Abstract
Allergic contact dermatitis (ACD) is caused by a delayed hypersensitivity reaction within the skin, manifesting as a pruritic dermatitis initially at the site of skin contact with the allergen. Clinical patterns will vary based on the actual allergen involved, but eyelid dermatitis is very suggestive of ACD. ACD may coexist with irritant contact dermatitis, contact urticaria, and various forms of endogenous eczema which can complicate establishing an accurate diagnosis. ACD is diagnosed via patch testing, where allergic reactions are reproduced on the back over several days. There are a number of regional baseline series used for patch testing, which have been developed to incorporate the most important allergens in different geographical locations. These include metals (e.g. nickel, chromate), fragrances, preservatives (e.g. methylisothiazolinone), formaldehyde and formaldehyde releasers (e.g. quaternium-15), the hair dye p -phenylenediamine, topical antibiotics (e.g. neomycin, bacitracin), and rubber accelerators. The most important aspect of treatment is allergen avoidance. In addition, skin inflammation is addressed by topical corticosteroids, moisturizing creams, and avoidance of skin irritants.
Keywords
contact dermatitis, allergic contact dermatitis, allergens, patch testing, patch tests, nickel allergy, methylisothiazolinone, airborne contact dermatitis, systemic contact dermatitis, cosmetic allergy, delayed hypersensitivity reaction
- ▪
Allergic contact dermatitis (ACD) is a pruritic, eczematous reaction
- ▪
Acute ACD and many cases of chronic ACD are well demarcated and localized to the site of contact with the allergen
- ▪
ACD can also have a diffuse or patchy distribution, depending on the allergen and/or the development of disseminated eczema (autosensitization dermatitis)
- ▪
The prototypic reactions are ACD caused by poison ivy and nickel
- ▪
ACD may coexist with irritant contact dermatitis, contact urticaria, and different forms of endogenous eczema
- ▪
Patch testing remains the gold standard for accurate and consistent diagnosis
Introduction
When the skin comes in contact with external agents, many adverse events can occur including contact dermatitis, which can be either allergic or irritant. Irritant contact dermatitis (ICD) accounts for ~80% of all contact dermatitis (see Ch. 15 ), with allergic contact dermatitis (ACD) accounting for the remainder . ACD is a delayed-type hypersensitivity reaction that is elicited when the skin comes in contact with a chemical to which an individual has previously been sensitized.
The cutaneous responses of ACD are dependent on the particular chemical, the duration and nature of the contact, and individual host susceptibility. The chemicals that cause contact dermatitis may be found in jewelry, personal care products, plants, topical medications (prescription, over-the-counter or herbal), clothing and home remedies, as well as chemicals the individual comes in contact with at work, during avocations, or via contact with another individual (e.g. consort contact dermatitis).
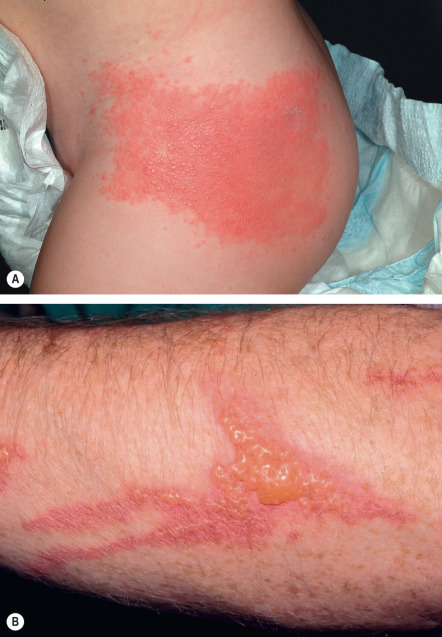
ICD and ACD, especially the chronic forms, can take on similar clinical appearances. The classic picture of contact dermatitis is a well-demarcated, erythematous, vesicular and/or scaly patch or plaque with well-defined margins corresponding to the area of contact ( Fig. 14.1A ). The distribution can be linear, when an object such as a leaf or branch is rubbed against the skin ( Fig. 14.1B ), or localized to the site where there has been contact with the offending chemical or product, e.g. hand dermatitis caused by ACD to epoxy resin or foot dermatitis due to ACD to the components of shoes ( Figs 14.2–14.4 ). Because ICD and ACD are not always discernible clinically, patch testing is required to help identify an allergen or exclude an allergy to a suspected allergen. While patch testing remains the gold standard for diagnosing ACD, it is important to note that ICD and ACD may coexist.



