Key points
• The advantage of using CBCT is the accurate visualization of the root angulations.
• Initial records using CBCT technology and intraoral scans of the dentitions can be used to simulate treatment outcomes, and this can be extremely helpful in choosing among multiple treatment options.
• One of the major benefits of CAD/CAM orthodontics is the straight-line approach of tooth movement from its initial position to the endpoint.
• Computer aided treatment planning and modern materials that allow the orthodontist the ability to diagnose and treatment plan more accurately by visualizing a simulated endpoint.
• One of the major benefits of simulations is the ability for the surgeon and the orthodontist to collaborate on the visualization of the outcome and the education of the patient.
• Today, dental extraction is much less common due to several advances in growth modification and dental compensation, and this can help establish good occlusal intercuspation in severe cases.
• Temporary anchorage devices (TADs), buccal shelf screws and bollard skeletal anchorage plates for maxillary protraction allow nonsurgical skeletal movement to treat skeletal discrepancies using growth modification appliances.
• The use of TADs has several major advantages over distraction osteogenesis, including reduction in surgical complexity, because there is no maxillary osteotomy and significant improvement in patient comfort.
Introduction
Orthodontics has seen a number of major advances in the past 20 years. , The introduction of high memory, resilient metals, and three-dimensional cone beam computed tomography (3D CBCT) imaging could be chapters on their own for the significance they have had on the profession. However, for the purposes of this chapter, we would like to concentrate on the paradigm shift to computer-aided design and computer-aided manufacturing (CAD/CAM) that has changed the entire orthodontic delivery system and can be leveraged to significant advantage for the craniofacial and surgical population.
Precision in orthodontic alignment is always a primary objective of any treatment plan and even more critical when orthodontic treatment is combined with orthognathic surgery. The better the alignment and fit of the occlusion at the time of the procedure, the less likely that occlusal interferences could affect surgical outcome and stability. With CAD/CAM technology, not only can we visualize the skeletal structure and dental anatomy better than we ever have, but we can make diagnoses and plan treatments more accurately because we can visualize a simulated endpoint.
Several manufactures have developed systems utilizing CAD/CAM technology to generate the forces necessary to move teeth. Invisalign (Align Technology) was the first to use computer-aided design to manufacture clear, removable “Aligners” in 1997. SureSmile (OraMetrix) was the first to introduce, in 1998, a customized computer-aided orthodontic wire system, which has been commercially available since 2005.
For the purpose of this chapter, we will discuss these two systems as representatives of the many manufacturers that have introduced competitive products in the past 10 years.
What is the advantage of suresmile?
In conventional orthodontic treatment, stainless steel wires were the foundation of the mechanical forces for tooth movement, but heavy wires produce a high initial pressure that dissipates very quickly and often overpowers the periodontal ligament, causing cellular necrosis. A major advantage of the newer, high-memory metals, such as copper–nickel–titanium (CuNiTi), is the ability to exert a very light pressure over a long period and that large deflections do not necessarily increase force levels. Light, continuous pressure produces the most efficient tooth movement, healthier roots, and periodontal bone support while providing greater patient comfort. The challenge with the soft resilient metals is that they are difficult to bend. Flexible metals that are able to retain bends, for example, Beta-Titanium, often become fragile and break.
