9. Safety Considerations in Aesthetic Surgery
“The physician must … have two special objects in view with regard to disease, namely, to do good or to do no harm.” 1 Hippocrates
Safety in Office-Based Surgery
Two decades ago <20% of surgical procedures were performed on an outpatient basis.
Today >80% of all surgeries are performed in an outpatient setting. 2
Numerous studies have established the efficacy and safety of outpatient office-based surgical facilities.
These studies have shown low complication rates of 0.33%-0.7% and extremely low mortality rates of approximately 0.002%. 2 – 6
The two largest plastic surgery societies in the United States, the American Society of Plastic Surgeons (ASPS) and the American Society for Aesthetic Plastic Surgery (ASAPS), have recognized the importance of establishing a culture of safety and have accordingly established task forces that are charged with establishing guidelines for office-based surgical facilities.
In their review of patient safety in an office-based setting, Horton, Janis, and Rohrich 7 divided this topic into four broad categories:
Administrative
Clinical aspects
Liposuction
Management of postoperative issues, in particular postoperative pain and postoperative nausea and vomiting (PONV)
Administrative Issues
Governance: Policies outlining the structure of office-based surgical facilities include staff responsibilities, supervision, and a patient bill of rights.
Physician qualifications: Practitioners must obtain and maintain adequate training and certification for all procedures/treatments performed in the office facility and should limit their practice to the scope of the certifying board.
Quality assessment: Develop a system of quality of care with continual evaluation focused on improving patient care/safety. This includes the maintenance of the physical plant, operating room/recovery room equipment, personnel evaluations and coursework, and development and implementation of protocols and procedures.
Accreditation and maintenance of surgical facility standards
Protocols for management of emergency situations. This includes transfer protocols to a higher level of care (i.e., hospitals), generally, where the surgeon has admitting privileges and ideally privileges to perform the same procedures that are performed in the office-based setting.
Informed consent process
Maintenance of complete medical records
Guidelines for patient discharge
System for reporting of adverse events
Core Principles
These core principles have been approved by the American College of Surgeons, the American Medical Association, and the ASPS for outpatient office-based surgery involving any level of anesthesia above local anesthesia procedures. 8
Core principle 1: Guidelines or regulations should be developed by states for office-based surgery according to levels of anesthesia defined by the ASA Continuum of Depth of Sedation statement dated October 13, 1999, excluding local anesthesia or minimal sedation.
Core principle 2: Physicians should select patients by criteria, including the ASA Patient Selection Physical Status Classification System. This should be documented in the preoperative evaluation of the patient.
Core principle 3: Physicians who perform office-based surgery should have their facilities accredited by the Joint Commission on Accreditation of Healthcare Organizations, the Accreditation Association for Ambulatory Health Care, the American Association for Accreditation of Ambulatory Surgery Facilities, the American Osteopathic Association, or a state-recognized entity such as the Institute for Medical Quality, or the facility should be state licensed and/or Medicare certified.
Core principle 4: Physicians performing office-based surgery must have admitting privileges at a nearby hospital, or have a transfer agreement with another physician who has admitting privileges at a nearby hospital, or maintain an emergency transfer agreement with a nearby hospital.
Core principle 5: States should follow the guidelines outlined by the Federation of State Medical Boards regarding informed consent.
Core principle 6: States should consider legally privileged adverse incident reporting requirements as recommended by the Federation of State Medical Boards and accompanied by periodic peer review and a program of Continuous Quality Improvement.
Core principle 7: Physicians performing office-based surgery must obtain and maintain board certification by one of the boards recognized by the American Board of Medical Specialties, the American Osteopathic Association, or a board with equivalent standards approved by the state medical board within 5 years of completing an approved residency training program. The procedure must be one that is generally recognized by that certifying board as falling within the scope of training and practice of the physician providing the care.
Core principle 8: Physicians performing office-based surgery may show competency by maintaining core privileges at an accredited or licensed hospital or ambulatory surgical center for the procedures they perform in the office setting. Alternatively, the governing body of the office facility is responsible for a peer review process for privileging physicians based on nationally recognized credentialing standards.
Core principle 9: At least one physician who is credentialed or currently recognized as having successfully completed a course in advanced resuscitative techniques (advanced trauma life support, advanced cardiac life support, or pediatric advanced life support) must be present or immediately available with age- and size-appropriate resuscitative equipment until the patient has met the criteria for discharge from the facility. In addition, other medical personnel with direct patient contact should, at a minimum, be trained in basic life support.
Core principle 10: Physicians administering or supervising moderate sedation/analgesia, deep sedation/analgesia, or general anesthesia should have appropriate education and training.
Clinical Issues Related to Office-Based Surgery
Preoperative evaluation: This includes a thorough history and physical examination performed by the surgeon, with consideration for use of a standardized form to capture all information pertinent to a patient’s medical history, which would allow the surgeon to adequately assess the patient’s risk for surgery and optimize the outcome from the proposed procedure.
