16 Anthropometry, cephalometry, and orthognathic surgery
Synopsis






Anthropometrics
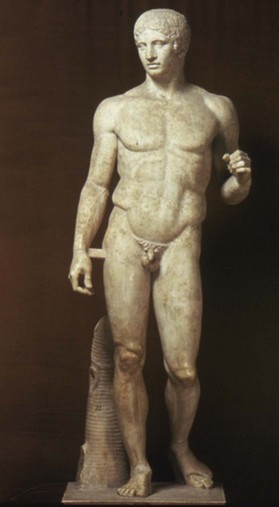
Anthropometry involves the study of the human body in relation to its variations in size and proportions. The use of well-established aesthetic standards allows facial, craniofacial, and maxillofacial surgical techniques to achieve cosmetic results.1 Throughout history, there has been a fascination with the human form. While the ancient Egyptians are reported to have been the first to divide the human body into equal parts, the Greek sculptor Polycleitus is credited with the development of canons as exemplified in his statue of Doryphorus (Fig. 16.1).2 During the Renaissance, artists such as da Vinci, Dürer, Pacioli, and Alberti developed the Neoclassical Canons, which divided the face into symmetric ideal proportions. The 18th and 19th centuries brought the concept of physical anthropology, in which the majority of measurements were performed directly on skulls with less attention given to soft tissue points. Camper introduced the concept of the facial angle and used this measurement to challenge the hypothesis of an evolutionary basis to racial inequality.3 Later anatomists, however, such as De Gobineau, Broca, Topinard, and Lombroso, accepted variations in skull proportions as evidence of inferiority of all non-white individuals.4–6 The 20th century was highlighted by the development of radiographic techniques to indirectly measure the facial skeleton. Broadbent’s concept of cephalometrics7 allowed the initial compilation of normative facial data in 5400 children over 36 years as part of the Bolton study.8,9
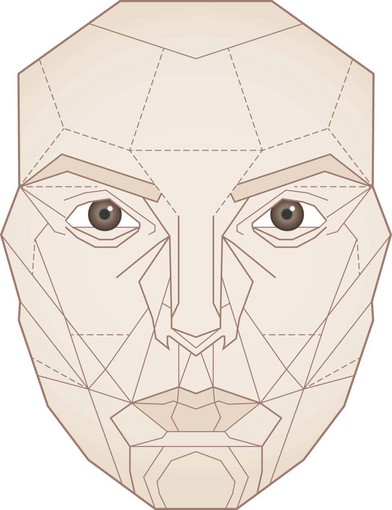
The idea of the “golden proportion” having application to facial analysis, although introduced by Seghers et al.,10 was popularized by Ricketts.11–14 The aesthetically attractive 1 : 1.618 ratio, indicated by the Greek letter phi (Φ), was first recorded in the 3rd century bc by the Pythagoreans and has applications dating back to the architecture of the Egyptians.1 Ricketts’ use of the golden divider caliper to demonstrate, e.g., the relationship between the width of the nose to mouth or the height of pupils to nasal alae and alae to chin has allowed application of the golden proportion to preoperative planning.15 Marquardt has attempted to further objectify the concept of an aesthetic face with his development of the golden ratio phi mask (Fig. 16.2). Although the validity of this concept has been supported by superimposing the mask on young, white individuals of European descent,16 there are many limitations, as Guyuron points out,17 in the use of two-dimensional photographs to define an attractive face.
Modern-day anthropometrics has been perhaps led by the work of Leslie Farkas. He has defined and measured countless soft tissue points and dimensions in hundreds of people of varying ethnicities and ages.18,19 His extensive work has allowed the development of a database of normative values to which subsequent facial analyses may be compared. Perhaps of equal importance, Farkas has realized the limited application of the neoclassical canons and the golden ratio to only a select group of patients.20,21
With the development of three-dimensional scanning systems, a new layer of complexity has been added to facial analysis. Data points can be obtained from a variety of different technologies, including computed tomography (CT); magnetic resonance imaging (MRI); ultrasonography;22 facial morphometry;23 3-D video imaging system;24 moiré-stripe photography;25 liquid crystal range finder system;26 surface scanner system, and stereophotogrammetry. The accuracy of these techniques has been tested and appears to correlate well with direct measurements. The clinical application of these systems allows not only a detailed facial analysis by the physician, but also a more realistic and conceptually tangible postoperative result for the patient.
Facial analysis
The standardization of soft tissue facial analysis and the application of the neoclassical canons relies on consistent facial landmarks (Table 16.1, Box 16.1). By use of the classic two-dimensional photograph, facial proportions can be examined both vertically and horizontally.