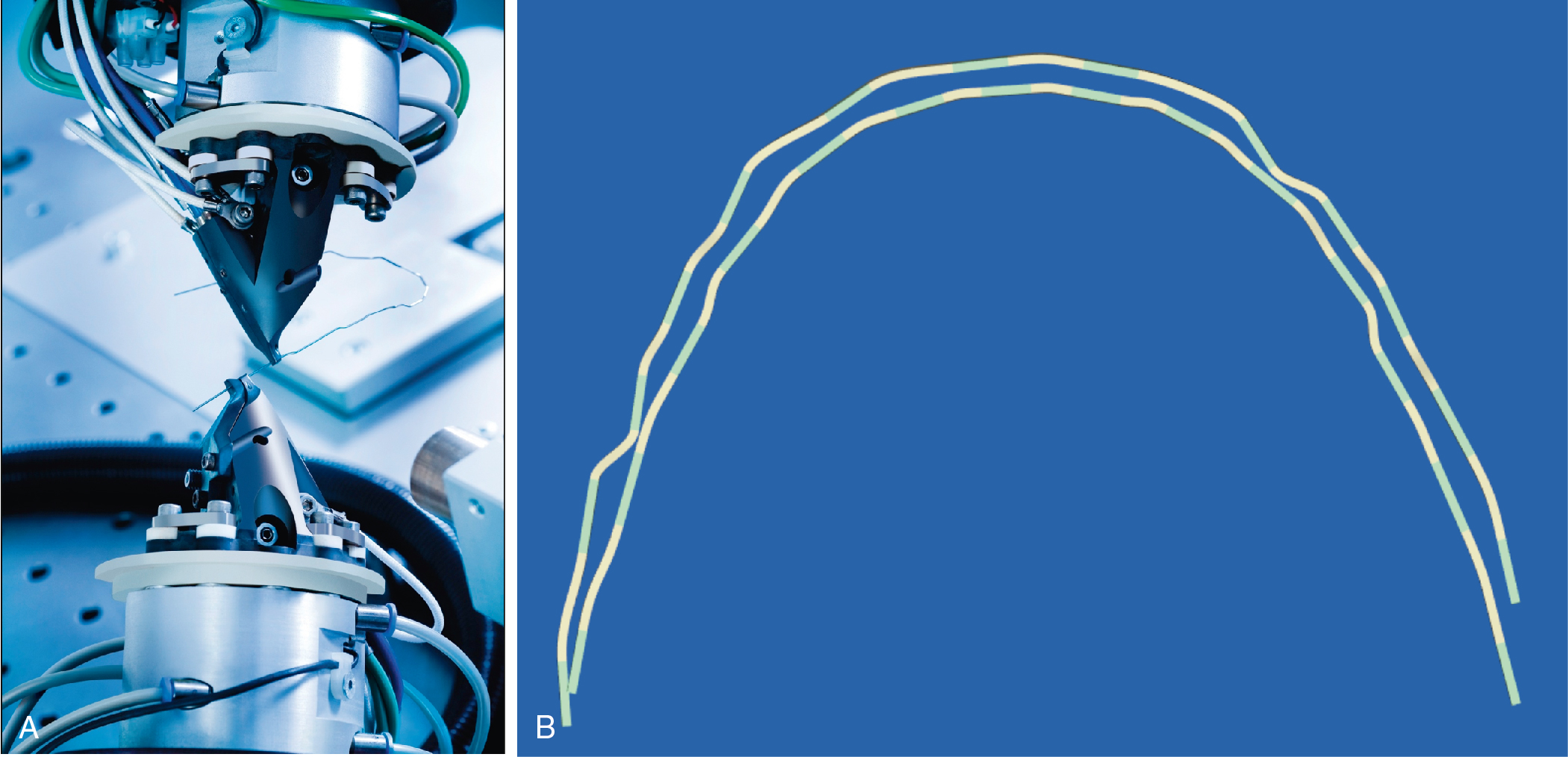
The SureSmile process ( Fig. 18.1 ) starts with a CBCT scan or an optical scan of the dentition to create a digital model. The advantage of using CBCT is the accurate visualization of the root angulations. The SureSmile software allows for individual teeth and brackets to be digitally moved to create an ideal setup of the final tooth position within the maxillary and mandibular dental arches. Sequential computer-aided/manufactured orthodontic wires are fabricated from the initial position to the final position of the dentition. The customized wires can be made from a variety of sizes (0.016 round to 0.019 × 0.025 rectangular) and materials (CuNiTi, Beta-Titanium, Elgiloy, and TiNb). The SureSmile laboratory uses a robotic arm to heat the wire, make the appropriate bends, and cool the wire so that the bends will be maintained ( Fig. 18.2 ).
SureSmile technology has an advantage over other CAD/CAM systems because the system itself is bracket agnostic—meaning, orthodontists can choose whatever bracket they are most comfortable with.