Anesthesia evaluation: For any procedure that requires >simple local anesthesia (i.e., sedation or general anesthesia), anesthesia should be given by a practitioner, either a certified nurse anesthetist or anesthesiologist, in accordance with the current specific state requirements where the surgical facility exists.
Patient selection in office-based surgery is an important concept. 9 , 10
Patients should be risk stratified based on the American Society of Anesthesiologists (ASA) physical classification status (Table 9-1).
ASA I and II patients are considered ideal candidates for all types of office-based surgery.
ASA III patients are considered reasonable candidates for procedures that can be performed using a local anesthetic with or without sedation (see Chapter 5).
ASA IV patients are candidates for only local anesthesia procedures in an office setting.
These are general guidelines and should be interpreted by each surgeon in consultation with the anesthesia practitioner.
Monitoring and Minimizing Physiologic Stresses Related to the Surgical Procedure
Hypothermia
Definition: Core body temperature <36° C
Incidence: 50%-90% of surgical patients if no preventative measures are used. 11
Causes:
Thermoregulatory mechanisms are impaired by anesthesia.
Core-to-peripheral heat redistribution begins soon after anesthesia.
Patient loses body heat to ambient temperature of OR. 12
Risks: Increased blood loss, coagulation disorders, increased risk of cardiac events, increased risk of surgical site infection, postoperative shivering, and lengthened hospital stays.
All of these factors secondarily contribute to increased costs. 13
Prevention: Use of cutaneous warming devices, forced-air warming blankets, and intravenous fluid warmers (see Chapter 5)
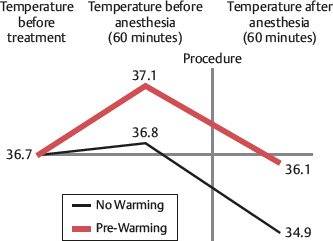
Actively prewarm patients for 1 hour preoperative with forced-air heating
Patients not prewarmed are prone to hypothermia within 30 minutes of anesthesia induction (Fig. 9-1). 12
Recommendations: If no antihypothermia devices are available, office surgical procedures should be limited to <2 hours’ duration and <20% body surface area of exposure. 9
Blood loss
If the anticipated blood loss is >500 ml, the procedure should be performed in a facility in which postoperative monitoring and blood replacement products are readily available. 9
Duration of the Surgical Procedure
Overall procedure length should be limited to <6 hours for office-based surgical procedures. 9
The safety and efficacy of outpatient office-based surgery has been established by numerous studies. 2 – 6
Some studies have correlated the length of the ambulatory surgical procedure with increased rates of postdischarge readmission to a hospital. 14
State regulations must be checked for details, because some states have more aggressive regulations/restrictions.
Postoperative Pain and Nausea
The postoperative management of office-based surgical patients affects the discharge process, the patients’ overall satisfaction with the procedure and facility, and ultimately patient safety.
Inadequate pain control has physiologic effects on all organ systems. 15
Postoperative pain is the main reason for delayed discharge and hospital readmission after ambulatory surgery. 16
Inadequate pain control can also cause PONV.
PONV has received less attention than pain management but actually represents the most common reason for patient dissatisfaction. It is also a major factor in delayed discharge and unplanned postoperative hospital admission.
Up to 10% of patients experience PONV in the recovery room. 15 , 17
The incidence of PONV increases to 30% at 24 hours, and most patients have PONV after discharge with no access to treatment. 17
Long-acting narcotics and inhalational anesthetic agents should be avoided to reduce PONV.
Propofol has been shown to have antiemetic effects. 18
Multimodal pain and PONV management are recommended in the preoperative, intraoperative, and postoperative phases of the office-based surgical procedure.
Multimodal PONV involves treating all five major receptor systems 19 , 20 :
Serotonin (5-HT3): These are currently the most effective and safest agents. 21
Dopamine (DA)
Histamine (H-1)
Acetylcholine (Ach)
Neurokinin (NK-1)
For additional details, see Chapters 7 and 8.
Liposuction
According to the 2016 American Society for Aesthetic Plastic Surgery Cosmetic Surgery National Data Bank statistics, liposuction procedures (414,335) were the most commonly performed aesthetic procedures in the United States. 22 Most of these procedures are performed in an office-based setting.
Anesthesia
(see also chapters 5 through 7)
For small-volume liposuction, infiltration with a solution containing a local anesthetic may be sufficient without the need for adjunctive anesthesia, although the use of monitoring devices during the procedure is recommended.
Bupivacaine (Marcaine) should not be used because of the severity of its side effects, its long half-life, and the inability to reverse toxicity.
Lidocaine maximal dosage is 35 mg/kg. 23
For larger-volume liposuction, the amount of lidocaine used should be reduced.
Superwet (1:1) technique rather than tumescent (3:1) technique is used to reduce lidocaine dosage and infiltrate volume.
If regional or general anesthesia is used, not using or reducing the lidocaine dose should be considered.