Patients with the most common clinical presentations of ACD often do not seek medical attention. Those who have earring dermatitis or erythema and pruritus under a ring may simply diagnose themselves as having an allergy to jewelry. An individual who is gardening over the weekend may never present to a physician, because the “poison ivy rash” is so familiar. Nickel (worldwide) and poison ivy (US; see Ch. 17 ) are among the most common etiologies of ACD and are often not further investigated because the cause is obvious. However, oftentimes, the clinical picture and history are not sufficiently specific to identify the causative allergen, and patch testing is then necessary. For example, the patient with chronic hand dermatitis or eyelid dermatitis who comes to the office for treatment is often unaware that a personal care product could be the cause of the problem. These are the patients who can be most helped by a thorough history and cutaneous examination, as well as the diagnostic procedure of patch testing.
History of Patch Testing
Jadassohn has been credited with describing the technique of patch testing over 100 years ago. In 1931, Sulzberger and Wise formally brought the technique to the US and described its use as a diagnostic tool for identifying a causative allergen responsible for dermatitis. This technique has been further developed over the years on a worldwide basis, with standardized allergens, testing devices, and protocols as well as numerous regional baseline series.
Epidemiology
ACD can affect individuals in all walks of life. It can affect the old, the young, and individuals of all races and both sexes. Differences between genders may be seen but are generally based upon exposure patterns, such as nickel allergy occurring more frequently in women, presumably because of their greater exposure to jewelry . Occupations and avocations also play an important role in the epidemiology of ACD (see Ch. 16 ). Allergens, and therefore patch test results, differ from region to region, e.g. preservatives used in personal care products can vary based on government legislation. While quaternium-15 is a cosmetic preservative that commonly causes ACD in the US, some have argued that it is not even needed in the European Baseline Series . In addition, even in a particular locale, some allergens can increase in clinical importance over time while others decrease due to usage patterns, and new allergens are continually being introduced.
Pathogenesis
ACD is a delayed-type hypersensitivity response. It is an allergen-specific reaction that requires prior sensitization of the individual to the chemical in question. The pathogenesis of ACD involves an initial sensitization phase when the patient first comes in contact with the chemical, which penetrates the skin and then elicits a cascade of events that results in sensitization (see Ch. 4 for details). The subsequent re-exposure of the skin leads to the presentation of the responsible allergen to an already primed T-cell milieu, causing the release of multiple cytokines and chemotactic factors and resulting in the clinical picture of eczema. Once sensitized, all that is needed to elicit a reaction is contact with a low concentration of the causative chemical.
Clinical Features
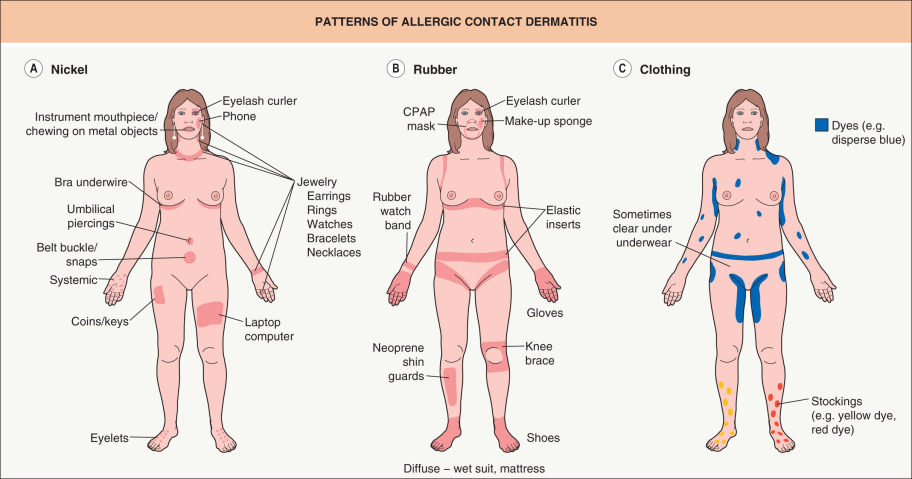
In order to diagnose ACD and treat it adequately, the clinician needs to be familiar with its clinical presentations. The typical appearance is often a well-demarcated pruritic eczematous eruption, which may be acute (blistering, weeping and/or edema, e.g. Figs 14.1, 14.5 & 14.6 ) or chronic (lichenified or scaly plaques, e.g. Figs 14.2, 14.3, 14.4B, 14.7 & 14.8 ). This reaction is typically localized to the area of skin that comes in contact with the allergen ( Fig. 14.9A,B ). However, the clinician must also be aware that patchy or diffuse distributions can also be seen, depending on the nature of the causative allergen ( Figs 14.9C & 14.10 ). For example, body washes or shampoos that are rinsed over the body may cause a more patchy or diffuse clinical dermatitis. Other less common presentations of allergic contact dermatitis are listed in Table 14.1 .





