The authors developed an anonymous, Web-based survey instrument available globally, and collected data from 171 pemphigus vulgaris (PV) patients to assemble epidemiologic data pertaining to an extensive set of clinical parameters in demographically diverse populations. The results showed female predominance, prevalent onset of disease in the fifth decade of life, and a strong correlation of PV with thyroid disease and type 1 diabetes in patients and family members. Most patients have a history of either mucosal-only or mucocutaneous lesions, but numerous patients self-report cutaneous lesions only, without previous or concurrent mucosal lesions, especially in the non–North American PV population.
Pemphigus vulgaris (PV) is a prototypic organ-specific autoimmune disease characterized by the presence of circulating autoantibodies against desmoglein (Dsg) 3, and in some cases Dsg1, causing blister formation in the skin and mucous membranes. Previous studies have reported the incidence of PV to range from 0.076 per 100,000 person-years to 5 per 100,000 person-years. While PV is rare, for those affected the disease presents a lifetime physical, emotional, and monetary burden. There is no cure, and only palliative treatment, mostly based on general immunosuppression, is available at this time.
As with all autoimmune diseases, the etiology of PV is multifactorial, with complex interactions of genetic and environmental factors contributing to disease development and exacerbation. Although there is a strong link to the HLA DR4 and DR6 associated alleles, specifically DRB*0402 and DQB1*0503, the vast majority of individuals carrying these PV associated alleles do not develop PV. There are limited data regarding additional genetic or environmental factors relevant to the initial expression of disease and the subsequent disease course in the current literature, and to date there are no published national or international registries for autoimmune bullous skin diseases with large databases of clinical information.
Comprehensive demographic and epidemiologic data collection can potentially help to elucidate questions of disease etiology. To date, studies regarding the epidemiology of PV have focused on narrowly defined demographic populations, and the data collected have typically been restricted to a limited set of disease characteristics. To bridge this gap, and to overcome limitations in patient recruitment due to the rarity of PV, the authors developed an anonymous, Web-based survey instrument available globally. It has been reported that 80% of American adults have used the Internet to search for health-related information; as such, the Internet is an increasingly useful tool to conduct research. In fact, anonymous Web-based questionnaire techniques are increasingly being used to assess patient attitudes toward medical care and to collect disease-relevant medical history data in an expedient and efficient manner. In this study, self reported demographic and epidemiologic data pertaining to a wide range of clinical parameters was collected, including disease onset, phase, and morphology, comorbid disease, family history of autoimmunity, and possible trigger factors in PV.
Two hundred and fifty-one patients affected by a variety of autoimmune blistering conditions took part in the online survey, of which 171 reported a diagnosis of PV. The study supports the viability and usefulness of an online mechanism for the investigation of a rare disease. The authors have successfully collected a comprehensive set of disease-relevant data that provide insights into disease expression and disease association.
This newly developed survey tool for blistering skin disorders facilitates patient participation across broad demographic areas, and has the potential to be used to follow patients longitudinally in order to track disease development over time.
Materials and methods
Online Study Tool
To collect epidemiologic data from a diverse group of people affected by pemphigus and pemphigoid, the authors devised a comprehensive, anonymous, online survey available globally to all individuals with Internet access and English language proficiency. The Longitudinal Study Engine (LSE) hosted at the Biomedical Research & Informatics Core at Michigan State University was used. The LSE supports a fully anonymous data collection protocol and can track multiple logins as separate entries for a given patient identification number, hence providing the possibility of longitudinal data analysis.
Patient Recruitment
The study was approved by Michigan State University’s Institutional Review Board (IRB, X06-943, status exempt). Patients were recruited to participate in the online questionnaire primarily by the International Pemphigus and Pemphigoid Foundation (IPPF) research Web site link to the study, and subsequent patient promotion through Internet support group forums and message boards. Other methods included a link on the homepage of the Division of Dermatology and Cutaneous Sciences, Michigan State University, and direct contact with patients who had previously expressed interest to be contacted when new research projects became available.
Data Acquisition
After logging into the survey, patients were prompted to create a username, accept a consent form, and review a short instructional page on how to use the survey. Depending on the question, answer choices included yes-or-no options, drop-down boxes, or open text fields. The entire survey requires approximately 15 to 20 minutes to complete. LSE is housed on 2 Dell PowerEdge 2850 (Dell Inc, Round Rock, TX, USA) servers hosted in the Michigan State University HealthTeam Data Center. The data center is physically and logically controlled to meet National Institute of Standards and Technology definitions of HIPAA (Health Insurance Portability and Accountability Act of 1996) security.
