INTRODUCTION
Already described in Roman times and in the Middle Ages, and rediscovered by the Swiss dermatologist Robert Muller, ambulatory phlebectomy (AP) is a safe and effective surgical technique that enables the removal of incompetent saphenous veins (except the saphenofemoral and in most cases the saphenopopliteal junctions), their major tributaries, perforators, and reticular veins, including the feeding veins of telangiectasias, or even blue telangiectasias. AP may also be used in varicophlebitis and superficial phlebitis, or for veins in other locations, for instance, dilated periorbital, temporal, or frontal venous networks, as well as venous dilatation of the arms, or dorsum of the hands.
AP is indicated in almost all patients, including the elderly. Most of the procedures are performed in truly ambulatory patients, but the technique may also be used in conjunction with other surgical procedures in ambulatory or stationary patients, such as ASVAL (ambulatory selective variceal ablation under local anesthesia).
The goal of AP is to secure definitive treatment of the varicose veins once the underlying cause of reflux has been treated and eliminated. In some cases, the goal may be only partial or short-term improvement. Examples include avulsion of a single painful varicose vein in a young mother unwilling or unable to consider more extensive treatment, or in an elderly patient, removal of a single symptomatic varicose segment or of a feeding vein causing a leg ulcer.
THE PROBLEM BEING TREATED
This chapter will clarify how to select patients who may benefit from AP and how to perform the procedure safely and effectively. However, AP cannot be learned solely from a textbook, and being able to perform the procedure independently requires observing an experienced phlebologist treat different kinds of varicose veins as he or she carefully explains the successive steps of infusing anesthesia, operating, and bandaging.
Every patient should be carefully interviewed and examined, including duplex ultrasound (DUS), before selection of the most appropriate procedure ( Box 10.1 ). Side-transillumination (episcopy) is a useful tool for detecting reticular varicose veins and feeding veins associated with overlying telangiectasias.
Box 10.1
Diagnostic Methods
-
•
Patient interview
-
•
Clinical examination while the patient is in the supine position
-
•
Episcopy (side-transillumination)
-
•
Duplex ultrasonography
PATIENT SELECTION
Patients of all ages may be treated with AP. All types of primary or secondary varicose veins (saphenous, reticular, perineal, telangiectatic, veins, and perforators corresponding to classes C1–C6 of the clinical, etiologic, anatomic, pathophysiologic classification [CEAP]) may be removed by AP ( Boxes 10.2–10.4 ; Figs. 10.1–10.3 ). Further special indications are discussed at the end of this chapter.
Box 10.2
C classes in CEAP (2020)
Each clinical class is further characterized by a subscript for the presence of symptoms (S = symptomatic) or absence of symptoms (A = asymptomatic). Symptoms include aching, pain, tightness, skin irritation, heaviness, muscle cramps, and other complaints attributable to venous dysfunction. (Adapted from Lurie F et al 2020. The 2020 update of the CEAP classification system and reporting standards. Journal of Vascular Surgery: Venous and Lymphatic Disorders 8(3):342–352.)
-
C 0 No visible or palpable signs of venous disease
-
C 1 Telangiectasias or reticular veins
-
C 2 Varicose veins
-
C 2r Recurrent varicose veins
-
C 3 Edema
-
C 4 Changes in skin and subcutaneous tissue secondary to CVD
-
C 4a Pigmentation or eczema
-
C 4b Lipodermatosclerosis or atrophie blanche
-
C 4c Corona phlebectatica
-
C 5 Healed venous ulcer
-
C 6 Active venous ulcer
-
C 6r Recurrent active venous ulcer
Box 10.3
Indications for Ambulatory Phlebectomy
-
•
Saphenous and saphenous tributaries
-
•
Varicose veins of the lateral aspects of the leg
-
•
Reticular varicose veins
-
•
Perineal varicose veins
-
•
Veins of the dorsal aspect of the foot
-
•
Varicose pearls
-
•
Perforators (with some limits)
Phlebectomy of an isolated portion of a saphenous vein should not be conducted if the termination is insufficient. Phlebectomy of the perforators is to be envisaged with caution. The results are good if the hook is used to remove the medial perforators of the thigh and small perforators of the lateral surface of the legs. The results are mediocre with respect to the medial perforators of the lower leg.
Other Indications
-
•
Curettage of telangiectasias
Other Esthetic Indications
-
•
Facial, palpebral and arm veins, etc.
Box 10.4
Principal Indications of Sclerotherapy and Ambulatory Phlebectomy (AP)
-
•
Sclerotherapy: telangiectasias and reticular varicose veins
-
•
Ultrasound-guided sclerotherapy: intrafascial varicose networks, including the small saphenous veins
-
•
AP: from reticular to large, epifascial varicose veins
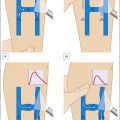
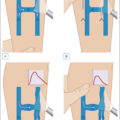
(A) Pretibial varicose veins (C2). (B) Six weeks after ambulatory phlebectomy.
(A) Saphenous accessory varicose veins, incompetence of Dodd’s perforator (C2). (B) Six weeks after ambulatory phlebectomy.
(A) Reticular varicose veins (C1). (B) Six weeks after ambulatory phlebectomy.
Regional venous networks particularly appropriate for AP include accessory saphenous veins of the thigh, groin pudendal (perineal) veins, reticular varicose veins (popliteal fossa, lateral thigh, and leg, as described by Albanese), veins of the ankles, and the dorsal venous network of the foot.
While most procedures are performed in ambulatory patients, the technique may also be used in conjunction with other surgical procedures, such as high ligations (crossectomy), stripping of incompetent saphenous veins, and endovenous ablation (laser or radiofrequency) in ambulatory or stationary patients.
