Key points
- •
Understanding anatomic changes associated with age is essential.
- •
Pre-operative assessment of eyelid tone and tarsoligamentous laxity.
- •
Resect skin, muscle and fat in a conservative fashion.
Introduction
The eyes and periorbital tissues are paramount in facial beauty. Unfortunately, they are also one of the first areas to show signs of aging. Because of this, blepharoplasty has become one of the most commonly requested and performed aesthetic procedures. Despite being considered a straightforward procedure, upper eyelid surgery has gained much interest with the recent focus on periorbital and brow aging. Lower blepharoplasty, on the other hand, has been referred to as one of the more challenging procedures in plastic surgery. With the increase in the number of blepharoplasties performed each year, there is also an increase in the incidence of postblepharoplasty complications. The recent popularity of the transconjunctival technique for lower lid rejuvenation when there is no excess skin has been a response to the incidence of lower lid malpositioning (retraction, ectropion, and scleral show). Although more conservative, it does not eliminate the risk of lid malposition, as some original publications have suggested. Because of these questions an individualized approach, focused on the patient complaints and characteristics, is preferred today.
Upper lid surgery
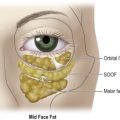
The upper eyelid problem is compounded by aging, because the brows tend to descend and progressive relaxation of the tissues tends to occur, leading to larger and larger folds of the upper eyelid. Traditional blepharoplasty has often involved the excision of both lax skin and muscle with excessive removal of fat. It is the authors’ belief that a conservative approach is sufficient for most patients. The evaluation of the upper eyelid must include an evaluation of the eyebrow. Brow ptosis should be corrected to achieve repositioning of heavy eyebrow skin, which may be compensated by frontalis action to keep the eyebrows above the orbital rim. Aging causes the eyebrow fat to descend over the upper lid, giving it a full appearance. Special attention should be given to the bulging of the lateral third of the eyebrow, which could consist of a fat structure located between the orbicularis muscle and frontal bone denominated retro-orbicularis oculi fat (ROOF) and/or projection of the supraorbital bone rim.
Lower lid surgery
Several different approaches to the rejuvenation of the lower lid and midface have been proposed. Traditionally, lower lid blepharoplasty has been confined to a choice of skin or skin–muscle flap transcutaneous blepharoplasty. The senior author has chosen a more individualized approach based on variations in anatomical features and patient goals. A transcutaneous skin–muscle flap lower blepharoplasty is reserved for cases with mild periorbital aging with better eyelid skin. A transcutaneous skin flap, however, is the procedure of choice in cases where excessive skin is present, with visible and marked wrinkles, meaning more skin needs to be excised. Canthal support is performed whenever tarsoligamentous laxity is present.
Patient selection
It is the authors’ belief that by identifying the anatomical abnormalities and choosing the proper techniques, surgeons can achieve satisfactory eyelid rejuvenation providing a natural look, while preserving function and minimizing complications. Recognition of the specific features of patients’ aesthetic concerns during pre-operative evaluations serves to focus on the patients’ understanding and expectations of realistic surgical results. The patients are first clinically classified as having mild or advanced eyelid and midface aging. An interesting classification of midface aging was first published by Hester and Codner. This classification clinically categorized midfacial aging as type I, aging confined to lower lid; type II, lower lid aging with minimal descent of lid/cheek junction (midfacial aging confined to upper midface); type III, lower lid aging with descent of lid/cheek junction and malar prominence, skeletalization of the orbital rim, and deepening of the nasolabial fold; and type IV, characteristics of type III with deepening of the nasojugal groove and/or presence of a ‘malar bag’. Type I patients are good candidates for a more conservative approach such as the transcutaneous skin-muscle flap blepharoplasty. Type II and maybe III are good candidates for a skin flap blepharoplasty with orbicular redraping. More advanced cases of aging such as some type III and IV may require a midfacial procedure.
In addition to the degree of aging, many different conditions must be observed in the blepharoplasty patient. The Oriental upper eyelid for instance should be addressed with specific goals. The full upper lid look and the lack of fold should be considered. Another common presentation is the secondary case. Secondary blepharoplasty has more pitfalls and potential problems than a primary case. The margin for error is exceedingly small. Because of that, secondary eyelid surgery should be undertaken only after careful evaluation and accurate diagnosis of the cause of the deformity.
Eyelid tone
The eyelid is characterized by an almond-shaped horizontal palpebral fissure with an upward slant from the medial to lateral canthus. The lower lid is positioned 1 mm above the lower edge of the limbus with the subject in neutral gaze. Eyelid tone is characterized by an absence of tarsoligamentous laxity and skin excess. Whenever tarsoligamentous laxity is present lateral canthal anchoring is mandatory. The degree of laxity is used to determine the type of lateral canthal support. A lateral canthopexy is usually performed for moderate lid laxity, which is considered to be less than 6 mm of lid distraction away from the globe in the forceps induced lid distraction test. Certain morphological features, such as an inadequate infraorbital rim, maxillary hypoplasia, and orbital proptosis, might make patients more prone to developing lower eyelid retraction and subsequent dry eye. Patients with prominent eyes are at higher risk for lid malposition and require additional vertical support of the lateral canthus. While the standard position of the lateral canthopexy suture is at the lower level of the pupil, patients with prominent eyes may require additional vertical positioning of the lateral canthal support suture at the superior aspect of the pupil.
Indications
Evidence of periorbital aging is the primary indication for a blepharoplasty procedure. The most common cosmetic problems are fat herniation of both upper and lower eyelid, excess skin of the upper eyelid and wrinkling of the lower eyelid skin. Alterations in the quality of skin, lengthening of the lower lid margin, orbicularis muscle hypertrophy and other aesthetic conditions, such as scleral show or prominent globes, are also encountered and may be considered reasonable indications for these procedures. It is the authors’ belief that patients with mild eyelid aging (aging confined to lower lid or lower lid aging with minimal descent of lid/cheek junction) are good candidates for a transcutaneous skin muscle flap lower blepharoplasty. Usually, these patients do not need canthal support. Patients with moderate to severe signs of orbital aging should be addressed with transcutaneous skin flap with orbicular suspension and redraping lower blepharoplasty. In these patients, a canthal support procedure is usually indicated. Excess skin and muscle, defined by the presence of redundant lower eyelid anterior lamella, is also approached with a skin muscle flap lower blepharoplasty. With regard to the upper lid, a more standardized procedure is usually performed as described below.
Operative technique
Pre-operative preparation
Pre-operative evaluation includes a thorough ophthalmic history, including prior operations, ocular trauma, allergies, dermatological disorders, dry eyes, or other relevant conditions such as Graves’ disease. Patients with specific dry eye complaints undergo pre-operative visual acuity testing, Schirmer’s test or tear production tests, as indicated. Patients are questioned regarding any bleeding disorders or the recent use of procoagulant medications, and standard perioperative medications and protocols are suggested. Pre-operative photographs are obtained, including upward gaze (which allows a more complete visualization of the fat projection), eyes open, eyes closed, squinting, and up-close lateral views.
Evaluations include questioning the patients regarding their aesthetic concerns and correlating those concerns with anatomical findings. The skin condition, lower eyelid position, muscle hypertrophy, and fat herniation are specifically evaluated and discussed. The relationship of the lower eyelid margin to the inferior corneal limbus, scleral show, orbital proptosis, inadequate infraorbital rims, orbicularis muscle hypertrophy, and lateral canthal rhytids are also noted. The upper eyelid is evaluated to assess concomitant eyebrow descent. Informed consent was obtained from all patients.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