Data Analysis
Participants were first grouped by diagnosis (PV, pemphigus foliaceus, pemphigus vegetans, pemphigus erythematosus, IgA pemphigus, bullous pemphigoid, herpes gestationis, cicatricial pemphigoid, ocular pemphigoid) and descriptive statistics for the largest cohort, PV, are reported as frequencies and percentages. In a subsequent analysis within the PV population the authors compared North American and non–North American populations. To investigate whether the distribution of categorical variables differs between populations, chi-square or Fisher’s exact test values and unadjusted odds ratios (OR) with 95% confidence intervals were calculated. All analyses were performed using SAS software, Version 9.1 (SAS Institute Inc, Cary, NC, USA). Because of the online nature of the survey, entries that failed to answer any questions and entries that only provided demographic information were removed. In addition, uninterpretable data were excluded from analysis.
Results
Study Population
A total of 251 pemphigus and pemphigoid patients were enrolled over a time interval of 8 months. The majority of patients reported a diagnosis of PV (n = 171), followed by cicatricial pemphigoid (n = 33), bullous pemphigoid (n = 28), pemphigus foliaceous (n = 25), ocular pemphigoid (n = 13), pemphigus vegetans (n = 2), IgA pemphigus (n = 1), paraneoplastic pemphigus (n = 1) and pemphigus erythematosus (n = 1). A majority of PV patients originated from North America (United States, n = 125; Canada, n = 11; Mexico, n = 1) while the remainder originated from Great Britain (n = 13), Israel (n = 7), the Netherlands (n = 4), India (n = 3), Australia (n = 2), Belgium (n = 1), Germany (n = 1), Greece (n = 1), Pakistan (n = 1), and Trinidad (n = 1). In this report the analysis is focused on the PV population.
Eighty percent of PV respondents to the survey reside in North America (United States, Canada, Mexico). Differences in genetic background, specifically HLA haplotypes in various ethnic groups, have been described in PV. Because genetic as well as environmental factors can potentially vary across geographic regions, the authors undertook an initial strategy to compare disease characteristics of North American PV (NAPV) patients with non–North American PV (non-NAPV) subjects. However, as few significant differences were detected in regards of demography (racial breakdown, see later discussion) and disease characteristics (history and development of lesion morphology, see later discussion), both populations were merged for most analyses.
Demography
The demographic breakdown of the PV populations participating in this study is shown in Table 1 . Of the 171 PV patients, 52 were male and 117 female, with a male to female ratio of 1:2.25. The mean age was 51.8 years, ranging from 25 to 80 years. Most patients identified themselves as Caucasian (n = 142, 83.0%), followed by Asian (n = 12, 7.0%), Hispanic (n = 6, 3.5%) and Black (n = 4, 2.3%). However, in the NAPV population, significantly more patients identified themselves as Caucasian than in the non-NAPV population (OR 13.14, 95% confidence limit [CL] 5.48–31.52, P <.001). Congruent with the fact that PV and the PV-associated HLA haplotype DRB1*0402 are highly prevalent in Ashkenazi Jewish populations, nearly one-half of the 171 patients in the study reported being Jewish (n = 74, 43.3%); of these 74, 58 (73.8%) reported Ashkenazi descent (see Table 1 ).
| PV (n = 171) | ||
|---|---|---|
| Age in years, mean (range) | 51.8 (25–80) | |
| Male/Female ratio | 1:2.25 | |
| n | % | |
|---|---|---|
| Sex | ||
| Male | 52 | 30.8 |
| Female | 117 | 69.2 |
| Race | ||
| White/Caucasian | 142 | 83.0 |
| Asian | 12 | 7.0 |
| Black/African American | 4 | 2.3 |
| American Indian/Alaskan Native | 1 | 0.6 |
| Native Hawaiian/Pacific Islander | 1 | 0.6 |
| Hispanic/Latino | 6 | 3.5 |
| Other | 5 | 2.9 |
| Jewish Descent | ||
| Jewish | 74 | 43.3 |
| Ashkenazi Jewish a | 58 | 73.8 |
a Ashkenazi Jewish descent is presented as raw number of patients and percent of Jewish participants within the Jewish subgroup (n = 74).