Contraindications are rare or relative and include critical arterial ischemia, infections, allergy to local anesthetics, bed ridden status, and impaired blood clotting or immunity. AP is usually not performed during pregnancy or immediately postpartum, as varicose veins frequently regress spontaneously.
EXPECTED BENEFITS
Since Muller’s first writings in 1966, AP has been considered a very effective and economical technique that affords outstanding cosmetic results (Muller 1966, Muller 1996).
Long-term results tend to be excellent as long as the most proximal source of reflux is eliminated; however, evidence-based objective data confirming this widely accepted conclusion continue to be sparse (Richards 2021). A single randomized, controlled trial by de Roos (2003) has been published and found excellent long-term results of AP (after 2 years) and verified its superiority to liquid sclerotherapy for treatment of the anterior thigh accessory great saphenous vein. An extensive study demonstrates satisfying long-term results of phlebectomy, even with the conservation of a refluxing saphenous vein (Pittaluga 2009, Scheerders 2022). Several recent studies have evaluated the results of different varicose vein surgery techniques, including phlebectomy, but only 1 year after the procedure, which is too short to draw any valid conclusions.
Improvement in anesthetic techniques with the advent of tumescence has resulted in greatly reduced pre- and postoperative pain, hematomas, and complications (Ramelet 2012). As AP is usually performed in the friendly environment of an office rather than in the operating room, it is mostly experienced as “quite comfortable” by patients.
The technique is safe, as noted by several publications that have reviewed reported complications of AP. The side effects of this procedure will be discussed later.
It should be noted that in order to obtain good results and prevent recurrences, AP must only be performed when it is indicated. When this procedure is selected, it must consist of removal of all segments of varicose veins, including feeding perforators, to prevent relapses or unsightly complications, such as telangiectatic matting.
AP is an easy and inexpensive procedure to perform. A skilled practitioner may remove an extensive array of varicose veins in a short period of time, generally lasting 20–90 minutes, with both legs being operated upon in a single session.
A simple, streamlined operative approach by a well-trained practitioner is much more effective and economical than “high-tech” new modalities.
OVERVIEW OF TREATMENT STRATEGY
Treatment Approach and Major Determinants
Major treatment modalities in phlebology include compression therapy, sclerotherapy, AP, endovenous ablation, surgery, and laser treatment. Each technique has its own indications and advantages, although there are some areas of overlap.
For most indications, the procedure most similar to AP is sclerotherapy. Sclerotherapy is principally indicated in the treatment of telangiectasias and reticular varicose veins. New modalities, such as foam sclerotherapy and ultrasound-guided sclerotherapy, afford excellent results in the treatment of intrafascial varicose networks, including postoperative relapse, the small saphenous veins, or saphenous and accessory saphenous veins of the thigh (see Box 10.4 ).
AP is superior to sclerotherapy in the treatment of medium to large, epifascial varicose veins. With AP, there are fewer recurrences and no risks of inadvertent intraarterial injection, skin necrosis (due to extravasation of sclerosant or unpredictable arteriovenous anastomosis injection), or residual hyperpigmentation.
The combination of ultrasound-guided sclerotherapy and AP opens up interesting prospects: suppression of proximal reflux by echosclerotherapy (glue may be an alternative) followed by phlebectomy of the residual varicose veins once the reflux has been suppressed. Phlebectomies can be performed in the same session. We prefer to wait 1 or 2 weeks between the two procedures, as preoperative bleeding is less significant when the proximal portion of the insufficient vein has been obliterated.
PATIENT INTERVIEWS
Elicitation of patient histories is discussed in a previous chapter. Recording structured case histories permits appropriate weighting of the various symptoms and venous risk factors and improved estimation of prognosis.
The physician must be especially receptive to the patient’s complaints and expectations, as postoperative patient disappointment is often less a matter of technical failure than the result of unrealistic patient expectations that were unchallenged prior to treatment.
Careful analysis of the patient’s history and symptoms may enable the physician to differentiate venous problems from arterial lesions, nerve root irritation syndrome, osteoarticular or muscle-tendon disease, and more generalized diseases, such as fibromyalgia. Some symptoms, such as muscle cramps and restless legs, are not very specific. Treatment of varicose veins is unlikely to result in the resolution of these symptoms, and the patient should be made aware of this.
The prognosis and likely evolution of chronic venous disease in each particular patient should also be discussed. Depending on the predominant type of varicose veins, the severity of the disorder, and the presence of specific risk factors, patients may be likely to encounter different clinical courses in the future.
CLINICAL EXAMINATION
This is an essential part of the treatment, as good AP results depend on the accuracy of the diagnosis and of a thorough evaluation of the exact origin and extent of the varicose veins. Clinical examination should be supplemented by DUS, as described in Chapter 4 (see Box 10.1 ).
TREATMENT TECHNIQUES
Equipment
Only a few surgical instruments and forms of equipment are required ( Box 10.5 ) for AP. Among the types of hooks that have been marketed for vein grasping and extraction are the Muller, Oesch, Ramelet, Tretbar, and Varady ( Figs. 10.4–10.7 ).
Box 10.5
Equipment Necessary for Phlebectomy
-
•
Local buffered anesthetic, normal saline, or Ringer’s solution
-
•
Resuscitation equipment, indispensable during any procedure
-
•
Sterile gloves and mask
-
•
Disinfectant (not removing the marking stain of the course of varicose veins)
-
•
No. 11 straight blade scalpel
-
•
18-Gauge needle
-
•
Phlebectomy hooks
-
•
Mosquito forceps
-
•
Sterile pads
-
•
Dressing materials
-
•
Elastic bandages
(A and B) Phlebectomy hooks by Ramelet. (C and D) New phlebectomy hooks by Ramelet.
(Courtesy HEBUmedical.)
Phlebectomy hooks by Muller.