Pemphigus refers to a group of human autoimmune blistering diseases involving skin and/or mucous membranes. Endemic pemphigus foliaceus (EPF), or fogo selvagem is an organ-specific autoimmune blistering disease, first reported in the beginning of the 20th century in rural areas of Brazil. The disease follows the course of streams and creeks, and vanishes after urbanization of the endemic areas. The auto-antigen related to EPF is desmoglein 1, a 160 kDa glycoprotein of the desmossomal core, targeted by in situ and circulating IgG autoantibodies, mainly of the IgG4 subclass.
Pemphigus refers to a group of human autoimmune blistering diseases involving skin and/or mucous membranes. Circulating and in situ autoantibodies against epithelial transmembrane glycoproteins of the desmosome, mostly desmoglein 1 (Dsg1) and desmoglein 3 (Dsg3), are found in pemphigus patients. Immunoglobulin-G (IgG) autoantibodies against the extracellular domain of Dsg1 and Dsg3 proved to be pathogenic when passively transferred into experimental mouse models. Endemic pemphigus foliaceus (EPF), also known as fogo selvagem (FS) is an organ-specific autoimmune blistering disease, first reported in the beginning of the 20th century (1903) in Brazil. Interestingly, the skin condition was thought to be one of the clinical variants of a superficial mycosis, known as tinea imbricata or tokelau. FS occurs in rural areas of Brazil, following the course of streams and creeks, and vanishes after urbanization of the endemic areas. The disease is observed in other countries of South America, such as Colombia, Venezuela, Peru, Ecuador and Paraguay, and also in Northern Africa (Tunisia).
The skin lesions are characterized by subcorneal blisters that result from the autoimmune aggression, with no mucosal involvement. Although EPF shares clinical, histologic and immunologic features with the classic form, described by Cazenave in1844, its epidemiologic profile is unique, including endemic geographic areas, familial cases, and disease onset at earlier ages, with no differences in gender distribution.
Disease presentation
The primary lesion is a superficial blister that easily ruptures, leaving superficial, denuded areas. Predominant sites occur in seborrheic areas, such as head (scalp and face), neck, and upper trunk. Nikolsky sign is present in most FS patients with active disease. The skin lesions may be worsened by sun exposure and progress in weeks or months. Acute and fulminant FS is seldom reported, with extensive bullae erupting over a period of 1 to 3 weeks. FS most reported clinical presentations are below described.
Localized Form (Forme Fruste)
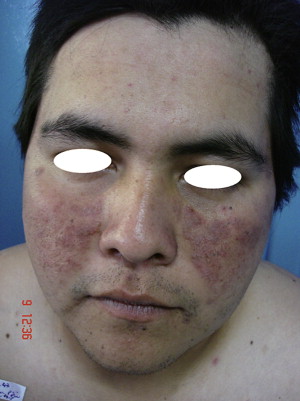
Small vesicles that easily rupture, leaving erosions and crusts are seen on seborrheic areas of the face and trunk. Individual lesions may appear as round or oval keratotic plaques with a yellow–brown surface. Discoid lupus erythematous (DLE)-like lesions, characterized by erythematous-violaceus or hyperpigmented papules and plaques, distributed in the same seborrheic areas, are also described ( Fig. 1 ). However, FS lesions lack the follicular prominence (carpet tack sign), the epidermal atrophic changes, and hypopigmentation, which are usually seen in DLE lesions. Localized FS may remain unchanged for months or years; its course may lead to spontaneous remission, or to acral spreading, involving the trunk and extremities, culminating in generalized disease.
Generalized Forms of FS
Bullous invasion
Patients will present with acute, aggressive disease, in which there is a predominance of widespread, blistering lesions. The lesions are usually confluent on the trunk, and remain isolated in the arms and legs ( Fig. 2 ). Fever, arthralgia, and general malaise are associated with the onset of the vesicular eruption, but bacteremia and sepsis are seldom observed. Occasionally vesicles form circinate or annular patterns, and after rupturing, produce exfoliation resembling the superficial mycosis, tinea imbricata.

