Chapter 40 Anatomical Retroscrew Anterior Cruciate Ligament Fixation
Single- and Double-Bundle Anterior Cruciate Ligament Reconstruction with Retroscrew Biointerference in a Single Femoral Socket
The concept of anatomic graft positioning for anterior cruciate ligament reconstruction (ACL) has been previously described by many authors.1–6 In the past, anatomical graft tunnels were believed to obtain an optimal ACL reconstruction; the position of the graft within bone tunnels had to avoid the intercondylar roof and wall impingement. Studies have documented the landmarks for the placement of endoscopic tunnels in anatomical reconstructions through a full knee range of motion that will avoid impingement.7,8
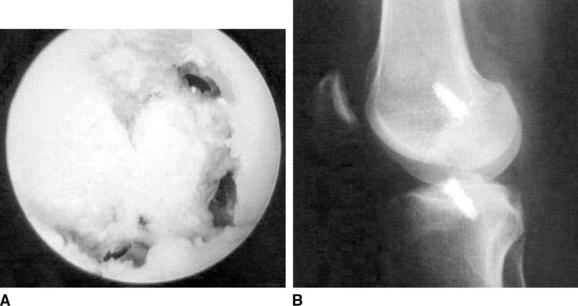
Recently, issues regarding graft fixation position have become important. Experimental and clinical trials have shown that anatomical graft fixation and position at or near the origin and insertion of the native ACL in contrast to nonanatomical fixation position will (1) minimize graft tension, (2) minimize graft length change, (3) produce a more stable reconstruction through full knee range of motion, and (4) avoid anteroposterior, sagittal, windshield wiper–type graft motion.1,2,4,7–10 Five-year follow-up studies comparing anatomical and nonanatomical fixation for ACL reconstruction have shown absence of tunnel expansion up to 5 years with an anatomically fixed graft at the intraarticular tibial tunnel orifice (Fig. 40-1)5,6,8,11,12
The Retroscrew (Arthrex, Naples, FL) (Fig. 40-2) is inserted into the tibial tunnel in an inside-out position so that the head of the screw achieves aperture fixation at the intraarticular tunnel orifice. Standard interference screw fixation is used on the femoral side. The Retroscrew is beneficial during tensioning because unlike an antegrade screw, the Retroscrew will pull the graft tighter into the tunnel, especially during tensioning.
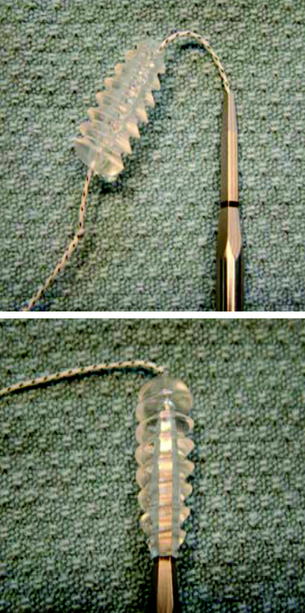
Fig. 40-2 The femoral and tibia Retroscrews are shown. The screws are tethered by a #2 Fiberwire suture.
Morgan et al4 first described an “all-inside” technique for ACL reconstruction that addressed the issues of anatomical fixation. However, the procedure was not popular because of its technically demanding nature3,5,6,13 (Fig. 40-3).

Operative Technique: Single Femoral Socket, Single-Bundle Graft
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