Diagnostic simulations
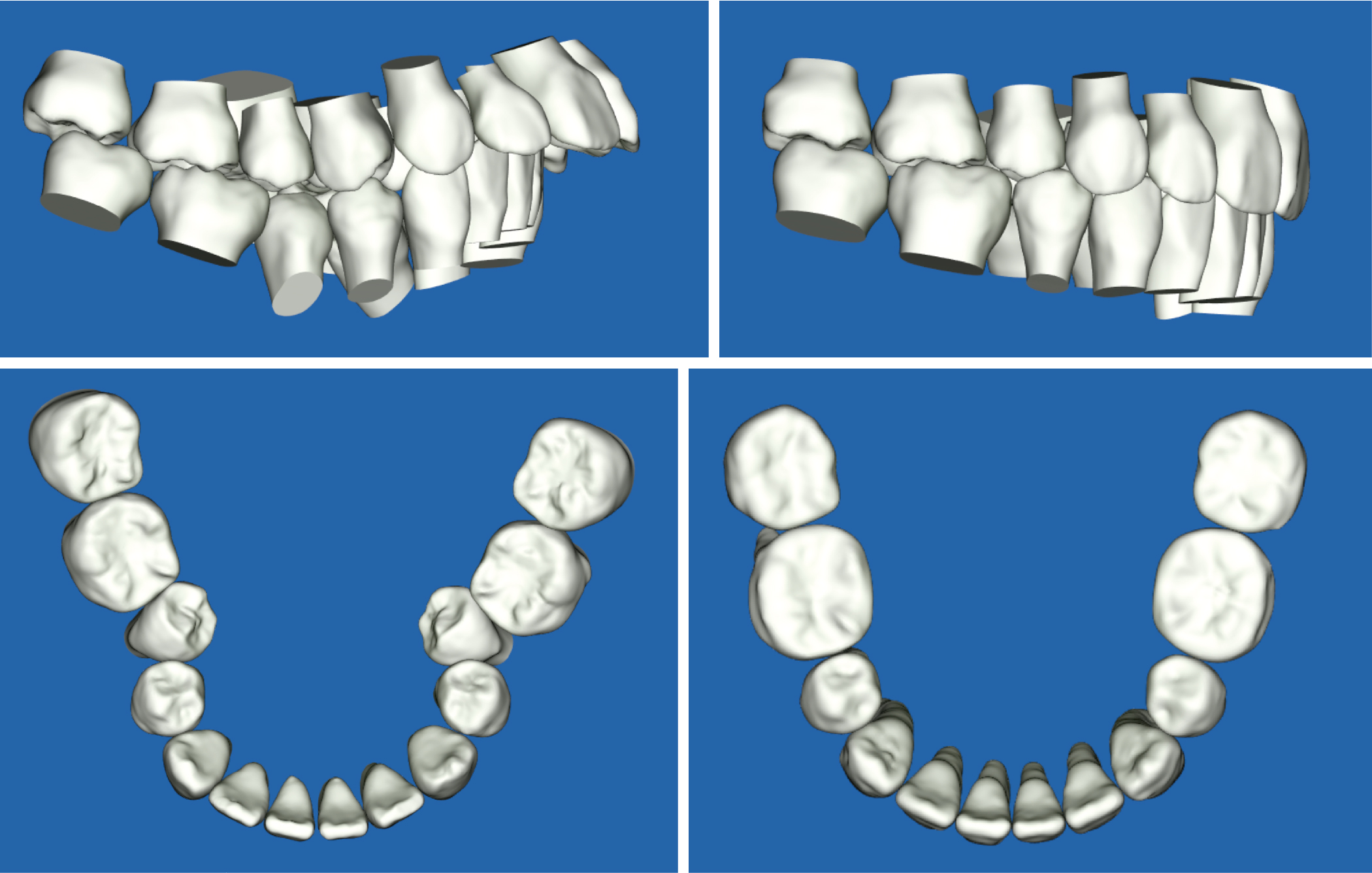
Initial records using CBCT technology and intraoral scans of the dentitions can be used to simulate treatment outcomes, and this can be extremely helpful in choosing among multiple treatment options. Fig. 18.3 shows the initial scan of a patient with severe crowding. The SureSmile software allows the orthodontist to easily manipulate the model teeth to create simulations to visualize and measure the amount of expansion needed to align teeth and help determine the need for extraction. This can be extremely useful in situations where multiple missing teeth can produce unusual occlusal schemes and require adjustments in alignment to produce even occlusal contacts.