| RARE TO UNCOMMON PRESENTATIONS OF ALLERGIC CONTACT DERMATITIS | |
|---|---|
| Based primarily upon morphology | Based primarily upon distribution and/or pathogenesis |
|
|
* The lesions of erythema multiforme may favor sites previously unaffected by poison ivy.
† Overlap with systemic contact dermatitis and clinical overlap with s ymmetrical d rug- r elated i ntertriginous and f lexural e xanthema (SDRIFE; see Table 21.14 ).
Pathology
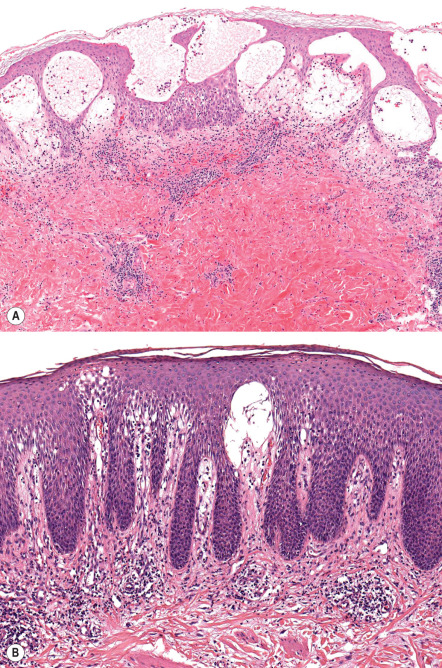
Although the diagnosis of ACD is in large part a clinical one aided by the diagnostic procedure of patch testing, histology can sometimes be helpful. This is especially true when excluding other diagnoses, such as mycosis fungoides. The pathology of ACD is most helpful in acute lesions, as subacute or chronic lesions often produce confusing patterns that are not diagnostic. Histologically, ACD is the prototype of spongiotic dermatitis. In the acute stage, there is a variable degree of spongiosis, with a mixed dermal inflammatory infiltrate containing lymphocytes, histiocytes and a variable number of eosinophils. In moderate to severe reactions, marked spongiosis results in intraepidermal vesiculation ( Fig. 14.11A ). In subacute to chronic stages, epidermal hyperplasia, often psoriasiform, develops ( Fig. 14.11B ).
However, even when spongiotic dermatitis is present, clinicopathologic correlation is always required, as ACD is not the only cause of this reaction pattern. In addition, as with any dermatitis, the application of topical corticosteroids may alter the histologic findings. Occasionally, other histopathologic patterns are seen in ACD, as outlined in Table 14.1 .
Differential Diagnosis
The differential diagnosis of ACD includes many other forms of dermatitis, such as ICD, protein contact dermatitis, atopic dermatitis, stasis dermatitis and seborrheic dermatitis, as well as the erythematous form of rosacea. Hand and foot ACD also needs to be distinguished from endogenous dermatitis, psoriasis, and tinea (see Table 13.4 & Fig. 15.6 ). Of note, these conditions may coexist, which can make clinical assessment complicated. In general, when evaluating regional dermatoses (e.g. eyelid, hand and foot), other disorders common to the area need to be considered as well as allergens specific to that area ( Table 14.2 ). If there is widespread disease, either because of widespread contact with an allergen or autosensitization, additional causes of erythroderma (see Ch. 10 ), e.g. Sézary syndrome, enter the differential diagnosis.
| EYELID DERMATITIS – DIFFERENTIAL DIAGNOSIS AND MOST COMMONLY ASSOCIATED ALLERGENS | |
|---|---|
| DIFFERENTIAL DIAGNOSIS |  |
| Endogenous | |
| |
| Exogenous | Allergens most commonly associated with ACD of the eyelids * |
|
|
* Adapted from North American Contact Dermatitis Group (2003–2004); Dermatitis. 2007;18:78–81.
