Anatomical Subunit Repair of Unilateral Cleft Lip
David K. Chong
Kathryn V. Isaac
DEFINITION
Cleft lip is a congenital malformation in embryonic development leading to discontinuity of the upper lip. The cleft may be:
Complete or incomplete
Bilateral or unilateral
Cleft lip may occur in isolation or in combination with a cleft palate. It may occur as part of a syndrome or in the absence of associated anomalies.
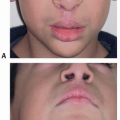
A cleft lip has an associated cleft nasal deformity with characteristic features varying in severity depending on the type of cleft lip, width of the cleft, and presence of associated cleft palate.
The cleft lip nasal deformity affects the skeletal, cartilaginous, and muscular framework.
ANATOMY
During the 5th to 7th weeks of gestation, cleft lip occurs as a failure of complete union of the medial nasal process and the maxillary prominence.
Clefting occurs through the skin, muscle, and mucosa of the labial and nasal structures.
The cleft of the lip distorts and/or disrupts several important anatomic structures.
Muscles
Orbicularis oris (pars marginalis and pars peripheralis)
Pars alaris, depressor alae nasi
Upper lip
Cutaneous lip: philtral columns, central dimple, cutaneous roll
Red lip: Cupid’s bow, vermillion, mucosa
Nose
Nasal floor, alar base, nasal cartilages, septum, columella
PATHOGENESIS
The etiology of cleft lip is genetically complex and is due to multiple genetic and environmental risk factors.
Most cases are sporadic, but some are familial, X-linked, or autosomal dominant. Familial history of clefting is an important risk factor.
Cleft lip and cleft lip with cleft palate are considered variants of an entity that differ in severity.
The environmental risk factors associated with clefting include maternal smoking, infection, poor nutrition, teratogen exposure (alcohol, phenytoin, valproic acid, retinoic acid), and advanced paternal age.
PATIENT HISTORY AND PHYSICAL FINDINGS
Diagnosis of a cleft lip is made by prenatal ultrasonography, by MRI, or by physical examination at birth. Detailed assessment is made of the child’s breathing, feeding, growth, and development.
Assessment of growth and weight is key to identify and monitor feeding difficulty and use of feeding aids (Haberman/Pigeon teat).
The plastic surgeon should define the cleft lip type according to the anatomic structures involved, laterality, width of the cleft, and presence/absence of a cleft palate.
Also, the child should be assessed for associated anomalies suggestive of a syndrome—craniofacial dysmorphism, airway compromise, cardiac defects, ocular and auricular abnormalities, and musculoskeletal anomalies. A genetics referral is suggested if suspicious of a syndromic etiology.
DIFFERENTIAL DIAGNOSIS
Syndromic cleft lip with or without cleft palate
Van der Woude syndrome
Gorlin syndrome
CHARGE syndrome
Ectrodactyly-ectodermal dysplasia-clefting
Brachio-oculofacial syndrome
Kabuki syndrome
Kallmann syndrome
SURGICAL MANAGEMENT
Cleft lip repair is ideally performed at age 6 months because the landmarks are larger and easier to identify.
The principles of the anatomical subunit repair enable the surgeon to formulate a plan for the predictable and successful closure of any type of cleft lip.1
The labial cleft closure is designed, measured, and determined prior to skin incision. The operation is the execution of a formulated plan. This eliminates the potential of compromising landmarks and removes the fear of underrotation, as well as lip height or length discrepancies.
With this repair, the most visible part of the scar lies along the anatomical subunits, and the labial elements are perfectly matched in length to create an optimal continuity of vermilion, cutaneous lip, and alar-labial junction.
Rotation of the labial elements is achieved by:
Skin triangle above the cutaneous roll
Muscle repair
Mucosal release
Risks of the procedure are scar deformity, nasolabial asymmetry and/or deformity, wound dehiscence, and infection.
The main objectives of the cleft lip repair are to (1) separate the nasal and oral cavities; (2) restore lip continuity and continence; (3) reconstruct a functional labial sphincter for facial expression, speech, and feeding; (4) and restore aesthetics of the labial and nasal subunits.
The main steps of the procedures are as follows:
Marking key landmarks and designing closure of labial elements based on pre-incision measurements
Medial lip element release of skin, muscle, and mucosa to adequately balance the Cupid’s bow, then composite elevation of lateral lip elements to insert into the created “jigsaw”
Restoration of muscle continuity
Closure of the mucosa
Closure of the nasal floor
Skin and vermilion closure
Nasal correction with suture techniques
In discussing this repair, the language used in Millard’s description of the rotation-advancement cleft lip repair will be used.2 The application of this language will help to clarify and describe this technique for surgeons who have adopted the Millard technique or modifications of it.