Indirect bonding setups
CAD/CAM technology has made the process of indirect bonding more accurate and time efficient. The advantage of placing the brackets on a simulated model first is that the position of the bracket can allow the initial light wires with very little force and high resiliency to achieve greater accuracy in arch alignment and coordination. The goal of presurgical orthodontics is to remove dental interferences and compensations that can impede proper seating of the occlusion. Placing brackets in an exact location to allow a “straight wire” (meaning, no bends) to align teeth into a perfect fit is challenging due to the variations in tooth anatomy and the severity of the initial malposition. , With that said, the more accurate the bracket placement, the more efficient is the tooth movement. The fastest tooth movement is accomplished with the least adjustments. One of the major benefits of CAD/CAM orthodontics is the straight-line approach of tooth movement from its initial position to the endpoint. Conventional wire mechanics often move a tooth too far or too little with constant adjustments to the puzzle until all teeth fit in their proper positions. Every adjustment can produce an unwanted side-effect movement to adjacent teeth and slow the process.
Indirect bonding has the benefit of being more comfortable for the patient. The key to any bonding procedure is keeping teeth dry, and this may require cheek and tongue retractors, which many patients find uncomfortable. In most cases, because the entire arch is placed at one time, the time necessary to place the brackets and wear the retractors is greatly reduced.
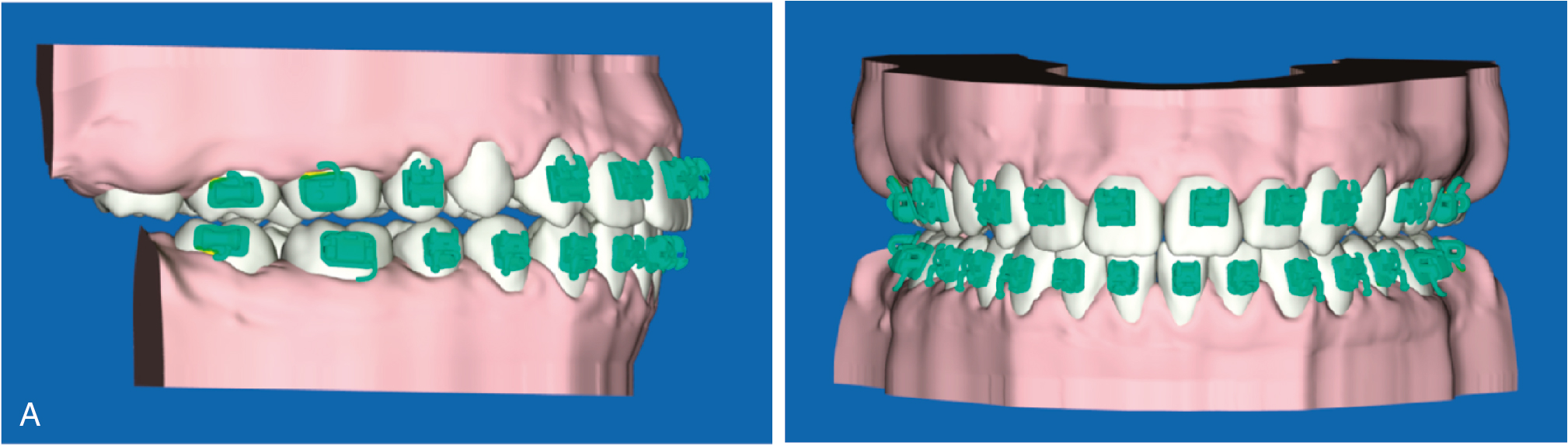
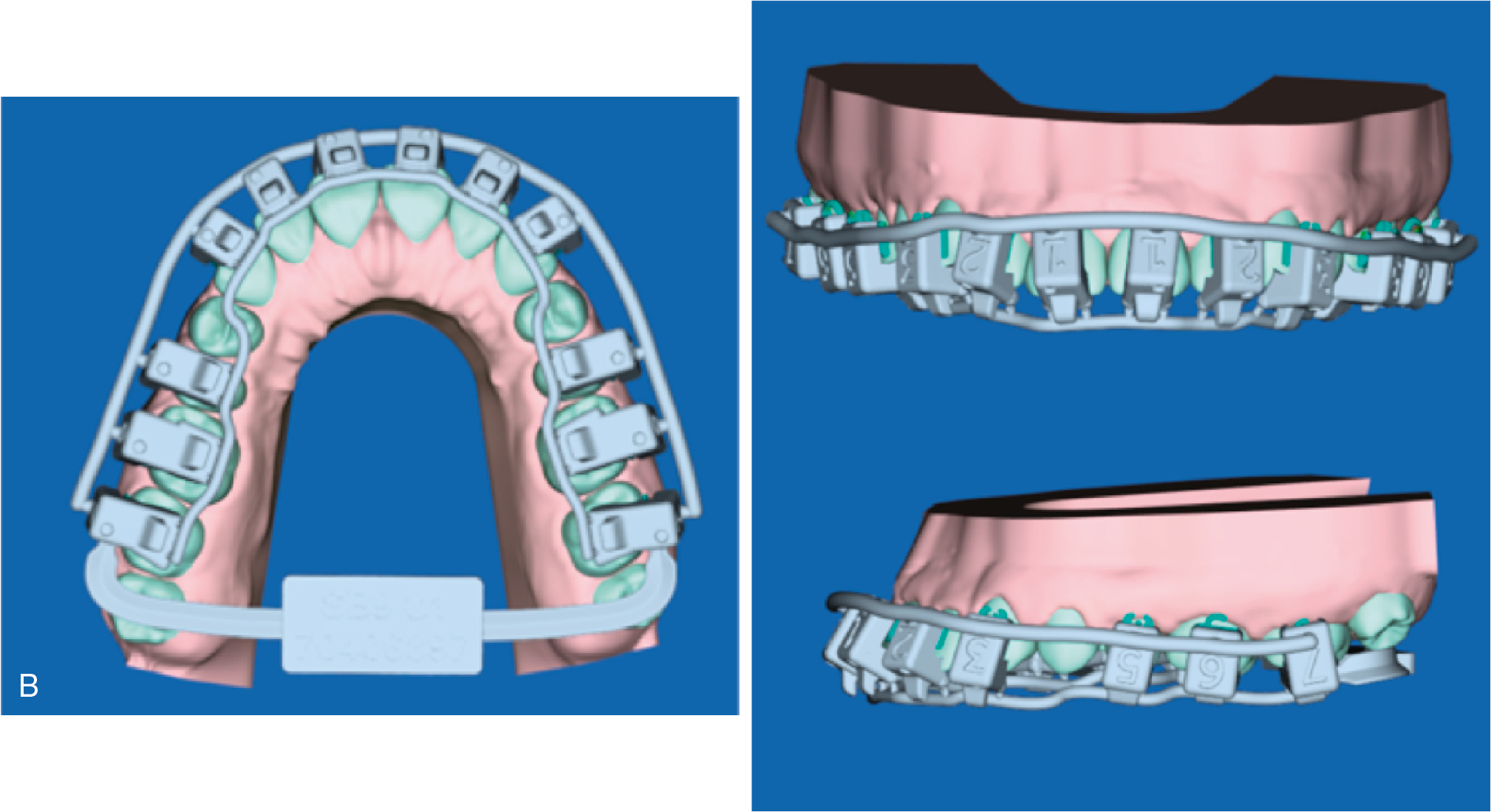
Indirect bonding is not new, and there are many excellent techniques using manual placement of brackets on models followed by transfer of the brackets to teeth by using plastic trays. The process can be very time consuming and costly. With CAD/CAM technology, brackets are placed virtually on a digital model, and then a transfer jig is printed with a 3D printer. The setup time is greatly reduced, and the cost of printing the transfer jigs are a fraction of that of manual laboratory procedures. To keep the time needed with the cheek retractors to a minimum, dental office staff can easily attach the brackets to the jigs and add the bonding composite before preparing teeth. Fig. 18.4 shows an example of a SureSmile bonding setup and placement.