Exfoliative erythroderma
Superficial blisters appear on erythematous base, and after their rupture, the skin surface becomes eroded and moist. Keratin maceration leads to a characteristic smell (rat’s nest). Other causes of exfoliative dermatitis must be eliminated before diagnosing FS. Confluent superficial erosions with crusting and serum exudate are the prominent features of the disease ( Fig. 3 ).

Keratotic
Disseminated, keratotic plaques and nodular lesions, similar to the ones present in chronic and localized forms of the disease will be present. These patients may comprise a small cohort of FS who are resistant to therapy.
Hyperpigmented
This form is often seen in patients undergoing remission. It may be restricted to areas of previous lesions, or be disseminated. Before the introduction of systemic treatment with corticosteroids, diffuse hyperpigmentation was considered an early indicator of spontaneous remission or cure. Several patients undergoing clinical remission would experience dramatic changes in their skin color, with marked skin darkening.
Pemphigus herpetiformis
This form is characterized by vesicles or pustules in herpetiform arrangement, and eosinophilic spongiosis. Lesions may either precede or follow typical FS lesions. Immunochemical analysis of pemphigus herpetiformis autoantigens demonstrates reactivity against either Dsg1 or Dsg3.
Before the steroid era, some complications such as growth retardation and dwarfism in children, and azoospermia in adults were described.
Disease pathogenesis
FS is an autoimmune disease with intermingled environmental, immunologic, and genetic influences triggering its onset.
Environmental Factors
FS shows unique and remarkable features such as the geographic and temporal clustering of cases, the increased frequency of cases among young adults and children, the increased frequency of familial cases, and an association with certain distinct HLA-DR alleles. Another striking observation is the decreasing prevalence of FS in some geographic areas that follows urban development. Settlements of native Brazilians, especially the Terena Reservation of Limao Verde, in Mato Grosso do Sul, Brazil, exhibit a high prevalence (3.2%) of FS, and an incidence of 1 to 4 new cases per year.
A possible role of hematophagous black flies ( Simuliid ) has been hypothesized for many years. In a hospital-based epidemiologic case–control study, it was reported that black fly bites were 4.7 times more frequent in individuals developing FS than in control individuals. Interestingly, a predominant black fly species ( Simulium nigrimanum ) in the Terena Reservation of Limao Verde was found, which is rarely seen in nonendemic areas of Brazil. A case–control study performed in the Terena village suggested ( Fig. 4 ) that individuals living in this endemic area might be at risk of developing FS, considering their housing (thatched roofs, adobe walls) and exposure to hematophagous insect bites (kissing bugs or bed bugs).

The same ecological systems found in the ’pemphigus country overlap with those described in Chagas disease and leishmaniasis. Interestingly, many patients with diseases transmitted by hematophagous vectors (ie, onchocerciasis [black flies], leishmaniasis [sandflies], and Chagas disease [kissing bugs]) possess antibodies against the extracellular domain 5 of Dsg1. It is possible that these vectors carry a molecule that triggers the anti-Dsg1 EC5 antibody response (antigen mimicry or cross-reactivity). Recently, the sialotranscriptome of adult female S nigrimanum flies, the most seen black fly in endemic FS areas has been isolated, comprising over 70 distinct genes within over 30 protein families, including several novel families. The sialotranscriptome provides an infinite platform for testing pemphigus patient sera against recombinant salivary proteins from S nigrimanum.
Genetics
Previous studies in FS documented genetic influence in the etiopathogenesis of FS. Classic Brazilian studies from the 19702 (n = 2686 FS patients from Goiania, Brazil) reported that 18% of the patients were blood relatives, and 93% of these familial cases were found in genetically related family members. Further publications revealed that the expression of DRB1-0404, 1402, or 1406 alleles is linked to FS, with a relative risk of 14. The hypervariable region of the DRB1 gene of these alleles at the level of residues 67 to 74 shares the same sequence: LLEQRRAA, which may confer susceptibility to FS.
