Fig. 21.4), which is generally applied in blood vessel bypass transplantation; the lateral opening of the front end should be cut into oval incision with about 30° oblique angle; the anterior angle cannot be too sharp. The longitudinal incision in the arterial wall of the trunk end should be greater than its diameter, and the angle for carrying out bypass transplantation with the transplanted blood vessel should be less than 45°, which is more conducive to unobstructed blood flow.
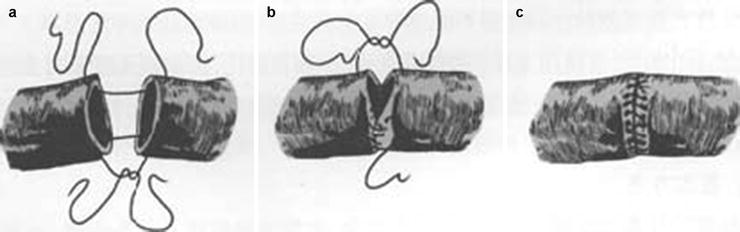
Fig. 21.2
End-to-end vascular anastomosis. (a) Anchoring. (b) Suturing. (c) Completion
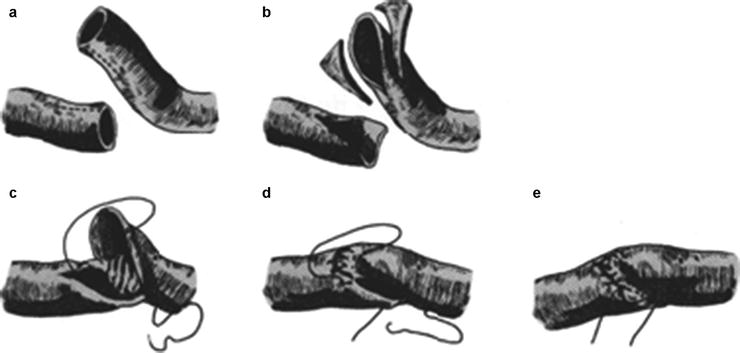
Fig. 21.3
Oblique end-to-end vascular anastomosis. (a) Preparation. (b) Oblique trimming. (c) Anchoring. (d) Suturing. (e) Completion
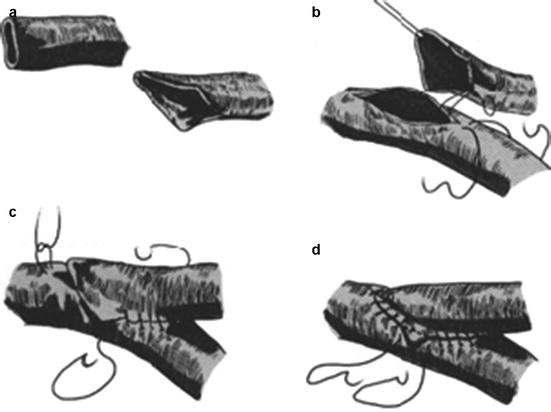
Fig. 21.4
End-to-side vascular anastomosis. (a) Preparation. (b) Anchoring. (c) Suturing. (d) Completion
- (2)
Usage of vascular graft material, including patch repair of vascular incisions (Fig. 21.5), end-to-end anastomosis, or end-to-side anastomosis between the artery and the artificial blood vessel or autologous vein. The patch material selectively used in patch repair of vascular incisions should have a length greater than the length of the arterial incision; after the patch operation is completed, the diameter of the vessel lumen after repair should be basically the same with that of the normal vessel lumen, thus ensuring the normal endovascular blood flow, while avoid forming the aneurysmal dilatation.