Deciphering and differentiating these diseases can sometimes be a challenge. Distribution and history can be helpful (see Figs 14.1, 14.4, 14.5 ), as can simple tests such as a KOH preparation. In addition, dermatoses are sometimes multifactorial, and ACD may be superimposed on atopic dermatitis or stasis dermatitis. However, in order to diagnose ACD, the clinician must first consider the possibility, then ask the right questions, and, finally, use the appropriate allergens to diagnose this condition. What follows will hopefully provide the clinician with an outline to the appropriate questions to ask and procedures to use when investigating ACD.
Patch Testing
Patch testing is a deceptively simple office procedure upon which the diagnosis of ACD often rests. Although the procedure is straightforward, deciding when and what to patch test requires training and experience. Unfortunately, patch testing is still underutilized. Past surveys have shown that only 50% of all residency programs in the US have a patch test center, and 27% of the responders did no patch testing at all .
The T.R.U.E. TEST ® , which is approved by the US Food and Drug Administration (FDA), consists of panels with pre-impregnated allergens, allowing for increased ease of use and perhaps resulting in increased patch testing. However, it currently screens for 36 allergens, including a negative control, and although this is helpful, extended testing beyond these allergens has been shown to improve diagnostic accuracy . With extended testing, 37–76% more positive reactions were detected, and 47% of the patients had positive reactions only to non-screening allergens (these latter allergens come in multi-use syringes or tubes [see Appendix]). Lastly, when patch testing was performed with 28 T.R.U.E. TEST ® allergens, only 27.6% of patients had completely detected allergens .
