Adipose Excess
Jessica Savas
Girish S. Munavalli
BACKGROUND
Societal attitudes and pressures to achieve the “ideal” human form are at an all-time high, and this is likely due to advancing technologies and the advent and explosive rise of social media.1 According to the Cosmetic Surgery National Data Bank Statistics annual report compiled by the American Society for Aesthetic Plastic Surgery, Americans spent more than 15 billion dollars on both surgical and nonsurgical cosmetic procedures in 2017 for the first time in history.2
Seemingly in contrast to this intense focus on health and beauty, obesity has more than doubled since 1980, and in 2014, over 1.9 billion adults were considered overweight with more than 600 million of these individuals with a body mass index (BMI) considered obese. According to the World Health Organization, obesity and overweight are defined as “abnormal or excessive fat accumulation that presents a risk to health.” Overweight and obesity are risk factors for a multitude of chronic diseases, including cardiovascular disease, diabetes, and cancer, and is a leading cause of preventable, premature death.3,4 In addition to having a negative impact on health, excess adiposity is of major aesthetic concern, and liposuction tops the list of the most commonly performed cosmetic procedure in both men and women for the last 5 years.2 Body contouring or sculpting is defined as the use of surgical or noninvasive techniques to modify the appearance of the body and is rapidly becoming one of the most requested nonsurgical aesthetic procedures in the United States.5
PRESENTATION
Patients present with a complaint of unwanted or excessive fat, often in select areas on the body. Common areas of concern include the abdomen, flanks, submentum, bra area, hips, and thighs.
DIAGNOSIS
Clinical Diagnosis
Adipose tissue excess may be diagnosed using a number of different methodologies, including physical
examination, circumference measurements, caliper measurements, BMI calculations, and ultrasound and computed tomography (CT)/magnetic resonance imaging (MRI).
examination, circumference measurements, caliper measurements, BMI calculations, and ultrasound and computed tomography (CT)/magnetic resonance imaging (MRI).
Laboratory Workup
The standard laboratory workup for adipose excess or obesity includes a fasting glucose and lipid panel, liver function and thyroid function tests, and hemoglobin A1C.
Diagnostic Measurements
The degree of fat may be evaluated by BMI, waist circumference (WC), and waist/hip ratio (WHR).
Body Mass Index. BMI is calculated as weight/height, and although it is correlated with fat, it does not distinguish between fat and lean body mass.
Circumference Measurements. Circumferential tape measurements are taken at the waist and the hip. The WHR is the most widely used index of regional adipose tissue distribution.6 The WC is the minimal measurement at the umbilicus; hip circumference (HC) is the widest measurement at the hips and buttocks. The threshold values of WHR are 0.85 for women and 0.95 for men; higher values are indicative of greater visceral fat and associated lipoprotein metabolism disorders, insulin resistance, and greater cardiovascular risk profile. To further assess the amount of abdominal visceral fat and associated cardiovascular risk, the WC taken midpoint between the lower border of the rib cage and the superior iliac crest and the sagittal diameter measured from a CT scan are recommended. WC >100 cm and sagittal diameter >25 cm on CT are indicative of higher levels of visceral fat and cardiovascular disease.6
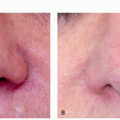
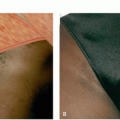
 FIGURE 6.1.1 Example of ultrasound measurement of fat reduction before treatment (A) and 4 months after (B). Note reduction in the thickness of the adipose layer. |
Caliper Measurements. Calipers are used to measure skinfold thickness, and raw values are used as an index of regional subcutaneous adipose excess.7 Skinfold caliper measurements may be taken at seven anatomic sites: triceps, suprailiac, thigh, chest, subscapula, midaxilla, and abdomen.8 The Siri formula is used to convert caliper measurements into body fat percentages.9,10
Ultrasound. Ultrasound has been validated as the most accurate and reproducible method for measuring adipose layer thickness following nonsurgical fat reduction11,12 (Figure 6.1.1). Ultrasound measurement reproducibility is very high for both subcutaneous and intra-abdominal fat thickness and highly correlated with CT adipose tissue determinations.