Disease Characteristics
To assess disease characteristics several defined clinical variables were evaluated: the age of onset of disease, the current phase of disease (active vs remittent), the morphology of lesions (mucosal-only vs mucocutaneous vs cutaneous-only), and lesion distribution. Because differences were found between NAPV and non-NAPV patients in terms of lesion morphology, data for both groups are listed in Table 2 .
| ALL PV (n = 171) | NAPV (n = 137) | non-NAPV (n = 34) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age of onset in years, mean (range) | 45.2 (17–74) | 45.2 (17–74) | 45.4 (23–61) | ||||||
| n | % | n | % | n | % | OR | CL | P value | |
|---|---|---|---|---|---|---|---|---|---|
| Disease Phase | |||||||||
| Active | 83 | 48.53 | 67 | 48.91 | 16 | 47.06 | 1.16 | 0.54–2.47 | .70 |
| Remittent | 83 | 48.53 | 65 | 47.44 | 18 | 52.94 | |||
| No response | 5 | 2.94 | 5 | 3.65 | 0 | 0 | |||
| History of Lesion Morphology a | |||||||||
| Cutaneous only | 19 | 11.59 | 12 | 9.16 | 7 | 21.21 | 0.37 | 0.13–1.03 | .0495 |
| Mucosal only | 37 | 22.56 | 28 | 21.37 | 9 | 27.27 | 0.71 | 0.30–1.70 | .44 |
| Mucocutaneous | 108 | 65.85 | 91 | 69.47 | 17 | 51.52 | 1.98 | 0.93–4.23 | .08 |
| Development of Lesion Morphology b | |||||||||
| Mucosal before cutaneous | 71 | 65.74 | 64 | 70.33 | 7 | 41.18 | 0.26 | 0.10–0.86 | .02 |
| Cutaneous before mucosal | 19 | 17.59 | 13 | 14.29 | 6 | 35.29 | 0.26 | 0.10–0.86 | .02 |
| No response | 18 | 16.67 | 14 | 15.38 | 4 | 23.53 | 3.27 | 1.03–10.39 | .04 |
a History of lesion morphology (all PV n = 164; NAPV, n = 131; non-NAPV, n = 33).
b Development of lesion morphology (all PV n = 108; NAPV, n = 77; non-NAPV, n = 13).
The average age of onset for disease in the combined (NAPV and non-NAPV) PV population was 45.2 years (range 17–74 years). The diagnosis of PV was confirmed by biopsy in nearly all participants (n = 168, 98%). In a considerable number of patients, however, the initial biopsy did not reveal the diagnosis of PV (n = 24, 14.0%). Of those who were initially misdiagnosed, the length of time that patients experienced symptoms before being correctly diagnosed ranged from 1 to 24 months (mean, 8 months).
Half of all PV survey respondents were in an active phase of disease (continuous presence of nontransient lesions), whereas the other half was in remission (no lesions or transient lesions only; transient defined as lasting less than a week) (see Table 2 ).
65.85% of patients reported a history of mucocutaneous lesions (n = 108), followed by a history of mucosal-only (22.56%, n = 37) and a history of cutaneous-only (11.59%, n = 19) lesions (see Table 2 ). Of note, the history of cutaneous-only disease morphology (ie, never had mucosal lesions) was significantly less frequent in the NAPV population (OR 0.37; 95% CL 0.13–1.03; P = .0495). Among participants who had experienced both mucosal and cutaneous lesions, a greater number manifested with mucous membrane lesions before the development of cutaneous lesions in both populations (65.7%, n = 71) than cutaneous before mucous membrane lesions (17.6%, n = 19), However, the percentage of NAPV patients who presented with mucosal lesions before cutaneous lesions was significantly higher than those in the non-NAPV group. Conversely, the non-NAPV population had a significantly higher percentage of patients who developed cutaneous lesions before mucosal lesions than that reported by the NAPV population (see Table 2 ).
Both mucosal and cutaneous lesion sites in patients were widely distributed over all areas of the body. Patients with mucosal disease (in both the mucosal-only and mucocutaneous disease manifestation) reported predominantly oral lesions (97.24%, n = 141), followed by involvement of the nasal passages, and less commonly anogenital or conjunctival lesions. Subjects with cutaneous disease (in both the cutaneous-only and mucocutaneous disease manifestation) reported lesions mainly on the scalp and face (n = 106, 83.46%; n = 61, 48.06%, respectively), less on the torso (chest n = 95, 74.80%; back n = 89, 70.08%; abdomen n = 72, 56.67%), followed by the extremities (arms n = 66, 51.97%; legs n = 53, 41.73%; hands n = 32, 25.20%; feet n = 19, 14.96%).
The difference between the NAPV and non-NAPV populations regarding mucosal lesion distribution was calculated in patients experiencing mucosal-only or mucocutaneous lesions. Cutaneous lesion distribution was calculated in patients experiencing cutaneous-only or mucocutaneous lesions. To address whether patients with distinct morphologic profiles exhibit different lesion distribution patterns, this analysis was repeated for each of the 3 morphologic groups described above: mucosal-only, mucocutaneous, and cutaneous-only. The authors find that regardless of the subgroup analyzed, the general distribution patterns remained the same, and there were only negligible differences between the NAPV and non-NAPV populations (data not shown).
