39. Blepharoptosis
Definition
Blepharoptosis is drooping of the upper lid margin to a position that is lower than normal. (Normal upper lid position is at the level of the upper limbus.)
Anatomy
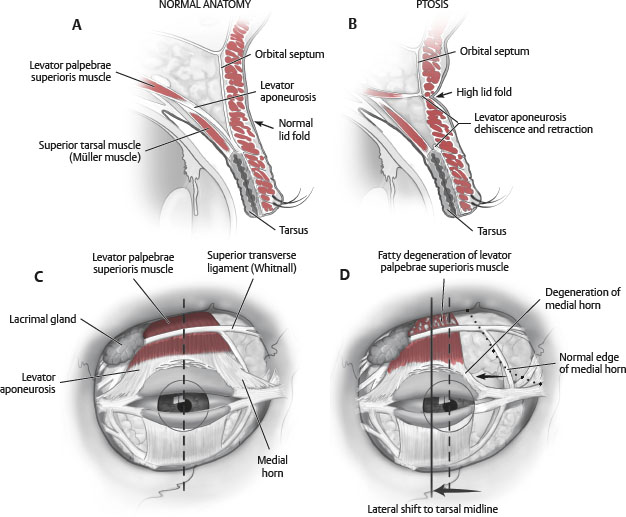
Levator Aponeurosis
Origin: Lesser wing of the sphenoid
Insertion: Orbicularis oculi, dermis, tarsus
Innervation: Superior division of oculomotor nerve (CN III)
Action: Provides 10-12 mm of eyelid elevation
Embryology: Develops in the third gestational month from the superior rectus muscle
Anterior lamella of the levator muscle forms aponeurosis
Posterior lamella of the levator muscle forms Müller muscle
Approximately 2-5 mm above the tarsus the anterior portion of the levator aponeurosis joins the orbital septum.
Müller Muscle
Origin: Posterior lamella of levator muscle
Insertion: Superior border of tarsus
Innervation: Sympathetics
Action: Provides 2-3 mm of eyelid elevation
Frontalis Muscle
Origin: Galeal aponeurosis
Insertion: Suprabrow dermis
Innervation: Frontal branch of facial nerve
Action: Elevates brow and upper eyelid skin
Etiologic Factors/Pathophysiology
True Ptosis
Intrinsic drooping of the affected eyelid
Pseudoptosis: Conditions That Mimic True Ptosis
Grave disease: Retraction of contralateral lid can give appearance of ptosis on unaffected side
Hypotropia: Downward rotation of the globe with accompanying lid movement
Duane syndrome: Extraocular muscular fibrosis and globe retraction
Posttraumatic enophthalmos
Contralateral exophthalmos: Gives impression of ptosis on the unaffected side
Chronic squinting from irritation
Congenital Ptosis
Developmental dysgenesis in the levator muscle
Idiopathic persistent ptosis noticed shortly after birth
Usually not progressive
Signs confined to the affected eyelid(s)
Decreased palpebral aperture with reduction of the pupil reflex to upper eyelid margin measurement (marginal reflex distance test [MRDI])
Decreased levator excursion
Poor or absent levator function reflected in the absence of the supratarsal crease
Ptotic eyelid generally higher than the normal eyelid during downgaze
Inheritance pattern unclear
Levator biopsies in congenital ptosis show absence of striated muscle fibers with fibrosis.
Tip:
History alone usually can distinguish congenital from acquired ptosis, but if there is a question, lagophthalmos on downward gaze is characteristic of congenital ptosis, because levator fibrosis prevents downward lid migration.
Associated ocular abnormalities
Coexistent strabismus and amblyopia
Caused by pupil occlusion
Marcus Gunn jaw-winking syndrome
Synkinesis of upper lid with chewing
Seen in 2%-6% of congenital ptosis
Caused by aberrant innervation from fifth cranial nerve
Blepharophimosis syndrome
Triad of ptosis, telecanthus, and phimosis of lid fissure
Congenital anophthalmos or microphthalmos
Hypoplasia of the lids, globe, and orbital bones
Coexistent eyelid hamartoma
Neurofibromas
Hemangiomas
Lymphangiomas
Acquired Ptosis
Myogenic
Involutional myopathic (senile ptosis)
Most common type
Stretching of the levator aponeurosis attachments to the anterior tarsus
Dermal attachments are maintained and therefore the supratarsal crease rises.
Levator function is usually good.
Chronic progressive external ophthalmoplegia
Progressive muscular dystrophy affects the extraocular muscles and levator.
5% of cases involve the facial and oropharyngeal muscles.
Traumatic
Second most common type
Allow recovery of myoneural dysfunction, resolution of edema, and softening of scar (approximately 6 months).
This can occur after cataract surgery from dehiscence of levator aponeurosis.
Neurogenic
Third nerve palsy: Paralyzes levator muscle
Horner syndrome: Paralyzes Müller muscle
Myasthenia gravis
Primarily, young women and old men are affected.
Ptosis worsens with fatigue, at the end of the day.
Improvement with neostigmine or edrophonium is characteristic.
Mechanical
Upper lid tumors
Severe dermatochalasis (excessive upper lid skin), brow ptosis
Evaluation
Determination of Cause
Congenital or acquired
Tip:
Evaluate for lagophthalmos during downward gaze. This indicates levator fibrosis, which is more commonly seen with congenital cases.
Degree of Ptosis
Always compare with contralateral side.
Measure amount of descent over upper limbus.
1-2 mm: Mild
3 mm: Moderate
4 mm or more: Severe
Record palpebral fissure height.
Levator Function
Measure from extreme downward gaze to extreme upward gaze while immobilizing the brow.
>10 mm: Good
5-10 mm: Fair
<5 mm: Poor
Levator Function | Good | Fair | Poor |
Levator excursion | >10 mm | 5-10 mm | 0-5 mm |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