Prior to the application of the patch tests, the clinician should ask questions about exposures both at home and at work, and attempt to understand the mechanics of the work environment. The effect of vacations and time away from work or home should also be ascertained. In addition, all personal care products should be inventoried and hobbies explored. The information gained can help to direct allergen selection more appropriately.
Technique
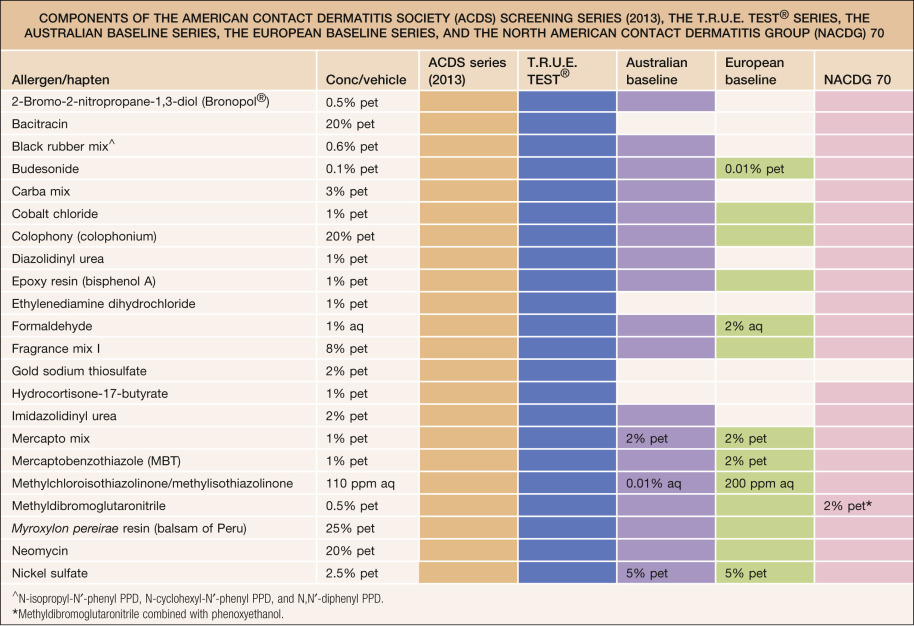
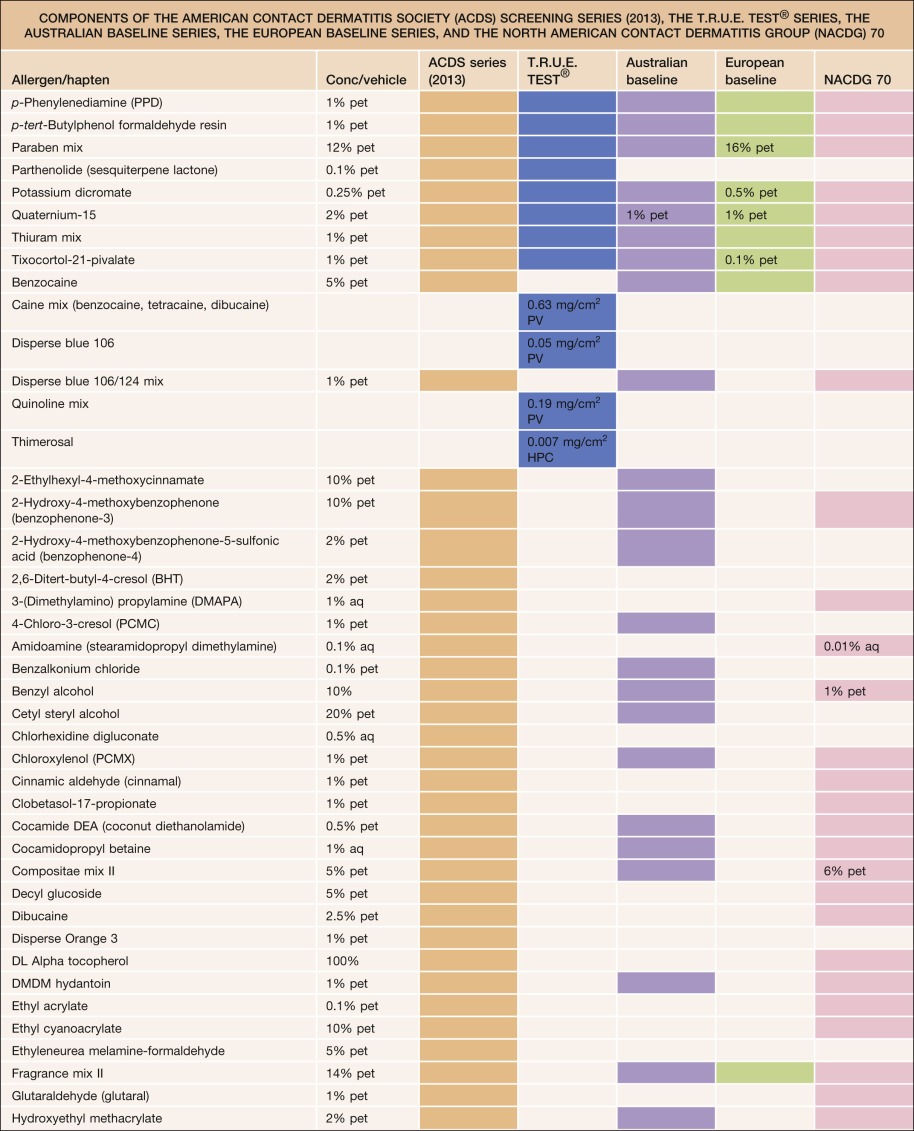
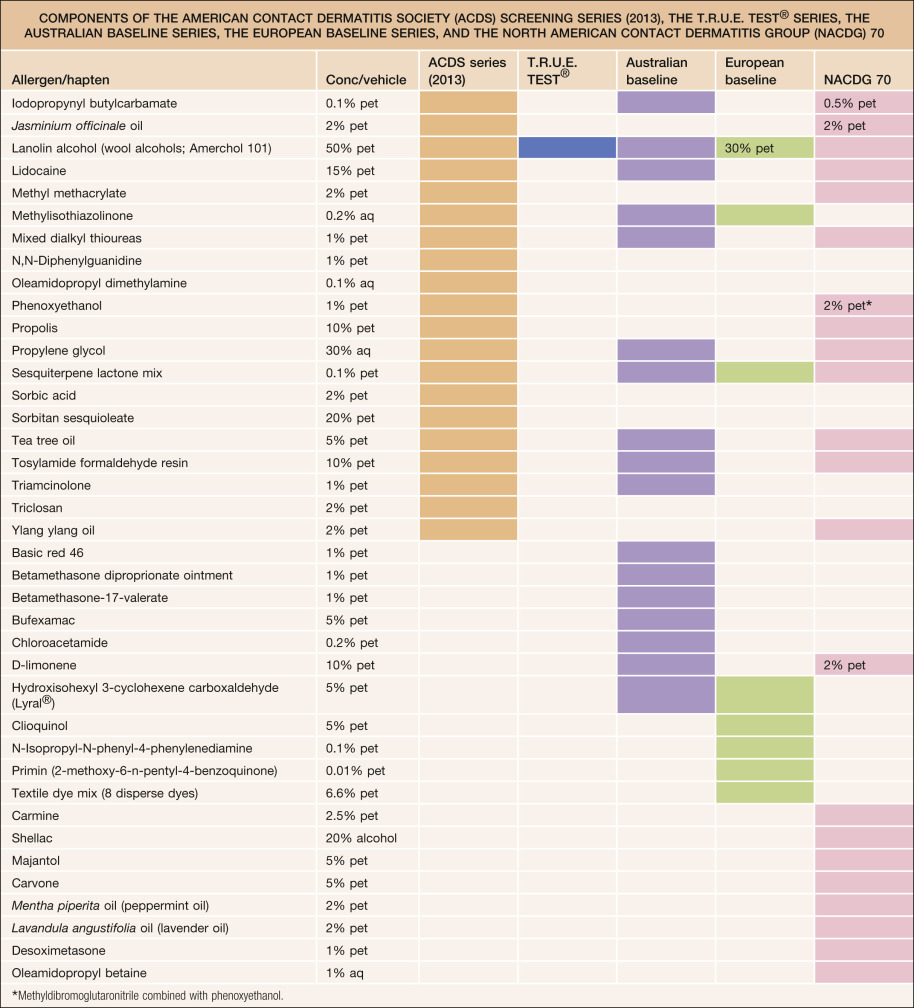
Although the T.R.U.E. TEST ® now has 35 allergens (plus control) and the European Baseline Series 30 allergens ( Table 14.3 ), referral centers with patch test clinics routinely patch test to an “expanded” series of 60+ allergens. Such panels include the North American Contact Dermatitis Group 70, the American Contact Dermatitis Society Series (2013), and the Australian Baseline Series, in addition to more specific allergen panels, e.g. the hairdressing tray, dental tray or florist tray, which contain allergens unique to a particular occupation. The companies from which these allergens and other supplies can be obtained are listed in the Appendix. Although these expanded series of allergens are not FDA-approved, they are often required to establish the precise etiology of the patient’s dermatitis.
Substances brought by patients to the dermatologist should not be tested in a blinded fashion. The physician should be aware of the chemical ingredients of the product, or severe irritation such as a burn or ulceration could occur. Therefore, no unknown product or chemical should be applied as a patch test. Material safety data sheets (MSDS) can sometimes help in further evaluating