48. Lip Augmentation
Definition of Problem
The Aging Lip
Collagen framework loosens, dermis thins, orbicularis oris thins and loses curve, redistribution of volume, cumulative solar damage
Contrary to previous teaching, there is not a loss of volume but a redistribution from thickness to length. 1 , 2
Resultant stigmata
Philtral flattening
Vermilion border flattening
Decreased pout
Cheiloptosis (elongated cutaneous upper lip)
Inverted vermilion (results in thin vermilion)
Minimal dental show
Attenuation and loss of Cupid’s bow curvature
Downward tilt of oral commissures
Perioral wrinkle
Congenital variations
Hypoplastic lip, long cutaneous upper lip, short cutaneous upper lip with excessive incisor or gum show, lack of ideal vermilion contours, asymmetries
Goals of Treatment
Restoration or Creation of Aesthetic Lip Characteristics
Volume: Projection of lips (upper lip in line with or in front of lower), central pout
Shape: Defined philtral columns and Cupid’s bow, projected “ski jump” transition at vermilion border 3
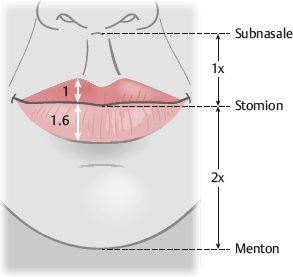
Balance: Upper cutaneous lip/upper vermilion ratio <3 (ideal 1.1-2.3), upper/lower vermilion ratio of 1:1.6 (see Fig. 48-1)
Indications and Contraindications to Treatment
Indications
Enhance lip volume, shape, balance
Improve self-image
Contraindications
Body dysmorphic disorder
Emotional/psychological instability
Unrealistic expectations
Patient demands guarantees
Pregnant or lactating
Immunosuppression
Bleeding disorders
Preoperative Evaluation
Patient History
Assess patient desires and expectations.
Ask patients to provide photos of their lips from when they were happy with them.
Has the patient undergone prior lip augmentation?
Which fillers or methods were used?
Was the patient satisfied with those results?
History of:
Bleeding disorders or immunosuppression
Allergies or history of anaphylaxis
Some products are impregnated with antibiotics.
Hypersensitivities or excessive scarring with previous allogeneics
Counsel patients to stop taking aspirin, NSAIDs, vitamin E, herbal supplements, and other anticoagulants or antiplatelets (if possible) at least 2 weeks before procedure to minimize bleeding and swelling.
Pregnancy or lactation
Smoking
Counsel the patient to stop a minimum of 2 weeks ahead of the procedure; permanent cessation is best.
Labial herpes
Counsel to take acyclovir or valcyclovir perioperatively (3 days before and 3 days after procedure)
Physical Examination
Patient positioning: Upright and in repose
Exclude a current perioral infection.
Measure lip dimensions.
Ideal Lip Dimensions
Frontal view (Fig. 48-1)
The length of the lips should equal the distance from one medial corneal limbus to the other.
Ratio of upper/lower vermilion show should be 1:1.6 (golden ratio) (see Chapter 2).
Upper cutaneous lip/upper vermilion ratio <3 (ideal 1.1-2.3)
Interpupillary line and stomion (commissural line) should be parallel and horizontal.
Aging leads to downward tilt of commissures (frown in repose).
Subnasale-stomion distance should be half of stomion-menton distance.
Lips are sealed when in repose.
Incompetence can be caused by vertical maxillary excess, hypoplastic upper lip, open bite, or muscular dystrophy.
With lips slightly parted, incisor show should be about 2 mm.
When smiling, gum show should be minimal.
Excessive gum show can be caused by vertical maxillary excess, gum overgrowth (necessitating gingivectomy), hypoplastic upper lip, or overactive muscles.
Cupid’s bow forms a “gentle M” shape, the stomion forms a “lazy M,” and the lower lip vermilion forms a “gentle W” with its peaks 2-3 mm lateral to the corresponding M peaks of the upper lip.
Three thickenings of the upper lip: A central tubercle and lateral thickenings, which are separated from the central tubercle by arches
Two paramedian thickenings of the lower lip, which correspond to and contour to the upper arches
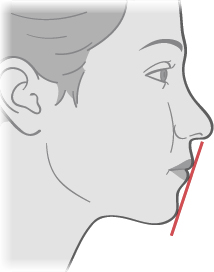
Nasolabial angle should be 85-105 degrees.
Slight eversion at the vermilion border with a projected “ski jump” transition 3
Lips should project beyond line connecting subnasale and pogonion.
Upper lip either in vertical plane with lower lip, or slightly anterior (∼2 mm)
Lower lip anterior to (∼2 mm) soft tissue pogonion
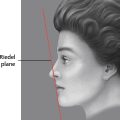
Upper lip, lower lip, and chin should touch an imaginary line (Riedel line).