Table 16.1 Soft tissue landmarks
| Vertex (v) | The highest seen point on the head with the head in Frankfort horizontal |
| Trichion (tr) | The junction of the hairline and the forehead in the midline |
| Glabella (g) | The most prominent point of the forehead in the midline between the eyebrows |
| Nasion (n) | The midline point of the junction of the frontonasal suture and the superior nasal bones. Externally, nasion often corresponds to the point of greatest concavity of the nasal dorsum near a line level with the upper lid lash line |
| Orbitale (or) | The palpable point of the lowest margin of the inferior orbital rim |
| Porion (po) | The most superior point of the external auditory meatus |
| Frankfort horizontal (FH) | The line connecting porion and orbitale. This line is parallel to the floor for anthropometric measurements. It is an approximation of neutral head position in straight gaze |
| Endocanthion (en) | The point of the medial canthus where the upper and lower lids join |
| Pronasale (prn) | The most prominent point of the nasal tip |
| Subnasale (sn) | The deepest point at the junction of the base of the columella and the upper lip in the midline |
| Stomion (sto) | The midline point where the upper lip touches the lower lip |
| Sublabial (sl) | The midline point at the junction of the lower border of the cutaneous lower lip and the superior border of the chin. It is the deepest point of the labiomental groove |
| Pogonion (pg) | The most prominent point of the chin in the midline |
| Gnathion (gn) | The most inferior point of the lower border of the mandible; also called menton (me). In cephalometric analysis, gnathion and menton are two different points on the mandible |
Box 16.1
Neoclassical canons
• The height of vertex to endocanthion is equal to the height of endocanthion to gnathion (two-section canon).
• The heights of trichion to nasion, nasion to subnasale, and subnasale to gnathion are equal (three-section canon).
• The heights of vertex to trichion, trichion to glabella, glabella to subnasale, and subnasale to gnathion are equal (four-section canon).
• The width of the alae equals one-fourth the width of the distance between the zygomas (nasofacial proportion canon).
• The length of the nose is equal to the height of the ear (nasoaural proportion canon).
• The inclination of the nasal dorsum is equal to the inclination of the ear (nasoaural inclination canon).
• The distance between the medial canthi is equal to the width of the eye fissure (medial to lateral canthus of the eye) (orbital proportion canon).
• The distance between the medial canthi equals the width of the ala (orbitonasal proportion canon).
• The width of the mouth equals  the width of the ala (naso-oral proportion canon).
the width of the ala (naso-oral proportion canon).
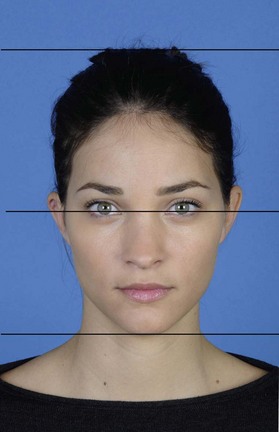
The initial proportional analysis of the face begins with the division into halves, with the height of the vertex to endocanthion being equal to the endocanthion to gnathion height (Fig. 16.3). Perhaps one of the most utilized canons is the division into thirds (Fig. 16.4). The distance from the trichion to the glabella equals the distance from the glabella to subnasale, which equals the subnasale to gnathion distance. Obviously, a limitation of this technique is the position of the hairline which may change with age, most notably in the male patient. When examining the lower third, it can be further divided into thirds such that the distance from the subnasale to the stomion is one-third and the distance from the stomion to gnathion is two-thirds (Fig. 16.5). The four section canon states that the distances from vertex to trichion, trichion to glabella, glabella to subnasale, and subnasale to gnathion are all equal (Fig. 16.6). Farkas examined the reliability of these relationships and found that a majority of patients deviate from these proportions.20 The upper half of the face, especially in women is actually greater than the lower half, and the height of the nose is typically less than the upper and lower thirds. Men typically have a larger lower third due to a more prominent mandible while women tend to have more equal lower and middle thirds. Further consideration must be given to proportional variations due to ethnicity, and these differences must be respected when considering surgical changes. Further division of the face into five major aesthetic masses27 (forehead, eyes, nose, lips, and chin) allows a more detailed analysis.


Forehead
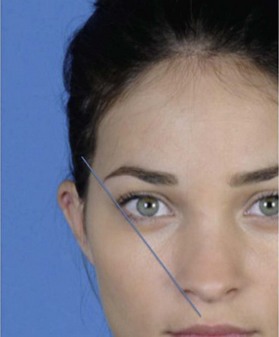
The aesthetic forehead has a slight convexity to it, with the apex lying just above the nasion. The nasofrontal angle is formed between the inferior forehead and the nasal dorsum (Fig. 16.7). In an aesthetic profile, this angle is between 125° and 135°. The forehead is the most stable unit of the face and small changes in its prominence at the supraorbital ridges can have dramatic effects on nasal length and projection. The nasal radix depth should be tangent to the fronto-subnasal line.28 The eyebrows should lie just above the supraorbital rim in women and have the apex of their arch above the lateral limbus. An important aesthetic feature is the lateral brow in women, which should be more elevated (Figs 16.8, 16.9). In men, the eyebrows are less arched and should lie at the level of the supraorbital rim. (Eyebrow aesthetics are thoroughly reviewed in Chapter 7.)