Autoimmunity
FS autoantigen
Eyre and Stanley demonstrated by immunoprecipitation techniques that sera of patients with either classic PF or FS recognize Dsg1, a 160kDa glycoprotein that belongs to the cadherin family of calcium-dependent cell adhesion molecules (CAMs). Dsg3, a 130kDa cadherin, and the major autoantigen for pemphigus vulgaris (mainly with mucous involvement) is seldom recognized by PF or FS patients (7%). Desmosomal cadherins share extensive homology with other members of this gene superfamily of CAMs, such as desmocollins and E and P cadherins. Dsg1 and Dsg3 are glycoproteins with an ectodomain that contains 6 putative calcium-binding sites, a transmembrane region, and an intracellular domain that is linked to the keratinocyte cytoskeleton via desmosomal plaque proteins.
FS autoimmune response
IgG anti-Dsg1
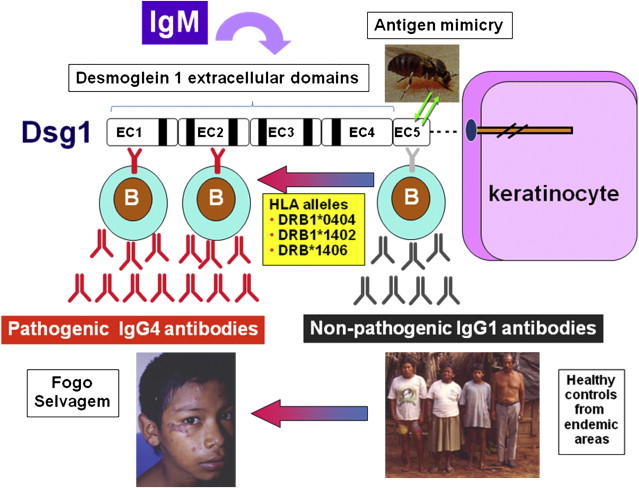
The autoantibody response in FS is based on IgG, and is predominantly of the IgG4 subclass. Total IgG4, F(ab)2, and Fab fragments of FS IgG are all pathogenic in the FS mouse model. Anti-Dsg1 antibodies are detected not only in the sera of FS patients, but also in normal controls that live in endemic areas. Moreover, the percentage of enzyme-linked immunosorbent assay (ELISA)-positive sera among the normal control population is inversely related to the distance from the endemic FS focus. At the molecular level, FS immunopathogenesis presents as an epitope-spreading model ( Fig. 5 ). When using domain-swapped Dsg1 and Dsg3, anti-Dsg1 antibodies from healthy controls and FS, patients on remission show an exclusive response to the extracellular domain (EC-5) of the molecule, whereas FS patients with active disease reveal a major reactivity against the extracellular domains 1 and 2 (EC1-2) of Dsg1. When analyzing preclinical stages of FS, EC-5 remains the major domain involved in the autoimmune response; however, intramolecular spreading may occur at the disease onset, leading to an EC1-2 oriented IgG response. IgG4 is a novel classifier/predictor that identifies donors with immunologic features of FS and is highly sensitive (92% [95% confidence interval, CI: 82–95]) and specific (97% [95% CI: 89–100]). In an FS-prone population, with a prevalence of 3% of the disease, it has a positive predictive value (PPV) of 49% and a negative predictive value (NPV) of 99.7%.
Related posts:
 A Globally Available Internet-Based Patient Survey of Pemphigus Vulgaris: Epidemiology and Disease Characteristics
A Globally Available Internet-Based Patient Survey of Pemphigus Vulgaris: Epidemiology and Disease Characteristics
 Diagnosis and Clinical Features of Pemphigus Foliaceus
Pemphigoid Gestationis: Pathogenesis and Clinical Features
Pathophysiology of Dermatitis Herpetiformis: A Model for Cutaneous Manifestations of Gastrointestinal Inflammation
Diagnosis and Clinical Features of Pemphigus Foliaceus
Pemphigoid Gestationis: Pathogenesis and Clinical Features
Pathophysiology of Dermatitis Herpetiformis: A Model for Cutaneous Manifestations of Gastrointestinal Inflammation
 Pathogenesis of Epidermolysis Bullosa Acquisita
Nail Involvement in Autoimmune Bullous Disorders
Pathogenesis of Epidermolysis Bullosa Acquisita
Nail Involvement in Autoimmune Bullous Disorders
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