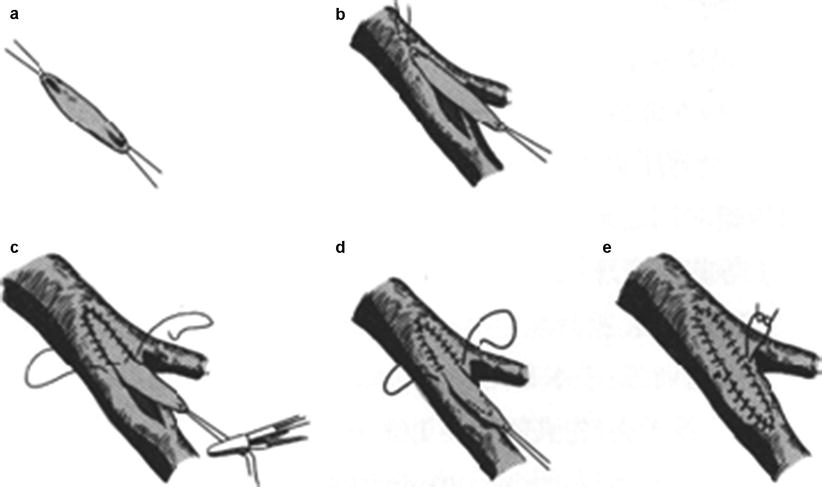
Fig. 21.5
Patch repair of vascular incisions. (a) Vascular patch preparation. (b) Incision. (c) Anchoring. (d) Suturing. (e) Completion
- (1)
3 Clinical Application of Vascular Surgical Techniques
The surgical resection of the tumor involves the different parts of the body, including resections of various tumors in the head and neck, chest, abdominal and retroperitoneal area as well as limbs, and so on and so forth; of which, the surgical treatment of head and neck malignant tumors involving the carotid artery is a very typical part, and the surgery is complex, and the difficulty is greater. This section focuses on the surgical treatment of head and neck tumors involving the major blood vessels to explore the application of vascular surgical techniques in surgical resection of the tumor.
3.1 Application in Head and Neck Oncological Surgery
The head and neck malignant tumors involving carotid artery have always been a thorny problem, which had been a bottleneck limiting the treatment level of the head and neck surgery. The head and neck malignant tumors which have developed into the advanced stage often involve the carotid artery or the internal carotid artery; in order to radically treat the tumor, the treatment of the tumor body and the affected carotid artery has become the key to the treatment. Previously, the tumor is stripped off simply from the arterial wall in clinic, but the safety of the incisal margin is not high, 42% of the results of pathological microscopy show that the artery wall is infiltrated by the tumor, the postoperative local recurrence rate is as high as 50%, and thus the purpose of radically treating the tumor cannot be achieved, and the arterial wall also has the risk of rupture bleeding; if the tumor and the affected carotid artery are ligated and resected, the problems required to be faced include the neurological complications and a higher mortality (the mortality rate of the patients undergoing emergency ligation is 50%). For this reason, the resection of the tumor body and carotid artery combined with the carotid artery reconstruction can eliminate the bottleneck limiting the improvement of treatment level of the head and neck surgery, and reduce the neurological complications and mortality rates, and increase the chance of patients receiving treatment.
3.1.1 The Resection and Reconstruction of the Carotid Artery
Due to the special nature of the carotid artery, when the tumor involving the carotid artery must be removed, under normal circumstances, it is advocated to carry out one-stage reconstruction. While, when the blood vessels are involved, the carotid artery has been compressed for some time; therefore, it itself has a certain anti-ischemic ability.
The basic method for preoperative assessment of resection and reconstruction: The carotid artery reconstruction often requires temporary occluding of the unilateral carotid artery, while the nonselective carotid artery occlusion can have 30–54% stroke rate. Therefore, the preoperative examination and evaluation of the vascular resistance have great significance for the establishment and decision of the operative plan.
Get Clinical Tree app for offline access

- (1)
Carotid artery compression test:
- 1)
Matas test: As early as in 1911, Matas introduced the method that the common carotid artery is compressed externally to detect the tolerance of the carotid artery. The method is that the proximal end of the common carotid artery is compressed daily; the blocking time is gradually increased; when the blocking time reaches more than 30 min every time, there is no occurrence of symptoms of cerebral ischemia such as dizziness, which indicates that the collateral circulation of the brain has been established; the common carotid artery can be resected more safely. This method is simple and easy, but the arterial blood flow cannot be completely blocked through compressing the carotid artery externally using the fingers; the location of compression is inaccurate, the efficacy is poor, and the giant neck tumors and the history of previous surgery and radiotherapy make the local tissue have hard texture and severe adhesion, and thus the test is difficult to carry out. It is reported that Matas test is prone to causing the shedding of the small emboli in carotid plaque and the ischemic brain injury induced by reactive hypotension and bradycardia, and thus it has been rarely used in clinical practice.