Chin should be within 1 mm of a vertical line drawn down from lower lip vermilion-cutaneous border (Frankfort plane).
Mid-nares to chin (Steiner line) should touch upper lip.
Labiomental groove ∼4 mm deep
Note asymmetries and contour irregularities.
Evaluate perioral region.
Assess vertical lip lines, nasolabial fold, labiomandibular fold (marionette lines), and prejowl sulcus.
Assess quality of rhytids (dynamic versus static).
Consider adjuvants for perioral rejuvenation (see Chapter 41) such as botulinum toxin, chemical or laser resurfacing, fillers, or implants.
Assess structural/bony loss, dentition, and soft tissue volume loss.
Take preprocedure photos with good lighting (frontal and profile views in repose, frontal and profile views with lips parted) to show the patient postoperative improvement (see Chapter 3).
Patient Counseling and Operative Planning
Outline aesthetic goals.
Discuss various procedures and options (discussed later in the chapter).
There are many approaches to augmenting and enhancing the lips.
Whenever many techniques to solve a problem exist, a universally optimal solution is probably not available.
Each option has advantages and disadvantages in various situations.
Develop an individualized plan with the patient.
Manage expectations, emphasizing realistic aesthetic outcomes.
If a surgical intervention will be performed, inform patient of the risk of hypertrophic or depressed scarring.
Patients are often concerned about pain.
Explain what they can expect during the procedure and the plan to minimize pain.
Explain the postoperative plan.
Augmentation Using Injectable Fillers
7 (see Chapter 22)
Advantages
Minimally invasive
Reversible
Because fillers are temporary, they allow patients to “test-drive” lip augmentation before committing to an intermediate-duration or permanent treatment.
Disadvantages
Good for mild to moderate volume needs, but not high-volume needs
Results are suboptimal in the aged, inelastic, ptotic lip.
Does not correct an elongated upper cutaneous lip.
Can produce “duck bill” or “trout pout” lips in such patients
Should not be used in patients with a history of anaphylaxis, multiple severe allergies, or allergies to bacterial proteins
Examples
Collagen
Bovine (Zyderm and Zyplast, Allergan): 3%-5% have hypersensitivity reaction. Must perform a skin test several weeks in advance
Human (Cosmoderm and Cosmoplast, Allergan): No hypersensitivity reactions
Porcine (Evolence, Ortho-McNeil Pharmaceutical): Longer duration than other collagen (>6 months)
No skin testing is required, but do not use it in patients with a history of anaphylactic or recurrent allergic reactions.
It has been reported to cause nodule formation.
Collagen injectables, in general, have a short duration (3-6 months).
Because of low viscosity, they are good for superficial vertical lip lines and the vermilion border.
Micronized Acellular Dermal Graft (Cymetra, LifeCell)
Short duration (3 months)
Rarely used
Hyaluronic Acid (HA) (Restylane, Galderma; Juvéderm, Allergan)
Most commonly used filler for lip augmentation
Natural constituent of extracelluar matrix; hydrophilic nature draws in fluid volume.
Native human HA lasts only days, so synthesized products are cross-linked for increased stability and longevity.
Rare complications
Longer duration than collagen (6-12 months)
Softer gels (Juvéderm) might be better for the lips, where the skin is thin.
Calcium Hydroxyapatite (Radiesse [formerly Radiance], Merz)
High viscosity and elasticity
Long duration (>12 months)
Used for deep creases and regional volume
Some experts use it along the vermilion border; however, many experts say to avoid its use in lips.
The lips are highly dynamic and can cause fillers to clump on animation.
This leads to lumps and nodules that are hard to treat when long-term or permanent fillers are used.

Senior Author Tip:
Do not inject Radiesse into the lip vermilion. Fig. 48-3 shows an example of the white clumps that often form after injection. These take a long time to disappear and need to be meticulously excised. Clear HA fillers, fat, and dermis are far better alternatives.
Poly-l-lactic Acid (PLLA) (Sculptra, Galderma)
Injected into deep dermis and subcutaneous space
Mechanism of action: Causes inflammatory reaction that leads to collagen deposition replacing filler
Requires multiple treatments to achieve desired augmentation
Long duration
Use in the lips is highly discouraged.
Silicone (Silikon 1000, Alcon)
Permanent
Contraindicated in thin skin
Not intended for use in the lips
Polymethylmethacrylate (PMMA) (Bellafill, Suneva Medical)
PMMA microspheres suspended in 3.5% bovine collagen
Therefore skin testing for sensitivity is needed before use.
Bovine collagen absorbed in 1-3 months, but the PMMA microspheres are surrounded by fibrous tissue and macrophages
Permanent
Can form nodules or granulomas
However, newer preparations have lower complication rates, ∼0.01%.
Successfully used in nasolabial fold, radial lip lines, and white roll
Proper injection technique is vital.