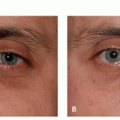
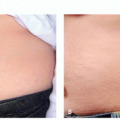
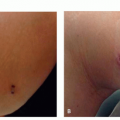
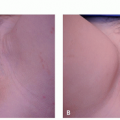
Standardized Digital Photography. Digital photography is a useful adjunct to ultrasound to monitor volume reduction and changes in body contour. Every effort should be made to create consistency between photos by controlling background, lighting, camera distance, and angle, as well as patient positioning. Serial photographs taken at baseline, with each treatment session and several weeks or months after completion of
the final treatment can provide a side-by-side comparison that is helpful for both patient and physician evaluation of results.
the final treatment can provide a side-by-side comparison that is helpful for both patient and physician evaluation of results.
Histopathology
Ultrasound, CT, and MRI findings are most often used to make the diagnosis and for monitoring of changes rather than skin biopsy.
Subtypes
Supra (pre) platysmal
Sub (post) platysmal
Abdominal subcutaneous fat
Visceral fat
On average, supraplatysmal fat represented 44.7% of the fat in the neck, the subplatysmal fat represented 30.7%, and the submandibular gland represented 24.5%. The very deep fat was scant, representing less than 1% of the fat in the neck.13 Clinical observation suggests that the normal aging process may lead to some atrophy of the intermediate (subplatysmal suprahyoid) fat layer. This is clinically relevant and suggests judicious treatment of intermediate (subplatysmal) fat in the youthful neck, to avoid possible contour deformity in later life.14
Differential Diagnosis
Hypothyroidism
Edema/ascites
Cushing syndrome
Insulinoma
Acromegaly
Lipodystrophy (see chapter 6.3)
Polycystic ovary disease
Pregnancy
Genetic syndromes (Prader-Willi, Börjeson-Forssman-Lehmann, Fröhlich, Bardet-Biedl, Cohen)
Iatrogenic/medication-induced (neuroactive medications, glucocorticoids, insulin)
Hypogonadism
PATHOGENESIS
To understand adiposity in disease states and the technologies employed for fat reduction, one must have a working knowledge of the anatomy and biology of fat as well as its role in normal human physiology.
Adipocytes are spherical, lipid-filled structures that are organized within the adipose tissue (Figure 6.1.2). Adipose tissue comprises primarily blood vessels, nerves, fibroblasts, and adipocyte precursor cells called pre-adipocytes. Mature adipocytes account for only one-third of the mass of adipose tissue. Collections of mature adipocytes comprise a fat lobule that is supplied by adjacent capillaries and nerves. The 2 major subdivisions of adipose tissue are visceral and subcutaneous fat. These differ not only by anatomic location but also by physiologic activity.15
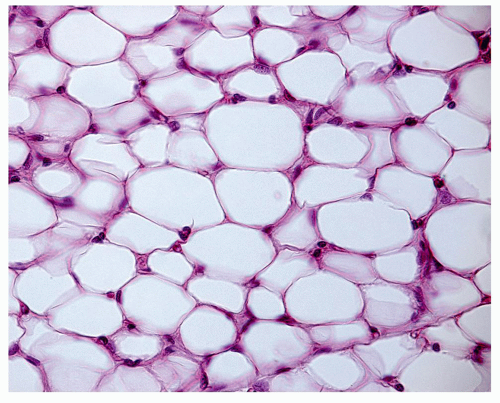 FIGURE 6.1.2 Adipose cell histology at 40× magnification, showing the pink cell membranes with darker, circular nuclei in the periphery of the cell. |
Adipose tissue is considered an endocrine organ because of its ability to secrete biologically active molecules called adipokines. Adipokines play a role in regulating glucose and lipid metabolism, insulin sensitivity, appetite, and satiety, as well as regulate immune and endothelial cell functions. With fat excess and obesity, adipokine profiles become dysfunctional resulting in insulin insensitivity and chronic systemic inflammation.16
Adipose tissue has a remarkable capacity for massive volume change. The adipose tissue mass is 9% to 18% of body weight in a lean adult man and 14% to 28% in women. In weight gain, adipocytes undergo hypertrophy or increase in size until a “critical mass” is achieved at which point adipocyte hyperplasia, or the formation of new fat cells, termed “adipogenesis,” occurs. The point at which this critical mass occurs varies by anatomic site and gender.16
The distribution of excess fat is obvious when comparing individuals of normal body weight with obese individuals (Figure 6.1.3). The proportion of body fat as well as the distribution of fat stores differs significantly between men and women. This discrepancy is rooted in the metabolic and hormonal differences between sexes and from an evolutionary biology perspective can likely
be explained by the metabolic demands of pregnancy and lactation. All other variables remaining equal, women have greater adipose stores than men and this appears to be true across all races and cultures.
be explained by the metabolic demands of pregnancy and lactation. All other variables remaining equal, women have greater adipose stores than men and this appears to be true across all races and cultures.
