BACKGROUND
Actinic keratoses (AKs) are common epidermal dysplastic lesions that typically present as scaly or keratotic macules or papules with a diffuse erythematous base in fair-skinned individuals at increasing age. Resulting from chronic exposure to ultraviolet radiation (UVR), AKs are predominantly located in sun-exposed skin such as the face, scalp, and dorsal arms and hands.
The incidence of AKs increases with patient age, and it is recognized as the most frequent dermatologic diagnosis in patients above 60 years of age. Studies find prevalence rates in patients above 60 years ranging between 19% and 25% in the United States and 23% in a UK population,
1,
2 whereas the highest prevalence of AKs is reported in Australia with up to 60% of patients having AKs.
3 In men aged 65 to 74 years, a study found AK prevalence rates at 55% and 19% in patients with high and low sun exposure, respectively, and reflects an increased incidence of AKs in patients with high cumulative UVR exposure.
4AKs are premalignant intraepidermal keratinocyte neoplasia that can progress into invasive squamous cell carcinoma (SCC).
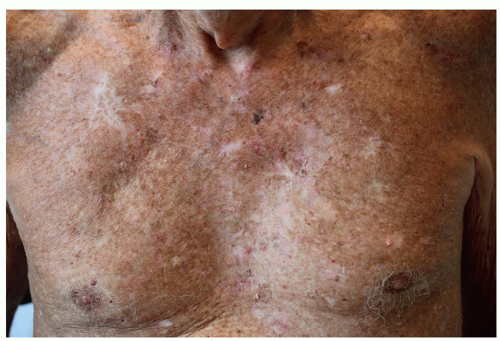
5The reported risk of each AK undergoing malignant transformation to SCC varies considerably and ranges from 0.025% to up to 2% per year, although the majority of studies that also include larger patient sets find transformation rates between 0.075% and 0.96% per year. The risk of SCC development is significantly greater in immunosuppressed organ transplant recipients (OTRs) and in patients with field cancerization, comprising photodamaged skin with multiple AKs, subclinical nonvisible lesions, and previous keratinocyte cancers.
6,
7 A patient with typical field cancerized skin is illustrated in
Figure 5.1.1.
PATHOGENESIS
Chronic exposure to UVR results in photoaging and skin cancer development. The main source of UVR is solar UVR, consisting of UVB (280-320 nm) and UVA (320-400 nm). For AK and SCC development, studies suggest a strong, positive association with accumulated UVR exposure, whereas exposure patterns are considered of less importance.
14 UVR exposure induces direct formation of photoproducts as well as indirect oxidative damage that both result in structural damage to skin DNA and RNA.
15 If the photoproducts are not repaired, they may induce transition-type mutation such as cytosine to thymine (C → T) in tumor suppressor genes, including p53, p16INK4a, p14ARF, and PTEN.
16 Accumulated mutations in tumor suppressor genes, especially p53, are typically detected in photodamaged skin and may result in dysplastic transformation, proliferation of atypical keratinocytes, and development of AKs and invasive SCC.
17,
18The major risk factors for AK development are male sex, age >70 years, baldness, photodamaged skin, and a high cumulative UVR exposure from sun exposure or tanning beds.
19 Individuals with fair skin types, including Fitzpatrick skin types I and II, possess a higher risk of AK development as these patients are more sensitive to UVR exposure owing to a lower constitutive skin pigmentation. Other risk factors include history of smoking and outdoor
work, whereas the number of nevi has not been related to AK prevalence.
20 Furthermore, studies have found that coexisting infection with human papilloma virus (HPV) is associated with AK and SCC initiation, although the exact mechanism is not fully established.
21,
22A few genetic syndromes are associated with an increased risk of AK and SCC development, including xeroderma pigmentosum, oculocutaneous albinism, and epidermodysplasia verruciformis. In xeroderma pigmentosum, defects in the DNA repair mechanism, nucleotide excision repair, greatly accelerate UVR-induced AK and SCC development. In albinism and epidermodysplasia verruciformis, SCC development occurs from lack of pigmentation and widespread colonization with multiple oncogenic HPV types, respectively.
Organ Transplant Recipients
Immunosuppressed solid organ transplant recipients have an especially increased risk of AK and SCC development that is up to 40 to 250 times greater than that in the general population. The continuous immunosuppression reduces the repair mechanism of UVR-induced DNA damage and potentiates the carcinogenic effects of UVR.
23 Specifically, azathioprine and other thiopurines have been recognized as DNA photosensitizers in immunosuppressant treatment and are associated with an increased risk of AK and SCC occurrence in patients with hematologic malignancies, inflammatory bowel disease, and rheumatic diseases.
24 As a consequence, transplant recipients experience onset of AKs earlier in life and usually develop multiple lesions compared with age-matched immunocompetent patients.
25 Transplant recipients are prone to develop numerous AK lesions in sun-exposed areas, which can, in conjunction with SCC, cause significant morbidity among patients. The prevalence of AKs increases significantly with increasing time after transplantation corresponding to longer duration of immunosuppressant therapy. Furthermore, patients receiving thoracic organ transplantation have a higher risk of SCCs because of higher immunosuppressive load. Daily use of sun screen, regular cutaneous screening visits, and aggressive treatment of AKs are important assets to prevent SCC development in these high-risk patients.
Natural Development of AKs
If left untreated, AKs have the potential to undergo 1 of 3 scenarios: (1) undergo spontaneous remission, (2) remain stable, or (3) progress into invasive SCC with the potential to metastasize.
Spontaneous regression of single AK lesions was reported to be 20% to 30% per year in a review, whereas one study found that up to 63% of AKs spontaneously resolved.
26 However, in field cancerized skin, spontaneous regression of a complete AK-field was observed in only 0% to 7% of patients and 57% of AKs recurred following spontaneous clearance.
26 These data indicate that inadequately treated AKs are dynamic but act as a chronic condition with low chance of sustained spontaneous regression, especially in field cancerized skin.
26,
27The risk of an AK evolving into invasive SCC has, in prospective studies, been reported at rates of 0.075% to 0.96% per year.
28 Over a 10-year period, SCC development has been reported up to 13% to 16% in patients with untreated AKs. The risk of SCC transformation seems higher in patients with clinical hyperkeratotic AK.
29 The transformation from AK to SCC may be associated with a period of rapid inflammation, which subsides upon SCC development that may be caused by SCC-mediated suppression of the immune system’s tumor response.
27 Additionally, AKs have been associated with an increased overall risk of skin cancer, including melanomas, possibly because AK indicates a previous or current extensive sun exposure.