9 Facial Palsy
Abstract
“Facial Palsy” discusses acute-onset palsy of the facial nerve. The ophthalmologist may be the first clinician to see a patient who presents with this condition. Under such circumstances the ophthalmologist should make every effort to establish the underlying cause of the facial palsy and should ensure that the patient’s cornea is adequately protected. Many clinicians incorrectly use the term “Bell’s palsy” synonymously with the term “facial palsy.” A Bell’s palsy is in fact an idiopathic facial palsy and a diagnosis of exclusion. Approximately 10% of patients presenting with an acute facial palsy have a treatable lesion. The ophthalmologist should be aware of the varied disorders that may cause a facial palsy, the detailed evaluation of the patient, and the various medical and surgical treatments available. Effective communication among all clinicians for the optimal care of the patient is essential.
9.1 Introduction
The ophthalmologist may be the first clinician to see a patient who presents with an acute-onset facial nerve palsy. Under such circumstances the ophthalmologist should make every effort to establish the underlying cause of the facial palsy and should ensure that the patient’s cornea is adequately protected. Many patients presenting with a facial palsy are automatically assumed to have a Bell’s palsy, and many clinicians incorrectly use the term “Bell’s palsy” synonymously with the term “facial palsy.” A Bell’s palsy is in fact an idiopathic facial palsy and a diagnosis of exclusion.
Key Point
Approximately 10% of patients presenting with an acute facial palsy have a treatable lesion.
The ophthalmologist should be aware of the following:
A number of other medical, paramedical, and surgical disciplines may be involved in the care of a patient with a facial palsy, including an ENT (ear, nose, and throat) surgeon, a neurosurgeon, a neurologist, a plastic surgeon, a physician, a physiotherapist, and a speech therapist.
The varied disorders which may cause a facial palsy (Box 9.1).
The detailed evaluation of the patient with a facial palsy.
The various medical and surgical treatments available.
A number of other medical, paramedical, and surgical disciplines may be involved in the care of a patient with a facial palsy, including an ENT (ear, nose, and throat) surgeon, a neurosurgeon, a neurologist, a plastic surgeon, a physician, a physiotherapist, and a speech therapist.
Box 9.1 The More Common Causes of Facial Palsy
Bell’s palsy
Ramsay–Hunt syndrome
Otitis media
Mastoiditis
Cholesteatoma
Trauma
Acoustic neuroma surgery
Sarcoidosis
Parotid tumor
Lymphoma
Nasopharyngeal carcinoma
Metastatic carcinoma
Lyme disease
Congenital
Key Point
It is essential that effective communication exist among all clinicians for the optimal care of the patient. The ophthalmologist must be made aware of the prognosis for recovery of facial nerve function, such as after the removal of an acoustic neuroma, and of any plans for surgery by other colleagues, such as facial reanimation surgery.
The ophthalmologist should be involved in the care of any patient in whom a facial palsy may be anticipated postoperatively, such as acoustic neuroma surgery. In the early postoperative period after acoustic neuroma surgery, periorbital swelling can cause a patient with a complete facial palsy to have apparently normal eyelid closure. As the swelling subsides such a patient develops severe lagophthalmos, which may be compounded by a reduced or absent corneal sensation, decreased tear production, and a poor Bell’s phenomenon.
Key Point
The priority for any clinician involved in the management of a patient with a facial palsy is prevention of exposure keratopathy. It is much simpler to prevent corneal ulceration from exposure than it is to treat it once it has occurred.