 FIGURE 6.1.3 MRI shows the difference between an obese woman on the left and a woman with normal body weight on the right. The yellow areas are areas of fat distribution. |
With regard to body fat distribution, women have greater adipose stores in the thighs and buttocks, whereas men preferentially accumulate fat stores in the abdomen.17 Differences in fat metabolism between men and women seem to parallel fat distribution. Women are more metabolically inclined to store fat than men; however, women are more likely than men to preferentially utilize fat as an energy source during periods of sustained exertion. Both fat distribution and metabolism are highly influenced by sex hormones. Testosterone increases lipolysis, and increasing circulating testosterone decreases total adipose tissue in men. Conversely, estradiol drives fat deposition via binding to the α estrogen receptor in subcutaneous fat and upregulating α-2A-adrenergic receptors, which results in decreased lipolysis.18
Studies have shown that the number of adipocytes is the major determinant of adipose tissue mass in adults. An individual’s number of fat cells remains fairly constant throughout a person’s lifetime.19 As previously mentioned, in states of caloric excess, new adipocytes may form through the process of adipogenesis; however, the converse is not true. Even after marked weight loss is achieved through diet and exercise, adipocyte volume may decrease but fat cell number remains unchanged. Certain anatomic locations have been shown to be more resistant to volume reduction, such as the abdomen and flanks.20 Ultimately, it is for these diet- and exercise-resistant areas of focal adiposity that patients seek surgical or noninvasive methods of fat reduction.
TREATMENT
Algorithm 6.1.1 presents the workup, diagnosis, classification, and treatment of adipose excess disorders.
Patient Selection
The ideal candidates for noninvasive body sculpting or contouring procedures are patients with focal adiposity that is diet and exercise resistant. A thorough medical history and physical examination of potential treatment areas should be completed, and smoking and alcohol cessation should be encouraged when applicable. A psychological assessment to elicit the presence of an underlying mental health disorder such as body dysmorphia is mandatory before all cosmetic procedures as these patients are unlikely to be satisfied with any intervention. A thorough discussion of and, when necessary, adjustment to a patient’s expectations in regards to outcome is paramount before pursuing noninvasive fat reduction. Results are variable, and although visible and sometimes significant focal reduction is possible, results are not equivalent to surgical fat reduction and most noninvasive techniques do not offer improvement in skin laxity, which is frequently needed in this patient population.
Medical
Diet and Exercise
Diet and exercise are the 2 most basic medical therapies for fat excess. Once medical disorders contributing to weight gain, such as hypothyroidism, have been ruled out by an internist, referral to a nutritionist is recommended. Exercise through a trainer or exercise class is also recommended.
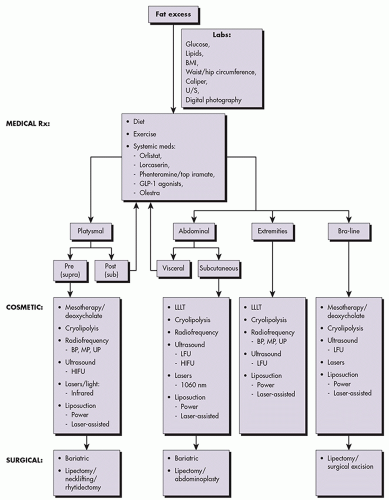 ALGORITHM 6.1.1 Treatment algorithm for adipose excess disorders. BP, bipolar; HIFU, high-intensity focused ultrasound; LFU, low-frequency ultrasound; MP, monopolar; UP, unipolar. (Courtesy of Macrene Alexiades, MD, PhD.). |
Systemic Medications
Only a few oral medications are approved by the US Food and Drug Administration (FDA) for the treatment of obesity and intended for use in patients with BMI >30 kg/m2 or >27 kg/m2 with a comorbidity risk factor (eg, diabetes, hypertension).21 These drugs include orlistat, lorcaserin, combination phentermine and topiramate, and combination bupropion and naltrexone. A newer drug class of glucagon-like peptide (GLP)-1 agonists, previously used for diabetes, is emerging as effective weight loss medications. They should be used in concert with diet, exercise, and behavior modification. After 12 weeks of use, 5% or more weight loss should be expected or the medication discontinued. An FDA warning has been issued regarding over-the-counter weight loss and “dietary” supplements. In 2015, the FDA banned amphetamine-like stimulant BMPEA, also known as acacia rigidula.