the chemical. However, not all ingredients are listed on these forms: those chemicals that represent a small percentage and fall below a certain threshold do not need to be listed, even though they may be the causative allergens. Identification of the latter requires communication with the manufacturer, so that full disclosure of the chemical ingredients can be obtained.
When patients bring all their personal care products to the office for patch testing, special attention is required. The general rule regarding testing of these products is that products intended to be left on the skin (so-called “leave-on” products), such as moisturizers and make-up, may be tested “as is”. Products that are intended to be diluted by water or rinsed off (so-called “rinse-off” products), such as soaps and shampoos, need to be diluted prior to patch testing (often to 1–10% in water). There are helpful guides for determining appropriate patch test concentrations for numerous chemicals . When these nonstandard allergens are tested, controls (including vehicles) must be tested to evaluate for the possibility of ICD.
After allergen selection has been finalized, appropriate technique is necessary to ensure adequate testing. The most common site is the upper back. The patient should not have a sunburn in this area and should not have applied topical corticosteroids to the sites of patch testing for 1 week . Systemic and longer-lasting injectable corticosteroids should also be avoided for at least 1–2 weeks . (If necessary for disease control, the daily oral AM dose of corticosteroids should not exceed the equivalent of 20 mg of prednisone during testing.) Any one of these factors may decrease the individual’s ability to elicit a reaction when challenged by an allergen, resulting in a false-negative test .
A nurse or technician in the office can be trained to apply the patches, and this leads to improved efficiency. Either the pre-packaged allergens are placed on the back as in the case of the T.R.U.E. TEST ® , or the allergens are dispensed into chambers. There are a number of different patch test systems, including Finn Chambers ® (SmartPractice, Phoenix, AZ) which are adhered to Scanpor ® tape (Norgesplaster, Vennesla, Norway; available in the US from SmartPractice); allergEAZE TM chambers (SmartPractice, Phoenix, AZ; Fig. 14.12 ); and IQ, IQ Ultra TM , or IQ Ultimate TM chambers (Chemotechnique Diagnostics; distributed by Dormer Laboratories, Inc.). These patches are applied to the back, reinforced with more Scanpor ® tape if required, and the patient is sent home with instructions to keep the back dry and the patches secured until the second visit at 48 hours. Patients should also be told to avoid excessive sweating and to avoid heavy lifting, as the patches may come loose. Antihistamines can be prescribed, as they will not affect the outcome of the testing. A map of where the allergens were placed should be constructed for future reference.
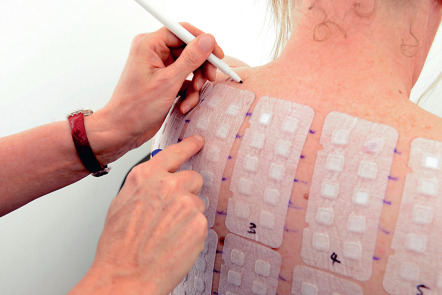
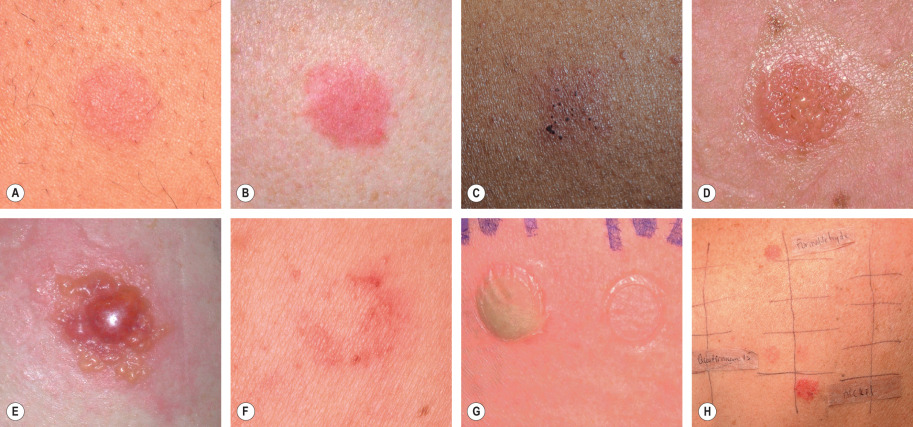
When the patient returns at 48 hours, the patches need to be examined to ensure that the testing technique was adequate. Initial inspection can determine that the patches are still in place. Confirmation comes from observing whether the chambers have adhered adequately so as to leave an impression in the skin (see Fig. 14.14G ). As the patches are removed, their sites of application should be marked in order to identify the location of the particular allergens ( Fig. 14.13 ). Two types of marking pen are recommended for this procedure: either a permanent surgical marker or a fluorescent highlighter. Highlighters are less messy and do not rub off as easily as the permanent marker. Because of the latter property, permanent markers can soil clothing and make interpretations at the second reading more difficult. Any positive reactions are scored according to the International Grading System ( Table 14.4 ; Fig. 14.14 ). The patient is again asked to keep the back dry until the second reading, which can be performed from 72 hours to 1 week after the initial application of patches.

| INTERNATIONAL GRADING SYSTEM FOR PATCH TESTS | |
|---|---|
| +/− | Doubtful reaction, faint macular erythema |
| + | Weak, non-vesicular reaction with erythema, infiltration and papules |
| ++ | Strong, vesicular reaction with erythema, infiltration and papules |
| +++ | Spreading bullous reaction |
| − | Negative reaction |
| IR | Irritant reaction |
When the patient returns for the second reading, the map is used to identify any positive reactions. If a fluorescent marker has been utilized, a Wood’s lamp may be needed to identify the markings. Positive reactions are again graded according to the standard system (see Table 14.4 ). This later reading is necessary as patch test responses to some allergens such as gold, neomycin, and corticosteroids may be delayed. The actual products the patient uses in his or her work and/or home environment are examined and the ingredients compared with the positive reactions. In so doing, products can be divided into groups: those that are free of the suspected allergen(s) and are safe to use, and those that contain these chemical(s) and should be avoided. There will usually be some products with no ingredients listed, and these will have to be further investigated by the patient or physician by contacting companies and inquiring about ingredients.
