Alar Contour Grafts
Jacob G. Unger
Rod J. Rohrich
DEFINITION
The alar contour graft (ACG) is a cartilaginous strut utilized in rhinoplasty to strengthen and reinforce the alar rim placed along the alar margin1 (FIG 1).
ACG is synonymous with alar rim graft.
Alar retraction is excessive elevation of the alar rim as evidenced from an AP or lateral view with >2 mm of elevation from the long axis of the nostril.2
Alar collapse is a malformation of the rim on basal view that can occur when the lower lateral cartilage (LLC) is congenitally cephalically oriented, resulting in a loss of support along the anterior portion of the alar rim with a subsequent concavity. This deformity may be static, dynamic, or both.
ANATOMY
ACGs are intimately related to the aesthetics of the alar rim. The ideal alar rim is defined on lateral view by a smooth contour with a slight arch, peaking vertically between the level of the tip defining points and the columellar-lobular angle. Further, the height of the alae should be no higher than 2 mm above or 2 mm below the long axis of the nostril.
The alar rim is largely composed of thick, lower nasal skin superficially and mucosa internally.
The lateral crus of the LLC normally runs parallel to the alar rim. The LLC may be cephalically oriented, which predisposes to alar deformity. The orientation of the LLC helps determine the shape of the ala anteriorly in the area of the soft triangle.
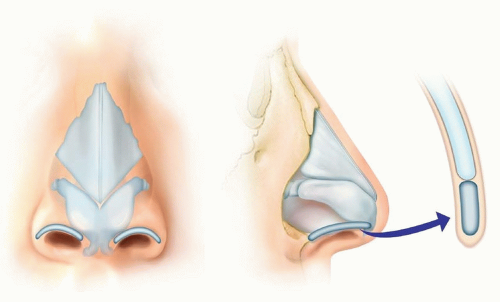
FIG 1 • Alar contour grafts.
PATIENT HISTORY AND PHYSICAL FINDINGS
Visual inspection and manual palpation of the nose will indicate if any alar rim deformities are present in the preoperative state. Standard rhinoplasty imaging should be undertaken with AP, lateral, basal, and ¾ views of the nose. Visualization of the lateral crura of the LLC through the skin envelope can help diagnose a more vertical orientation, which may portend a higher risk of future alar deformities.
Forced inspiration through the nares will uncover any dynamic external nasal valve collapse or evidence of alar collapse.
IMAGING
No imaging is necessary or indicated to prepare for alar rim deformity correction with ACG.
Three-dimensional imaging may be useful as a preoperative planning and patient communication tool. Caution is advised not to “lower” the alar position with a computer program if one does not feel that this is a consistently reproducible surgical outcome in his or her hands. However, this imaging may help educate patients how reinforcement of alar retraction or collapse with ACG may be very useful, as well as indicating changes in alar-columellar relationships.
SURGICAL MANAGEMENT
It is crucial that the correct diagnosis is made to ensure the most accurate surgical treatment. Most crucially, if the patient has had severe mucosal loss and shortening due to previous surgery, this must be disseminated to the patient. This is a much more difficult problem to correct and may require mucosal grafts or other interventions beyond placing ACGs.
In a virgin nose, alar retraction, notching, and collapse, both static and dynamic, can be treated with operative placement of ACGs. It is important to note the position of the LLCs as well. If they are cephalically oriented, some inferior repositioning may be indicated as well using lateral crural strut grafts or other techniques.Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