Injected into deep dermis using linear tunneling method with constant pressure through a 26-gauge needle
Not intended for use in the vermilion lip
Many experts warn that it should not be used in this location because of a high risk of lump and nodule formation.
Informed Consent
Needle marking, swelling, redness, ecchymosis, pain, itching
Local reactions to filler or anesthetics
These are usually self-limited.
Asymmetries and contour irregularities
Undercorrection or overcorrection
Complications (as listed later in the chapter)
Equipment
Good overhead lighting
Very small needle, 30- to 32-gauge for low-viscosity products, or slightly larger (∼27-gauge) for high-viscosity products
Anesthetic
Prepare filler.
Powdered fillers should be reconstituted 2-4 hours before injection.
Technique
The technique for HA or collagen injections is described here.
Perform postprocedure massage (pinch and roll) if blending is needed.
Apply Anesthetic
There are several viable approaches.
Cryoanalgesia: Apply ice or a cold compress to the site before injection.
EMLA or other topicals: Must apply 45-60 minutes before injection
Local anesthetic injections: Avoid liberal infiltration, because it distorts tissues.
Buffer the anesthetic with sodium bicarbonate because of the lips’ great sensitivity.
Inject along the vermilion border and areas to be augmented.
Swelling should dissipate after 10 minutes.
Some fillers come premixed with a local anesthetic.
For those that do not, a local anesthetic can be added.
Regional: 0.5 ml of 1% lidocaine can be injected along the upper and 0.5 ml along the lower gingival sulci.
Alternatively, topical benzocaine can be applied along the mucosal sulci using either a cotton-tipped applicator or a 2 × 2 gauze.
Because of the rapid absorption through mucosal surfaces, the anesthetic only needs to be applied a few minutes before injecting filler.
Nerve blocks: Inject ∼0.25 ml at both the infraorbital and the mental foramina.
This can prevent normal motion of the lips, compromising aesthetic outcome.
Some think that this allows too-aggressive injections.
Sterile Technique
Using sterile technique is imperative to prevent infections and biofilm: Remove makeup, prepare the injection site with antiseptic, and do not breach the mucosa.
Injection Technique
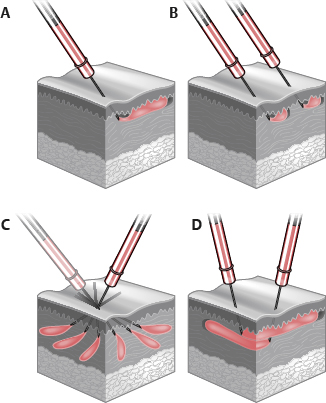
Injection techniques: Anterograde linear threading, retrograde linear threading, radial fanning, serial puncture, and cross-hatching 9 (Fig. 48-4).
Anterograde and retrograde linear threading and serial puncture are the techniques most used for lip augmentation.
Anterograde linear threading: A thread of filler is pushed out ahead of the advancing needle.
Do not inject large boluses into one area.
Retrograde linear threading: The needle is advanced to the desired location, then, as it is withdrawn, a thread of filler is injected.
Serial puncture: The needle is inserted, and a small depot is deposited until resistance is met. The needle is withdrawn and then reinserted a short distance farther, and another small depot is deposited.
Stretch or pinch the lip with nondominant hand to provide a firm, nonmobile surface.
Position needle with bevel facing deep to prevent superficial deposition.
Aspirate before injecting to prevent intravascular deposition.
Inject vermilion lip, vermilion border, and philtral columns as needed for individualized enhancement, seeking to accentuate patient’s anatomy.
A slow (<0.3 ml/minute) and gentle injection technique causes less pain. It also reduces the risk of vascular occlusion and other adverse effects.
Pay careful attention to lip-defining structures.
Be conservative with the philtral columns. Minor alterations are visible.
Preserve the Cupid’s bow. Small alterations are noticeable and can be distorting.
Avoid creating fullness above upper vermilion. This blunts the vermilion border and gives a flat “simian” look.
Accentuate the three upper lip and two lower lip thickenings.
Overfilling effaces lip-defining structures, leading to “sausage” or “duck bill” lips.
Taking a conservative approach, undercorrecting initially with gradual shaping over time, will lead to a more natural look.
Plane of Injection
Vermilion (mucosal): Submucosal, just above orbicularis oris
Vermilion border: Needle in potential space between red and white lip
Low resistance when in correct plane
This provides vermilion definition (ski jump transition).
Philtrum (cutaneous): Mid-dermis 9 (Fig. 48-5)
Young lips: Inject caudal half of philtrum, central three fifths of upper and lower vermilion lips.
Senile lips: Inject full philtrum and across entire vermilion lips.
Some vermilion eversion and shortening of the cutaneous upper lip can be obtained by injecting submucosally in the wet vermilion.