Preoperative Planning
If the child has a cleft lip and cleft palate, dentofacial orthopedics are utilized for aligning the cleft maxillary arches and improving the nasal deformity (lower lateral cartilage shape and position and septal cartilage alignment). The device is discontinued prior to the cleft lip repair.
Positioning
The patient is positioned supine with the neck neutral and head stabilized in a head ring.
The surgeon must have the ability to freely examine the face from all angles throughout the procedure to ensure that three-dimensional balance is achieved. Corneas are protected with transparent tape to use the plane and position of the eyes in the surgical field as an aid to assessing labial and nasal symmetry. The transparent tape should still allow the cheek to move freely.
Loupe magnification is helpful for accurate identification of anatomical landmarks, for precise tissue dissection, and for perfect approximation.
Approach
Successful application of this cleft lip repair is facilitated by highlighting conceptual differences between the rotationadvancement repair and anatomic subunit repair.
Important landmarks are marked out, never compromised, and incisions are made for closure that follows anatomical subunits.
Paradigm shift: Spend more time marking before any incisions are made and the surgeon is committed to the plan.
Calipers are used to measure incisions for perfect length match.
Paradigm shift: The artistic “eye” is supplemented by precise measurements.
Foundation of repair is in the muscle.
Paradigm shift: Extension of skin incision outside of the proposed philtrum to achieve rotation is not required.
Inferior triangle is placed above the cutaneous roll. This location restores the cutaneous roll without interruption and achieves any additional lip lengthening required for the skin.
Paradigm shift: Triangle is premeasured. Most measure 1 to 2 mm because the muscle repair and mucosal M flap both contribute to lip lengthening.
TECHNIQUES
▪ Planning the Repair: Medial Nasolabial Element
Markings are made with methylene blue dye after the patient is prepped and draped.
Markings of landmarks and anatomic contours are made with dots at the landmarks listed below and along the line of interest for measurement, incision, or alignment of elements.
Tattoo all points to prevent loss of landmarks.
Vermilion, Cupid’s Bow, and Nose
Mark the junction of the vermilion and mucosa along both medial and lateral lip elements (TECH FIG 1A).
This helps determine the vermilion height discrepancy and points of closure and ensures a continuous natural curve is achieved.
The following marks are placed on the medial lip element (TECH FIG 1B):
Mark the peak of Cupid’s bow on the noncleft side with one point above and below the cutaneous roll.
Mark the trough of Cupid’s bow.
Mark the peak of Cupid’s bow on the cleft side with one point above and below the cutaneous roll. The point above the cutaneous roll guides the placement of the opening incision for insertion of the triangular cutaneous flap, if required. Choose this point just medial to the actual peak of the Cupid’s bow because it is difficult to surgically create a curve. It is preferable to use the existing curve on the lateral lip element.
Mark the columellar points: one central and two adjacent that are symmetrically distanced from the center and lie at the superior end of the philtrum.
The noncleft side of the medial lip element will guide you to pick the superior extent of the philtrum, and you can mirror this onto the anticipated created philtrum on the cleft side of the medial lip element (TECH FIG 1C).
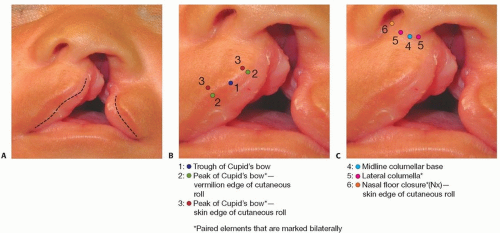
TECH FIG 1 • Medial lip markings. A. Vermilion. The border between the vermilion and the mucosa is marked. B. Cupid’s bow. C. Nose. (Copyright © David Chong.)
Remember that the apparent curve of the noncleft side philtral column is due to the unopposed action of the unrepaired orbicularis oris and is almost always a straight line in the Caucasian population once repaired.
In the noncleft nasal sill, mark the point where the medial footplate of the medial crus meets the nasal floor (Nx). This point is used to guide the nasal sill closure on the cleft side.
Measurements and Interpositional Triangle
Measure the distance on the noncleft side from the superior extent of the philtrum to the peak of Cupid’s bow above the cutaneous roll (TECH FIG 2A).
This is the total height of the philtrum (a) on the noncleft side that you need to recreate on the cleft side philtrum.
Measure the distance on the cleft side from the superior extent of the philtrum to the peak of Cupid’s bow above the cutaneous roll with tissue unfurled to mimic repair (TECH FIG 2B). This is the height of the cleft philtrum (b). It is key to unfurl the convex surface of the medial lip during this measurement; this maneuver aims to mimic the lengthening achieved with muscle dissection and repositioning with mucosal release.
Perform a simple calculation to decide the need for an opening triangle: subtract the distances between the philtrum of the noncleft side and the cleft side (a– b – 1) (TECH FIG 2C).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree