CHAPTER 41 Anatomic approach for tip problems
History
A successful treatment plan depends on an understanding of the following:
• The anatomic variations of the soft tissues and cartilaginous framework of the tip as well as their contributions to the external nasal appearance.
• The factors that are responsible for the support of the tip and how they are interrelated.
• The effect that each surgical modification or combination of modifications has on the final surgical result.
Anatomy
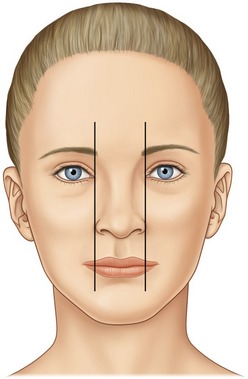
A pleasing appearing nasal tip will usually have the following components. The basal width of the nose should be approximately the same as the intercanthal distance (Fig. 41.1).
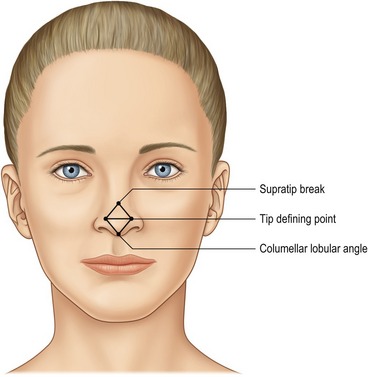
Four landmarks should be highlighted on the frontal view: the supra-tip break, the paired tip defining points and the most inferior portion of the infra-tip lobule. These points should divide the tip complex into two equal and opposite equilateral triangles (Fig. 41.2).
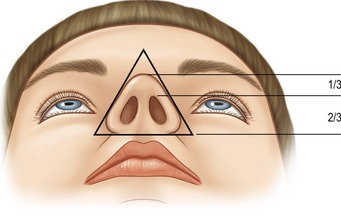
From the basal view, the base should form an equilateral triangle with rounded corners, side walls and a lobule to nostril ratio of 1 : 2. The nostrils are routinely oval in shape with a slight superior-medial orientation (Fig. 41.3).
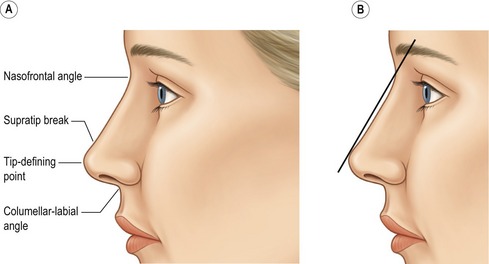
The straight alar side-walls should slope medially upward to the paired tip defining points (TDP). On lateral view, a straight line drawn from the naso-frontal angle to the TDP should be 2–3 mm anterior to the nasal dorsum in females. This should result in a slight supra-tip break. Generally, this is not necessary in males and one should err on the side of a straight nasal dorsum to prevent the nose from appearing feminine (Fig. 41.4).
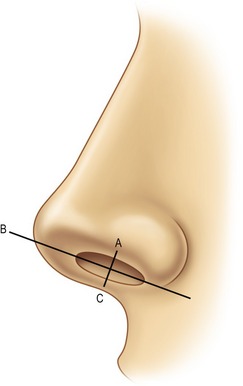
The alar-columellar relationship is measured from the naso-labial angle – which is defined by a line drawn through the most anterior and posterior portion of the nostril on profile. The nostril show should never be less than 1 mm or greater than 4 mm (line A–B and line B–C) (Fig. 41.5).
The nasal tip cartilages are comprised of paired lower lateral cartilage complexes (LLCC) on both sides which connect the lateral ends of the lateral crura to the pyriform aperture by the accessory cartilages. Each LLCC is comprised of a medial and a now named intermediate crus (formerly thought to be the anterior portion of the medial crus) which extends from the columellar-lobular angle to its junction with the lateral crus. The dome of the LLCC, which is typically rounded, is the most projecting part of the tip. The highest point on the dome is termed the tip defining point (TDP) (Fig. 41.6).