Comorbidity
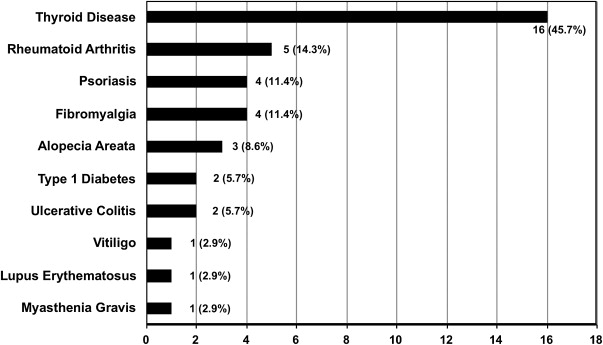
Because several comorbidities have been reported with various autoimmune diseases, it was next assessed whether other autoimmune diseases and cancers were prevalent among patients in the study population. Thirty-five of all 171 PV patients (20.5%) reported an additional autoimmune diagnosis. Nearly half (n = 16) of these were affected by autoimmune thyroid disease ( Fig. 1 ). A history of cancer was reported in 19 of the 171 PV patients (11%). Twelve of these 19 patients reported a history of skin cancer of an unspecified type. A limited number of patients listed cervical- (n = 2), prostate- (n = 2), breast- (n = 1), stomach/colon- (n = 1), or thyroid cancer (n = 1), and thymoma (n = 1). No patients reported a history of lymphoma or leukemia.
Genetics/Family History
Autoimmune diseases tend to run in families, and patients with a particular autoimmune condition often have one or more family members afflicted with autoimmunity. Forty-eight percent of the PV patients in this study (n = 82) reported having a relative with an autoimmune disease, ranging from 1 to 11 affected family members per patient. A total of 172 relatives with autoimmune disease were reported by patients, including 87 (50.6%) first-degree, 59 (34.3%) second-degree, and 26 (15.1%) third-degree relatives.
Five patients in the study had a total of 15 relatives of the first, second, and third degree who had PV themselves ( Fig. 2 ). The remaining patients with a family history of autoimmune disease had relatives affected by a wide range of autoimmune diseases, the 3 most common of which were type 1 diabetes (n = 27), thyroid disease (n = 25), and psoriasis (n = 13).
Subjective Trigger Factors
To shed light on environmental agents potentially relevant for disease induction, patients were asked to document factors they believed may have triggered the onset of their disease. Sixty-two percent of patients (n = 106) reported subjective trigger factors ( Fig. 3 ). Since participants could select more than one trigger, a total of 138 responses were recorded from these 106 patients. Thirty-eight percent (n = 65) of all PV patients reported experiencing a significant emotional trauma/stress before the onset of their disease (including loss of employment, death of a loved one, exposure to violence, neglect, verbal abuse, low self esteem, and depression). Other commonly reported subjective trigger factors were the use of a medication or supplement, a surgical/dental procedure, physical trauma, and illness (mostly infectious in nature). Less commonly mentioned were food/diet, poor sleep, cancer, allergic reaction/rash, vaccination, and climate-associated environmental factors.
When asked whether they had any history of infection before the onset of disease, 64 PV patients reported a total of 76 infections (again, patients could report more than one infection). The most frequently reported infections were of the herpes virus group (n = 35, 46.1% of all reported infections or 20.5% of all participants), including 27 patients with a history of herpes simplex type 1 or 2, 5 with herpes zoster, and 3 with Epstein-Barr virus (EBV) infection ( Fig. 4 ).
Related posts:
 Diagnosis and Clinical Features of Pemphigus Foliaceus
Diagnosis and Clinical Features of Pemphigus Foliaceus
 Pathogenesis of Endemic Pemphigus Foliaceus
Pemphigoid Gestationis: Pathogenesis and Clinical Features
Pathophysiology of Dermatitis Herpetiformis: A Model for Cutaneous Manifestations of Gastrointestinal Inflammation
Pathogenesis of Endemic Pemphigus Foliaceus
Pemphigoid Gestationis: Pathogenesis and Clinical Features
Pathophysiology of Dermatitis Herpetiformis: A Model for Cutaneous Manifestations of Gastrointestinal Inflammation
 Pathogenesis of Epidermolysis Bullosa Acquisita
Nail Involvement in Autoimmune Bullous Disorders
Pathogenesis of Epidermolysis Bullosa Acquisita
Nail Involvement in Autoimmune Bullous Disorders
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