Epinephrine: The recommended maximal dose is 0.07 mg/kg, although up to 10 mg/kg have been used safely. 24
Epinephrine is avoided for patients with comorbid medical conditions that prohibit its use, including hyperthyroidism, severe hypertension, cardiac disease, peripheral vascular disease, and pheochromocytoma.
For multiple-site liposuction procedures, infiltration is staged to decrease the epinephrine effects. 24
Patient selection: Liposuction is generally a safe procedure for treating localized adiposity of the abdomen, flanks, arm, trunks, and thighs. Liposuction is not a treatment for obesity. It is generally not recommended for patients with a BMI >30. 25
Volume
In an office-based setting, the maximal volume of lipoaspirate should be 5000 cc. 24 Large-volume liposuction (>5000 cc) should be performed in an acute facility that allows monitoring of fluid resuscitation requirements, and overnight observation/hospitalization should be strongly considered.
Combination Procedures
Studies have shown a cumulative effect on the incidence of complications when multiple surgical procedures are combined in one setting.
Studies have shown that smaller-volume liposuction can be safely and effectively combined with other plastic surgery procedures, even in office settings.
Some states have recently restricted the combination of liposuction with any other type of surgery.
Surgeons operating in an office-based facility must be aware of the local and state regulations.
Mortality
A survey study of ASAPS members showed 95 deaths in close to 500,000 lipoplasty procedures for a mortality rate of 1 in 5224 (19.1/100,000 versus 3/100,000 for elective inguinal hernia repair) 26 (Table 9-2).
Pulmonary embolism (PE) was the most common cause of death (23%).
Overall lipoplasty mortality rates have been reported as 0.0021%-0.019%. 26 , 27
Cause of Death | Number of Deaths | Percentage |
Fat embolism | 11 | 8.5 |
Anesthesia-related complications | 13 | 10.0 |
Hemorrhage | 6 | 4.6 |
Thromboembolism | 30 | 23.1 |
Cardiorespiratory failure | 7 | 5.4 |
Gastrointestinal perforations | 19 | 14.6 |
Massive infection | 7 | 5.4 |
Unknown or confidential | 37 | 28.5 |
Total | 130 | ∼100 |
Combination Surgical Procedures
After the 2000 Florida moratorium banned the combination of abdominoplasty and liposuction, interest in evaluating the safety and efficacy of combined plastic surgical procedures has increased. 28
Many states have imposed arbitrary restrictions on allowable lengths of surgery for office-based surgery.
Florida mandates that procedures lasting >6 hours must not be performed in the office setting, whereas Pennsylvania and Tennessee have imposed arbitrary 4-hour limits on office-based surgery.
Balakrishnan et al 29 reviewed the current available data and concluded: “As they [states] attempt to impose regulations on office surgery, it is evident that sufficient data do not exist to formulate immediate evidence-based policy.”
A review of the literature revealed that most studies have addressed the combination of abdominoplasty with either liposuction or gynecological procedures. 30 , 31
Unlike previous reports, 30 , 31 which were mainly retrospective reviews of the efficacy of combining abdominoplasty with gynecological procedures, these studies established the safety of office-based abdominoplasty and of performing concomitant aesthetic procedures with abdominoplasty. 32 , 33
Stevens et al (2006) 32 : Their study showed no statistically significant difference in complication rates between a group of patients who underwent abdominoplasty with a breast procedure compared with a control group who underwent abdominoplasty alone.
Melendez et al (2008) 33 : Aside from a single episode of PE in their abdominoplasty-only group (incidence 1.03%), they reported no other major complications or mortality in either study group (i.e., abdominoplasty versus abdominoplasty with another aesthetic procedure).
A 2006 retrospective Canadian study 34 compared a group of 37 inpatient abdominoplasty procedures with 32 patients who underwent outpatient abdominoplasty. Most patients underwent concomitant aesthetic procedures. There was no significant difference in complications between the inpatient and outpatient groups.
Although these studies support the safety of combining aesthetic surgical procedures, both abdominoplasty and high-volume liposuction have been established as higher-risk surgeries for VTE, 26 , 27 , 35 and it is prudent for surgeons to approach the combination of these two procedures with caution and maximize patient safety with appropriate VTE prophylaxis. In higher-risk patients these combination procedures should be performed in a hospital, or consideration should be given to not combining the procedures.
Gordon and Koch 36 reviewed 1200 consecutive facial plastic surgeries performed in an office-based setting:
The duration of the procedure was >240 minutes in 1032 (86%) procedures.
Patients whose surgeries lasted <4 hours served as a control group for the lengthier procedures.
The incidence of major morbidity was not increased in the patients undergoing procedures lasting >4 hours.
Clear, evidence-based criteria for the optimal duration of office-based surgery has not been established due to a paucity of objective level 1 evidence. 9 , 28
In general, overall surgical procedure time should be <6 hours for outpatient surgery, especially in the office-based setting. 9
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