A fat substitute olestra, a sucrose polyester with 6 to 8 fatty acid side chains, is approved as a dietary supplement. Olestra is too large to be hydrolyzed and is excreted without being absorbed. Supplementation with fat-soluble vitamins is recommended.
Cosmetic
In spite of the efficacy of surgical fat reduction, there has been a significant demand for treatments that offer visible results after a few sessions with little to no downtime, thus the rapid development and refinement of noninvasive fat reduction methods.
Noninvasive Fat Reduction
The currently available noninvasive techniques used to accomplish fat reduction can be divided into 4 main categories: low-level laser therapy (LLLT), cryolipolysis, radiofrequency (RF), and ultrasound. The latter category can be further subdivided into low-intensity/low-frequency ultrasound and high-intensity focused ultrasound (HIFU).
Low-Level Laser Therapy. LLLT has been used for decades as a noninvasive, nonthermal technique to reduce pain and inflammation as well as to stimulate healing and wound regeneration.22,23 Over the past decade, LLLT has been examined as an adjuvant to other fat reduction methods as well as monotherapy for noninvasive body contouring. The process by which LLLT accomplishes adipocyte injury has yet to be fully elucidated. The prevailing theory has centered on the ability of the 635-nm-wavelength lasers to penetrate to the level of the subcutaneous fat and cause pore formation in the adipocyte cell membrane with subsequent release of lipids into the interstitial space.24 The extravasated lipid is then removed via the lymphatics with an overall reduction in volume. Subsequent studies looking at pore formation could not replicate these findings, and the mechanism of action of adipocyte reduction by LLLT thus remains somewhat controversial.25 The Zerona LipoLaser (Erchonia Medical, Inc, Melbourne, FL USA) was the first device to be granted FDA approval in the United States for noninvasive circumferential reduction of the waist, hips, and thighs. This device features 5 rotating diode laser heads that each emit 17 mW of 635 nm laser light.26
Protocols. Well-designed studies and clinical trials have demonstrated an average reduction of 3.51 to 5.17 in circumferential measurements across the waist, hips, and thighs after only 2 weeks.27,28 Current standard calls for 6 to 12 treatments, up to 40 minutes, delivered 48 hours apart over 2 weeks. The number of treatment sessions is often dictated by the patient’s body habitus and fat reduction needs.
Adverse Events. LLLT is extremely well tolerated with almost no reportable adverse effects, although thermal injury can theoretically occur. Patient dissatisfaction is higher with this modality compared with other devices that will be discussed, likely because of unrealistic patient expectations when LLLT is used as monotherapy.
Mesotherapy/Deoxycholate. Injection of substances into the mesodermally derived subcutaneous tissues, termed mesotherapy, was first described in the 1950s when Dr Pistor attempted to treat asthma using injectable procaine.29 Today, mesotherapy is primarily employed for cosmetic purposes, namely, local fat reduction.
Cosmetic fat reduction via subcutaneous injection is accomplished through 1 of 2 mechanisms: lipolytic stimulation or ablative mesotherapy. Lipolytic stimulation relies on the premise that an individual’s fat distribution is related to the lipolytic threshold of fat cells, which varies based on gender and anatomic location. By injecting substances that reduce the lipolytic threshold, a temporary decrease in focal adiposity may be accomplished.30,31 Ablative mesotherapy is the more commonly employed modality by which detergents are used to achieve permanent destruction of adipocytes. In 2015, a
synthetic form of deoxycholic acid, ATX-101 (Kybella), was approved by the FDA as the first pharmaceutical intervention for submental fat reduction.
synthetic form of deoxycholic acid, ATX-101 (Kybella), was approved by the FDA as the first pharmaceutical intervention for submental fat reduction.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