- 2)
In vitro training of carotid artery compression device: The carotid artery compression device developed by Li Shuliang et al. has advantages that the effect in blocking the blood flow is definite and the patient has no pain. During training, the compression time is gradually extended to 30–40 min every time; the condition is qualified if the compression training is carried out for more than 20 consecutive days; there are no clinical manifestations such as dizziness, fainting, nausea, vomiting, and limb numbness, and the blood pressure is constant. However, due to longer compression training, the timing of treatment may be delayed or the good opportunity for surgical treatment may be missed.
- 3)
In vivo compression training of the carotid artery: Through the surgical exposure of the common carotid artery, Poppen clip is used as the training device for clipping the carotid artery in vivo. The carotid artery in proximal tumor is placed within the clip; firstly, one third of the vascular diameter is clipped and closed, and then the carotid artery is completely occluded within the following 6–7 days. The observational indexes are the same as those of in vivo compression training of the carotid artery. The carotid artery is clipped for 30–40 min every time; the condition is qualified if there are no symptoms of cerebral hypoxia for continuous 24–48 h. The in vivo compression is sustained and gradually increased, the pressure is constant and reliable, and the training time is short, but it requires surgical incision and may have the risk of infection, and its clinical application is subjected to certain limitations. And the vascular clips are exposed outside the skin; after the arterial wall is clipped close, the blood vessel becomes very thin, and it is very easy to be damaged by external forces to cause large bleeding.
The later both carotid artery compressions also have disadvantages that they are prone to causing the shedding of the small emboli in carotid plaque and the ischemic brain injury induced by reactive hypotension and bradycardia.
- 1)
- (2)
Balloon test occlusion: The balloon test occlusion (BTO) is currently the standard method to evaluate the cerebral ischemia tolerance, through intravascular occlusion of carotid artery system (the internal carotid artery or the common carotid artery) for a short time (15–30 min). Without clinical symptoms or signs, the patient can tolerate carotid artery removal or occlusion permanently. Otherwise, the patient must have the reconstruction of the carotid artery. The permanent internal carotid artery occlusion is carried out in three steps: the diagnostic angiography of carotid artery system and vertebral artery system, temporary occlusion of the internal carotid artery, and the permanent occlusion of the internal carotid artery. The diagnostic angiography can be carried out to learn the collateral circulation situation of the intracranial blood vessels and whether the atherosclerotic lesions or anatomical abnormalities occur concurrently. When the balloon, which is placed at the first and second cervical vertebral levels, is filled fully and the internal carotid artery is completely occluded and is maintained for 15–30 min successfully, the electroencephalogram and the neurological symptoms and signs should be monitored in the process. After the patients can tolerate temporary occlusion, two balloons are placed, respectively, in the carotid siphon to permanently occlude the internal carotid artery, and the angiography is carried out again to determine the location of the balloons, and the postoperative close monitoring should be maintained for at least 12 h.
The complication rate of the balloon test occlusion is similar to that of the conventional intervention operation. The method improves the accuracy of the assessment of the tolerability to the resection of the carotid artery, but 5–20% patients who even have tolerated the method still have cardiovascular complications after the carotid artery is permanently occluded. This may be related to the decreased blood perfusion and slowed blood flow as a result of the carotid artery occlusion. On the basis of this method, the methods such as Doppler ultrasonic measurement of the blood flow velocity of the cerebral artery and cerebral perfusion imaging and the measurement of the carotid reflux pressure are combined, and the comprehensive judgment is conducive to the preoperative evaluation.
- (3)
Doppler ultrasound study of cerebral blood flow (CBF) velocity: The Doppler ultrasound is used to measure the blood flow velocity of the middle cerebral artery after the common carotid artery, or the internal carotid artery is occluded to learn the compensatory situation of cerebral blood flow after occlusion. It is generally believed that the average flow velocity of the middle cerebral artery (the average value of the systolic and diastolic blood flow velocities) or pulse index (the ratio of the difference between the average value of the systolic and diastolic blood flow velocities to the mean blood flow velocity) is reduced by less than 30%, which indicates good compensation; and if it is reduced by 50–60%, which indicates poor compensation, this is prone to occurrence of neurological complications, and the arterial bypass should be established before they are permanently occluded [2, 3].