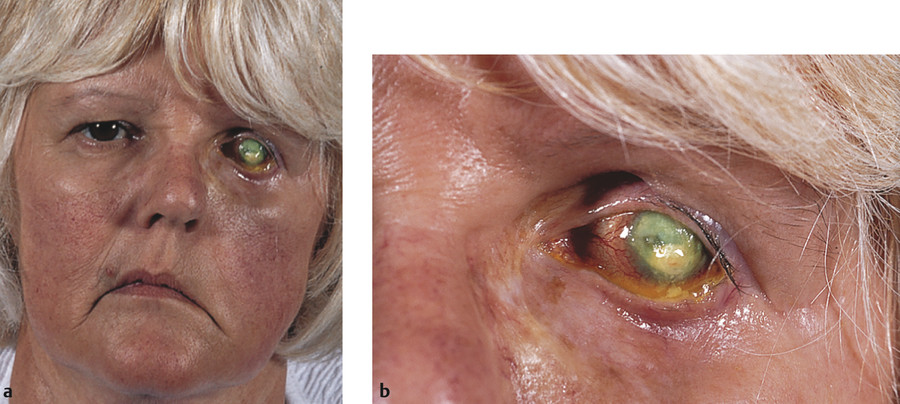
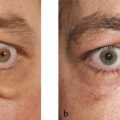
A facial palsy can have a devastating effect on a patient (Fig. 9‑1). It is associated with a number of potential problems that need to be addressed on an individual basis:
Visual defects from corneal exposure or its medical and surgical management.
Ocular pain or discomfort.
Chronic lacrimation and epiphora from corneal exposure, paralytic ectropion, and lacrimal pump failure.
Cosmetic disfigurement.
Difficulties with speech or drooling.
These problems can affect a patient’s ability to work, drive, and to interact socially. Patients may lose self-esteem and become discouraged and depressed.
9.2 History
A full history should be taken and a comprehensive examination performed to determine the cause of the facial palsy. Specific questions should be asked about the following:
Onset and duration of the palsy.
Any prior trauma.
Any past ENT history.
Any symptoms of hearing loss or hyperacusis.
Any symptoms of ear pain or discharge.
Any symptoms of other cranial nerve dysfunction, such as diplopia, anosmia, difficulty swallowing, or neurosensory facial deficits.
Past medical history, including, diabetes, sarcoidosis, and myasthenia.
Any skin rashes.
The patient’s presenting ocular complaints should be noted. The patient should be carefully observed during the history taking. An incomplete blink or any facial asymmetry or loss of the nasolabial fold or forehead creases should be noted.
9.3 Examination
The patient should undergo a complete ophthalmic examination. The patient should be examined systematically:
The muscles of facial expression should be tested to determine whether the patient has a facial nerve paresis or a complete paralysis. In a chronic palsy, signs of aberrant reinnervation should also be sought.
The degree of facial motor nerve palsy can be graded using a scoring system such as the House–Brackmann scoring system (Table 9‑1) to assist in monitoring the return of facial nerve function. In general, the temporal branches of the facial nerve are the most severely affected and the last to return.
The frontalis muscle should be tested to differentiate an upper motor neuron lesion (intact frontalis action) from a lower motor neuron lesion (impaired frontalis action).
The extent of voluntary passive and forced eyelid closure should be determined and the degree of lagophthalmos measured (Fig. 9‑2c,d).
Any upper eyelid retraction is noted (Fig. 9‑2a). (The upper eyelid retracts in chronic facial palsy because of the unopposed action of the levator muscle. In some patients upper lid retraction is masked by the effects of a brow ptosis. Some patients also develop a gradual contracture of the anterior lamella of the upper eyelid, which further aggravates lagophthalmos.)
The corneal sensation must be tested before the instillation of any topical anesthetic agents; the cutaneous sensation in the distribution of the branches of the trigeminal nerve should also be tested.
The cornea is examined using a slit lamp, and fluorescein is instilled into the conjunctival sac (Fig. 9‑2b). Any exposure keratopathy is recorded.
The tear film is assessed and the tear film break-up time measured. The height of the tear meniscus is recorded and a Schirmer’s test performed to assess tear production.
The fluorescein dye disappearance can also be observed and compared with the fellow eye. The patient’s blink should also be observed using the slit lamp, noting whether this is complete or incomplete.
The presence or absence of a Bell’s phenomenon is determined (Fig. 9‑2c,d).
The lower eyelid should be examined for any retraction or frank ectropion (Fig. 9‑2e).
The position and patency of the inferior punctum is determined.
The ocular motility should be carefully tested. This is important because the abducens nerve lies in close anatomical proximity intracranially to the facial nerve nucleus and nerve fascicles.
The patient’s hearing should be tested and the ear examined for any skin lesions affecting the external auditory meatus (e.g., herpes zoster or Ramsay–Hunt syndrome) (Fig. 9‑2f).