Interpreting the test
Through the process of reviewing exposures and products, the clinical relevance of positive test results can be determined. Allergens may have past relevance. For example, a patient who presents with a known allergy to nickel and reactions to costume jewelry is found on patch testing to have a positive reaction to nickel. The nickel may have past relevance to the patient’s problem with costume jewelry but no current relevance to the chronic hand dermatitis. Relevance may also be determined to be current. For example, a positive reaction to tuliposidase A (see Ch. 17 ) in a florist who has hand dermatitis and contact with Alstroemeria when arranging flowers would have present relevance. In some individuals, relevance may be unknown, as in a patient with an eyelid dermatitis and a positive reaction to thimerosal but no past history of an allergy to contact lens solutions and no identifiable contact with thimerosal.
Treatment and Patient Education
Once allergens are positively identified, the patient should be given written information on all of these chemicals. The information sheets should contain data regarding the name of the chemical, possible synonyms, typical uses for the chemical, how to avoid exposure, and, when appropriate, substitutions. The sheets can be individually composed or obtained from books and copied for patient use . In addition, the American Contact Dermatitis Society website ( www.contactderm.org ) is an excellent resource for allergen and product information, including patient information sheets ( Table 14.5 ). The Contact Allergen Management Program (CAMP) is another feature of the website (available to members of the society): this allows the user to input the known allergens and the database assembles a list of products free of the allergens entered. With this CAMP-generated list, the patients can then purchase products that lack the ingredients to which they are allergic. In addition, this website contains a Contact Dermatitis Alternatives Database which assists both patients and physicians with regard to appropriate substitutions for known allergens.
| ACDS EXPOSURE INFORMATION SHEET: BALSAM OF PERU | ||
|---|---|---|
| Other names | ||
| Myroxylon pereirae , Black balsam, Toluifera pereirae balsam, Honduras balsam, China oil | ||
| This complex substance contains many potential allergens: benzoic acid, benzyl acetate, benzyl benzoate, benzyl cinnamate, cinnamic acid, cinnamic alcohol, cinnamic aldehyde, cinnamyl cinnamate, eugenol, farnesol, isoeugenol, nerolidol, and vanillin | ||
| What is it? | ||
| Balsam of Peru is a sweet-smelling natural substance derived from the bark of a tree native to Central America. For decades it has been added to topical preparations for its aroma and its antibacterial effect. | ||
| Where might it be found? | ||
| Hemorrhoid treatment | Rectal suppository | Diaper or medicated ointment |
| Burn treatment or wound spray | Analgesic rub, liniment | Baby powder |
| Antiseptic lotion or cream | Deodorant | Feminine hygiene spray |
| Chinese ointment, Tiger balm | Aromatherapy product | Consecrated oil, incense |
| Dental cement | Hair tonic or pomade | Shampoo, conditioner |
| Shaving lotion, aftershave | Perfume, cologne | Cosmetic with fragrance |
| Sunscreen, tanning lotion | Toothpaste, mouthwash | Lip balms, chewing gum |
| Cough medicine, lozenges | Scabies treatment | Tincture of benzoin |
| Scented cleaning product | Scented candle | Air freshener, deodorizer |
| Scented paper product | Pet care product | Pesticide |
| Violin rosin | Histology slide fixative | Scented tobacco, coffee, tea |
| How to avoid it: | ||
| ||
| Dietary restrictions to avoid balsam of Peru | ||
| Avoid the following: citrus fruits and products that contain citrus flavor, peel, zest, or oil; tomatoes and tomato-containing products; spices such as cinnamon, cloves, vanilla, curry, nutmeg, allspice, anise and ginger as well as spicy condiments; sweet flavorings ; colas , i.e. soft drinks, such as Dr Pepper, that may contain sweet flavorings and spices; and liquors such as wine, beer, gin and vermouth | ||
| Related substances | ||
| You may show a cross-reaction to some closely related substances that are derived from plants. If you are not successful in clearing your skin rash by strictly avoiding sources of balsam of Peru, you may also need to avoid these: | ||
| Beeswax | Benzaldehyde | Benzoic acid |
| Benzoin | Benzyl salicylate | Colophony |
| Coniferyl alcohol | Coniferyl benzoate | Coumarin |
| Diethylstilbestrol | Resorcin monobenzoate | Resorcinol |
| Propolis | Storax | Tolu balsam |
| Wood tars | ||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