Eyes
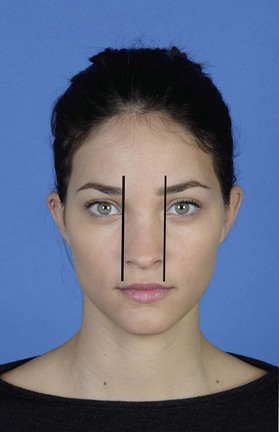
The shape, color, and cant of the eyes, as well as the quality of the eyelids are very important components of facial aesthetics (aesthetic issues are reviewed in Chapter 6). The width of the eye from medial to lateral canthus should equal the distance between the medial canthi. This distance is typically one-fifth of the width of the face with the most lateral fifths lying between the lateral canthus and helix (Fig. 16.10). The distance from the lid margin to the supratarsal crease, which changes with ethnicity, varies between 7 and 15 mm. The upper lid should cover 1–2 mm of the superior limbus, while the lower eyelid should be at the level of the inferior limbus. A vertical line through the medial limbus should intersect with the oral commissure.

Nose
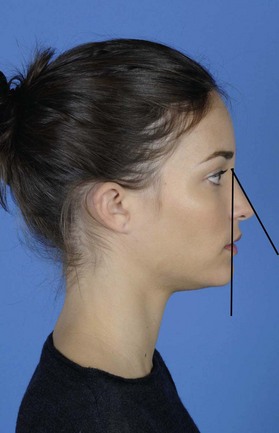
As the central and most prominent unit of the face, the nose plays a major role in facial aesthetics. Although nasal anatomy and nasal aesthetics are reviewed in Chapter 17, a few basic relationships will be discussed here. The nasofacial angle is formed by the nasal dorsum and the facial plane (defined by a line drawn from the glabella to pogonion), and ranges from 35° to 40° (Fig. 16.11). The nasolabial angle formed between the columella and upper lip is between 100–103° in men and 105–108° in women (Fig. 16.12). This angle is a very important component of nasal aesthetics and may be affected dramatically with changes in tip rotation or projection.

Tip projection is closely related to the nasofacial angle and can be measured in many ways. In Chapter 17, tip projection is defined as the distance from the alar base to the nasal tip; ideally 50–60% of the projection will lie anterior to a vertical line drawn over the most projecting part of the upper lip. The Byrd method suggests that tip projection should be 0.67 of nasal length. In the Goode method, a vertical line is drawn from nasion to the alar groove. The horizontal distance from ala to tip is then measured and a ratio of ala-tip : nasion-tip is typically 0.55–0.60, corresponding with a nasofacial angle of approximately 36°. The Baum method uses the nasofrontal angle as the vertical axis. A line is drawn from the nasofrontal angle vertex to the subnasale. A perpendicular horizontal line drawn to the tip should give a ratio of dorsum : tip of 2 : 1, which corresponds to a nasofacial angle of 42°. Powell27 suggests modifying this ratio to 2.8 : 1 to produce a nasofacial angle of 36°. The Simons method relates tip projection to upper lip length. The distance from the skin-vermilion junction to the base of the columella should equal the distance from the subnasale to the tip.
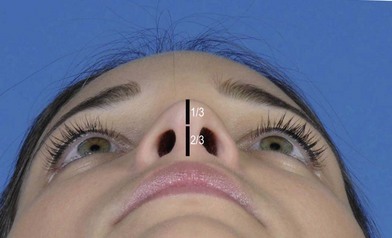
The ideal width of the nose at base from ala to ala should equal the intercanthal distance (Fig. 16.13).29 The nasal width : length ratio (from nasion to tip) should be approximately 0.7.30 On basilar view, the nostrils comprise two-thirds the length of the columella and the tip occupies the remaining one-third (Fig. 16.14).