If using collagen, overcorrect by 10%-20%.
Apply ice intermittently for swelling and cryoanalgesia.
Generic Augmentation Approaches
Numerous generic augmentation approaches exist. Two are included here:
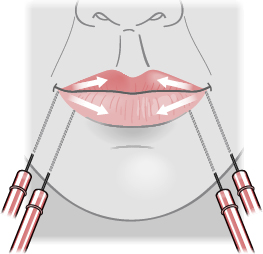
Anterior flow or serial puncture technique 3 , 10 , 11 (Fig. 48-6)
The patient is in an upright, sitting position.
Inject while standing at the patient’s side. Intermittently reassess from frontal view.
Inject from right to center and then from left to center.
Stretch the lip to ensure the needle enters at the commissure (labiomandibular groove).
Insert needle into potential vermilion space at 45-degree angle on mucosal side. Redirect it at 20-degree angle from lip.
Inject filler, pushing ahead of the needle.
When resistance is met and filler will not flow, injection is moved to next point.
Finish half of lower lip. Then inject along the side of mouth, where lower and upper lip connect, thereby elevating the corner of lip and decreasing the labiomandibular groove.
Inject upper lip.
Inject from mandibular margin to lower lateral lip, creating “supportive buttresses” to reestablish vertical height (lost secondary to bone resorption).
Repeat procedure on the other side.
The total injected volume is ∼1 cc into the upper lip and ∼3 cc into the lower lip and buttresses.
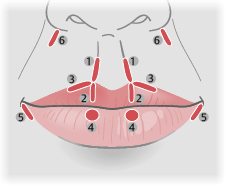
Six-step technique 12 (Fig. 48-7)
12 injections of ∼0.1 cc each
Patient is in a supine position.
Step 1: Define philtral columns. Pinch philtral column with nondominant hand while injecting in retrograde threading fashion in dermis. Repeat procedure in other philtral column.
Step 2: Cupid’s bow. Insert needle at the base of the philtral columns and advance down to the wet-dry margin. Inject in a retrograde threading fashion, creating a strut for each Cupid’s bow apex.
Step 3: Define a portion of the vermilion-cutaneous junction. Inject a thread along the vermilion-cutaneous junction from the apex of Cupid’s bow laterally and halfway to the oral commissure. Repeat procedure on the other side.
Step 4: Lower lip paramedian tubercles. With patient everting lower lip, insert needle into the wet-dry margin at about a third of the way from the midline to the commissure. Deposit 0.1 cc into the orbicularis oris muscle. Repeat procedure on the other side.
Step 5: Support the oral commissures. Inject in the lateral lower cutaneous lip, just below the oral commissure. Repeat procedure on the other side.
Step 6: Nasolabial fold. Inject superiorly in the nasolabial folds. This allegedly helps to evert the lip.
Senior Author Tip:
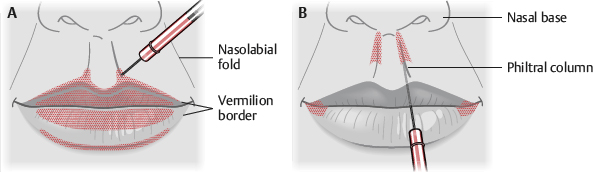
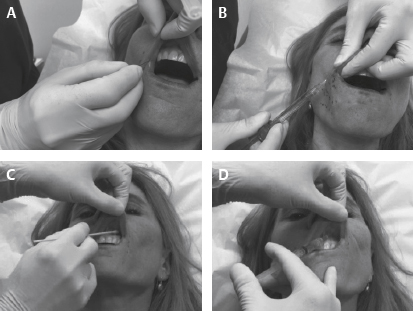
When injecting lips with filler, microcannulas are a surgeon’s best friend. Labial artery anatomy is notoriously variable. 13 The blunt tip of a 25-gauge microcannula introduced from each commissure and extending medially allows bruise-free volumization (Fig. 48-8, A and B). Philtral augmentation needs to be done sharply, however.
Numbing the sensitive vermilion is trivial and should be done with serial submucosal injections of lidocaine 1% with epinephrine at the sulcus. To make these relatively painless injections completely pain free, paint a topical anesthetic onto the mucosa 1-2 minutes before injections (Fig. 48-8, C and D). We use a combination of lidocaine 10%, prilocaine 10%, and tetracaine 4%. This technique prevents the problem of distorting the anatomy by direct injection of anesthetic into the lips.
Postprocedure Care
Schedule next appointment (possibly for touch-ups in 2-4 weeks) to ensure patient retention.
Little to no downtime
Continue intermittent ice application for the next few hours.
Avoid massaging perioral region, and minimize facial movements for the short-term.
Sleep with head elevated for 1 night.
Resume skin care and makeup application after 24 hours.
Take postprocedure photos at follow-up visits.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