Presurgical orthodontic preparation using suresmile
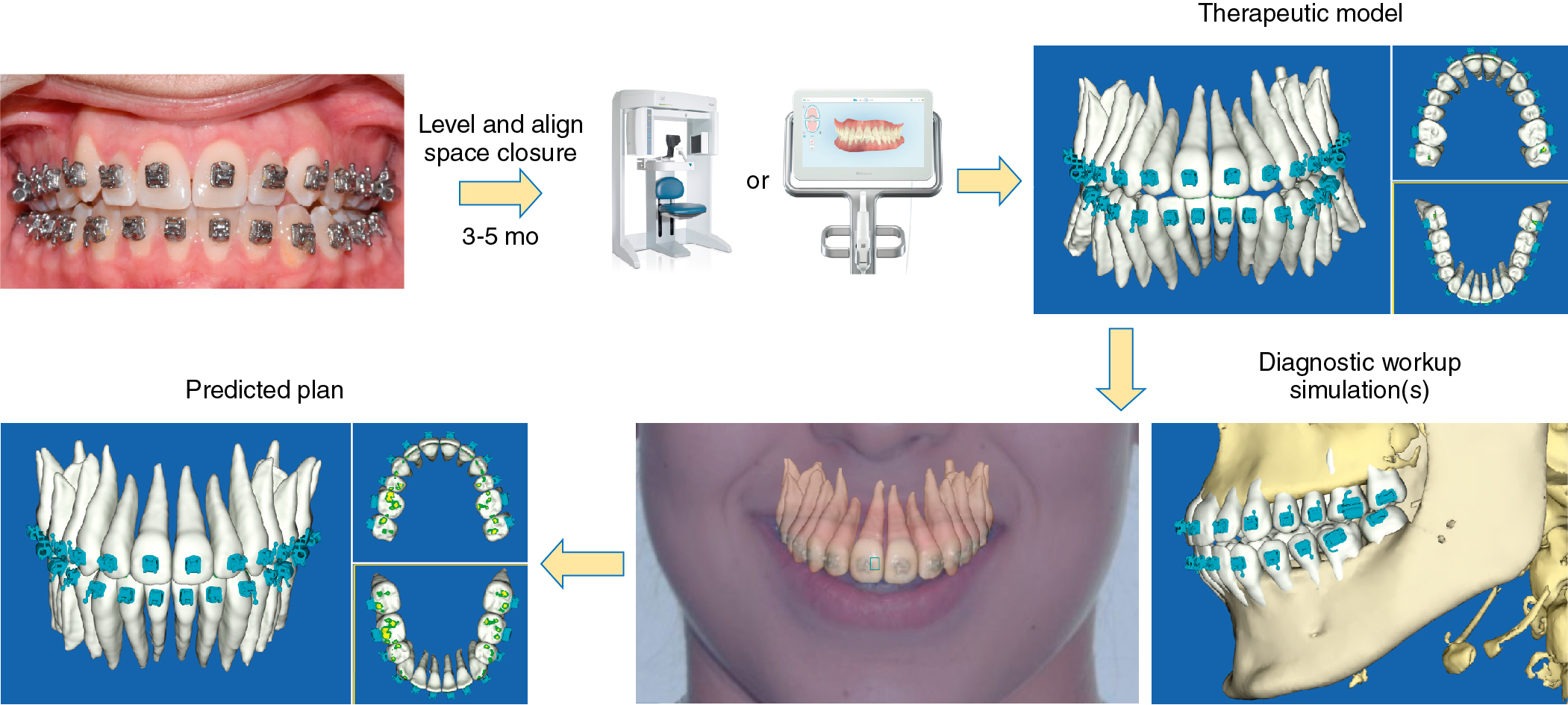
The patient in Fig. 18.5 presented with significant facial skeletal asymmetry as a result of unilateral condylar hyperplasia. This unilateral mandibular growth resulted in a class III occlusal relationship and an anterior crossbite. Skeletal surgery is necessary to restore the facial symmetry. The goal of orthodontic treatment would be to align and coordinate the arches so that the post surgical occlusion fits evenly in a Class I position with the dental midline coincident with the facial midline. Brackets were placed, and initial leveling was accomplished with light flexible wires similar to conventional mechanics. After a few months, a SureSmile therapeutic scan was performed, with a full-height CBCT scan to capture root regulations and bracket positions. The therapeutic scan was used to generate a simulation of the surgical and orthodontic outcomes ( Fig. 18.6 ).