Lips
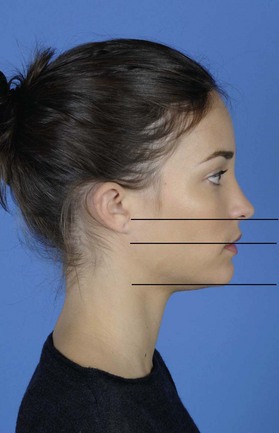
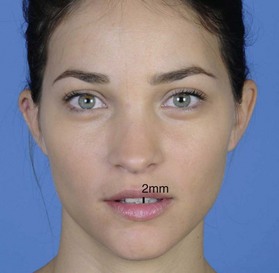
The upper lip extends from subnasale to stomion, while the lower lip and chin are measured from stomion to gnathion. The ratio of these distances should be 1 : 2. The ideal width of the oral commissure should be defined by a vertical line drawn from the medial limbus (Fig. 16.15). On lateral view, the lip protrusion can be measured as the perpendicular horizontal distance from a vertical line drawn from subnasale to pogonion. The upper lip typically lies 3.5 mm from this line and should protrude over the lower lip, which typically lies 2.2 mm anterior to the line.31 The underlying dentition has a profound impact on the fullness of the lips. In repose, the amount of maxillary incisal show should be 2 mm (Fig. 16.16). In a full smile, approximately two-thirds of the crown should show. This relationship is obviously impacted significantly by surgical changes in maxillary vertical position, which will be discussed later in this chapter.
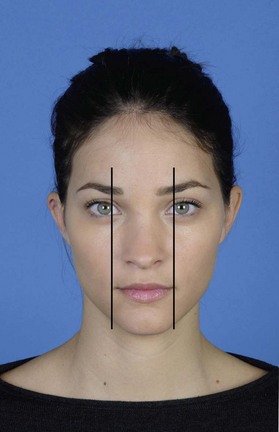
Fig. 16.15 The width of the oral commissure should be defined by a vertical line drawn from the medial limbus.
Chin
The mentocervical angle (Fig. 16.17) is measured by a vertical line drawn from the glabella to the pogonion and a horizontal line drawn from the gnathion to the cervical point (intersection of the neck and submental areas). This value ranges from 80–95° and is affected by both the position of the chin and the overlying soft tissue of the chin and neck. A more acute mentocervical angle gives a more pronounced, aesthetic jaw line (Table 16.1, Box 16.1).
Cephalometrics
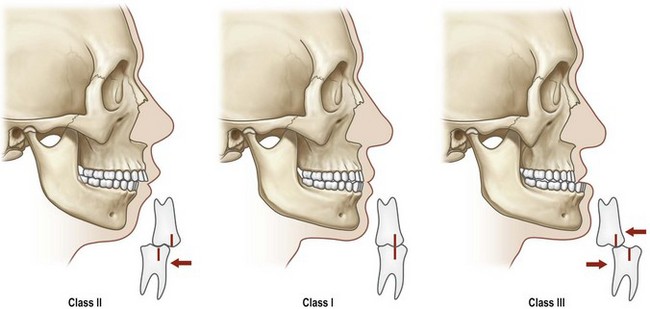
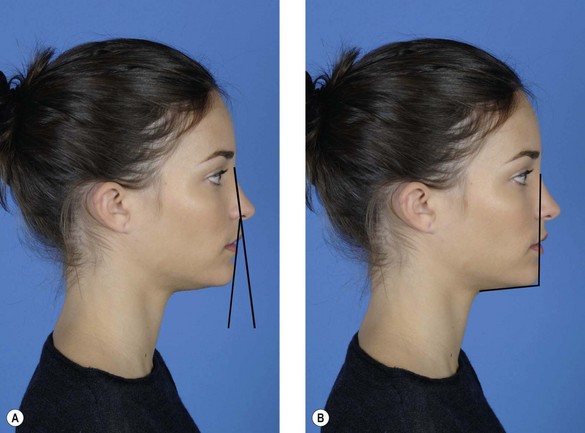
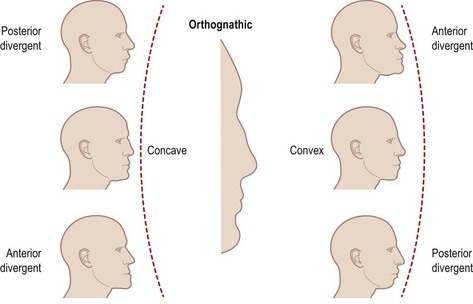
A convex facial profile can result from an over-projecting maxilla or a mandible positioned too far posteriorly. A concave facial profile can result from a maxilla being too far posterior or a mandible that protrudes forward (Fig. 16.18).
The relationship between the maxillary and mandibular dentition and occlusion was classically defined by Angle in 1899.32 He described the position of the maxillary and mandibular first molar teeth to each other as follows:
• Class I: normal relationship of the mesial buccal cusp of the maxillary first molar fits the buccal groove of the first mandibular molar (orthognathic)
• Class II: mandibular molar posteriorly positioned relative to the upper first molar (retrognathic)
• Class III: mandibular molar anteriorly positioned relative to the upper first molar (prognathic).
The correction of the first molar position is an important guide to achieve class I jaw and dentition relationships (Fig. 16.19).