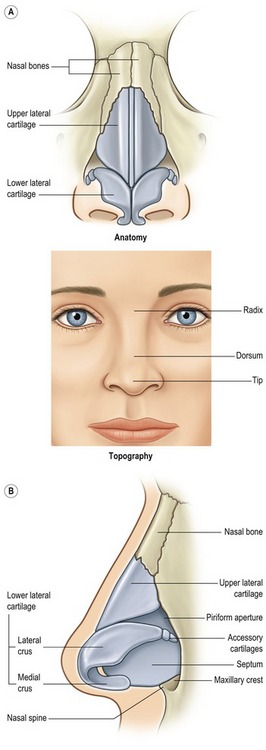
Fig. 41.6 A, It is of critical importance to appreciate the effect the underlying osseocartilaginous framework has on the overlying nasal skin. B, Tip shape results from the combined effect of the paired lower lateral cartilages, upper lateral cartilages caudal septum, septal angle and associated ligaments and skin.
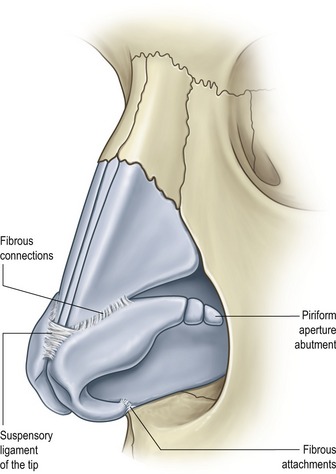
The LLCC are the major supporting factors of the tip. The larger, more rigid they are the more influence they have in this role. The LLCC are in turn supported by three ligamentous attachments to adjacent structures. One attachment is between the feet of the medial crura and the septum, another between the cephalic border of the lateral crus and the caudal border of the adjacent upper lateral cartilage (ULC) and the third from the medial cephalic border of the lateral crus across the septal angle to the medial cephalic border of the opposite lateral crus. Other structures adding to the support are the fibro-fatty tissue between the feet of the medial crura and the anterior maxilla, the septal angle and the tip skin (Fig. 41.7).
The shape of the tip is determined by the LLCC and their supporting structures.
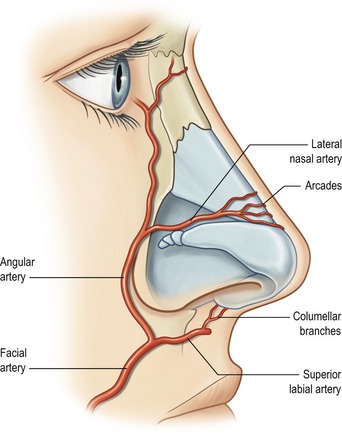
The blood supply to the nasal tip skin is supplied primarily by the angular and superior labial arteries, which derive from the facial artery. The lateral nasal artery originates from the angular artery; it then passes medially along the cephalic margin of the lateral crura and gives off caudal branches toward the nostril rim. The columellar artery takes off from the superior labial artery and courses up the columella to the region between the domes. The lateral nasal and columellar arteries then anastomose over the domal region, forming an alar arcade that runs along the cephalic margin of the lateral crura. The presence and location of these vessels has been shown to be anatomically consistent. Collateral flow may also be provided by the ophthalmic system, but this is less reliable (Fig. 41.8).
Technical steps
Using the open approach with bilateral marginal incisions connected by a staggered transcolumellar incision, the skin is elevated off the underlying cartilaginous and bony framework with sharp pointed scissors and periosteal elevators staying directly against the osseocartilaginous framework. The nose is then inspected to confirm or alter the clinical preoperative analysis (Fig. 41.9).
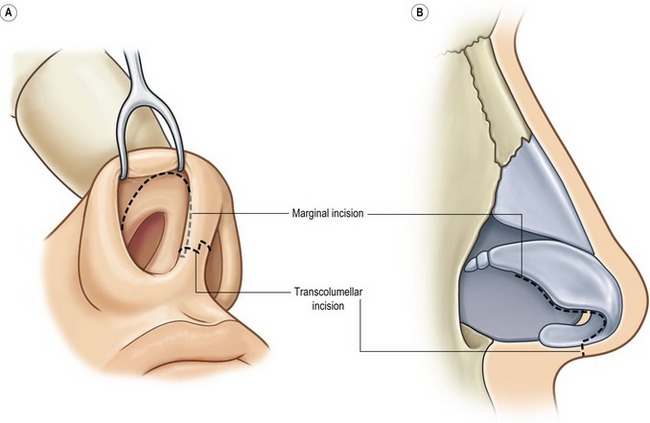
Fig. 41.9 Standard incisions employed in the open approach. (Infracartilaginous incision combined with staggered transcolumellar incision.)