Although BTO combined with ultrasonic Doppler method is convenient, this method has large individual differences. The in vitro ultrasonic positioning is imprecise, which has a larger relationship with the experience of the operator. Those measured by this method are hemodynamic parameters, which cannot truly reflect the functional state of the brain cells.
- (4)
Cerebral blood flow perfusion imaging: The normal cerebral blood flow (CBF) is about 50–55 ml/min per 100 g brain tissue; when the CBF is reduced to as low as 20–30 ml/min, the patient will have neurological symptoms. The brain CBF is less than 30 ml/min during BTO, which is correlated with the incidence rate of cerebrovascular complications; the patients with brain CBF less than this value have cumulative incidence rate of 30% in 1 month and up to 50% in a year after the internal carotid artery is permanently occluded.
- 1)
SPECT cerebral blood flow perfusion imaging: After the radionuclide-labeled drugs which can emit the low-energy γ photons are introduced into the human body, the SPECT imaging can collect the low-energy γ photons emitted from different organs using SPECT probe and carry out the imaging processing. Because the quantity of the labeled drugs entering into brain cells is positively correlated with the local blood flow, the computer technology and physiological mathematical model can be used to calculate the local cerebral blood flow and the average whole-brain blood flow. Because the radionuclide-labeled drugs are combined with the brain tissue for a long time, SPECT examination can be carried out after the balloon is taken out.
- 2)
PET cerebral blood flow perfusion imaging: After the positron-labeled tracers are introduced to the human body, they aggregate into the organs and emit a pair of high-energy γ photons showing an angle of 180° (511 keV) in the process of positron annihilation, which are collected by PET annular probe, and then imaging is developed after computer reconstruction. The commonly used radionuclides include 15O, 11C, 13N, and 18F. When the brain perfusion imaging is carried out, in the same way as SPECT, PET-CT uses the measured results to calculate the cerebral blood flow volume and estimate the state of the brain function according to the data model. Brunberg et al. drew a conclusion from the [15O]H2OPET cerebral blood flow volume measured by BTO in 22 patients with aneurysms: PET can quantize the cerebral blood flow volume and can effectively predict the tolerance to the arterial occlusion, while Chazono et al. [4] drew the opposite conclusion through research. Therefore, a multicenter clinical study is also needed further.
- 1)
- (5)
The monitoring of reflux pressure of the internal carotid artery: this method is used to measure the reflux pressure of distal segment of the common carotid artery after occlusion to understand the brain blood supply. Hays set 6.67 kPa (50mraHg) as safe pressure, 73 patients with less than 6.67 kPa underwent surgery after occlusion of the carotid artery under the condition that the bypass surgery was not performed, and 50% of patients had cerebrovascular complications. According to experiences of McCoy et al., after the common carotid artery is occluded, when the arterial blood pressure is reduced by less than 20%, the common carotid artery can be safely occluded. According to the experience of Ehrnefeld, the systolic blood pressure of the artery stump more than 9.33 kPa (70 mmHg) is the safe pressure; if the systolic blood pressure of the artery stump is lower than 7.33 kPa (55 mmHg), the cerebrovascular complications will occur. Since various hospitals adopt different standards, and the surgical methods are different, currently it is difficult to develop uniform standards.
- (6)
Monitoring of jugular venous oxygen saturation: The internal jugular vein blood comes directly from the cerebral vein; thus the jugular venous oxygen saturation (SjvO2) is used to replace the cerebral venous oxygen saturation. Under the condition that the SO2 and Hb are stable, SjvO2 can reflect the supply and demand condition of cerebral oxygen, and any factors increasing the cerebral oxygen consumption and (or) reducing the cerebral oxygen supply can lead to reduced SO2. The normal SjvO2 is 54–75%; when it is greater than 75%, it is indicated that the cerebral oxygen supply or the cerebral blood flow volume is increased; when it is less than 50%, it is indicated that the cerebral oxygen supply or the cerebral blood flow volume is relatively reduced, and the demand of cerebral oxygen metabolism cannot be met; if it is less than 40%, there may exist whole-brain ischemia and hypoxia, and the causes should be found and corrected. But the correctness of the measured value of SjvO2 is affected by the following factors:
- 1)
Either the left or right internal jugular vein blood is not entirely true cerebral venous blood, which is often mixed with 3–7% extracranial blood.
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Tissue Engineering and Oncological Surgery
Tissue Engineering and Oncological Surgery
 Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


- 1)