The parotid glands should be palpated for masses.
The preauricular, submandibular, and cervical lymph nodes should be palpated.
The oropharynx should be examined.
Although the patient’s visual acuity should be recorded, this may be inaccurate because of the presence of ophthalmic ointments, which may have been instilled into the eye for corneal protection.

9.4 General Treatment Considerations
Patients who are at high risk of exposure keratopathy and corneal ulceration should be identified early. The following are significant risk factors:
Absence of corneal sensation.
Severe lagophthalmos.
An absent Bell’s phenomenon.
A dry eye.
Patients may have more than one risk factor that further compounds the problem.
Key Point
Loss of corneal sensation indicates a severely guarded prognosis for patients with facial palsy and demands urgent and aggressive treatment.
Other factors must also be considered in determining the most appropriate medical or surgical treatment of an individual patient. These include the patient’s age, general health, and ability to comply with medical therapy regimens and frequent follow-up visits.
9.5 Medical Treatment
A number of relatively simple medical therapies can be applied, particularly for a limited time in a patient who has a good prognosis for the recovery of facial nerve function and who has no risk factors for the development of exposure keratopathy. These include the following:
Frequent use of preservative-free topical lubricants.
The avoidance of ocular irritants.
The use of spectacle side shields or moisture chamber goggles.
Taping the eye closed at night.
Upper eyelid botulinum toxin injections.
The application of external eyelid weights.
The most common ophthalmic treatment for facial palsy is the frequent use of lubricants. The lubricants should be used at least on an hourly basis during the day and should be preservative-free to avoid corneal toxicity from such frequent exposure to preservatives. Preservative-free lubricant ointment (e.g., Lacri-Lube or Xailin Night ointment), provides more efficient corneal protection than drops with a much reduced frequency of instillation but with more blurring of vision. Patients should avoid ocular irritants wherever possible (e.g., tobacco smoke).
Most patients do not tolerate moisture chamber goggles or plastic wrap occlusive dressings, but spectacle side shields are relatively unobtrusive and well tolerated.
The upper eyelid can be taped closed over the eye at night using Micropore, but it is essential to ensure that the eye is fully closed to prevent further trauma to the cornea by the tape, particularly in a patient with reduced or absent corneal sensation.
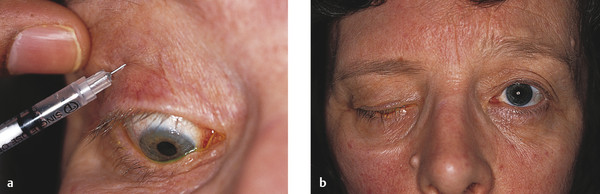
Botulinum toxin can be injected into the levator muscle to induce a ptosis for a patient with a temporary facial palsy (Fig. 9‑3). This is, however, expensive and commits the patient to monovision for a period of 8 to 12 weeks before spontaneous recovery occurs. Some patients can develop problems with fusion and suffer diplopia after the use of botulinum toxin. In addition, because the superior rectus can be weakened, the Bell’s phenomenon may be adversely affected, creating more problems with exposure keratopathy during the recovery phase.
An external eyelid weight may be applied to the upper eyelid with a tissue adhesive (Fig. 9‑4).
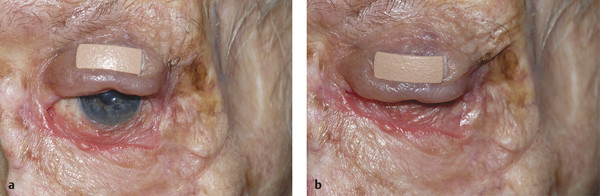
The weight is flesh colored to make it less conspicuous. Such weights are useful for a temporary facial palsy but can also be used for a trial period before subjecting a patient to an upper eyelid gold weight implant or platinum chain implant.
Patients with the onset of a true Bell’s palsy should be treated within 72 hours of the onset of the palsy with a high dose of oral corticosteroids to improve the rate of recovery. Studies have shown that antiviral agents are ineffective in the treatment of Bell’s palsy.
Patients can gain additional regularly updated information about their condition and various management options by visiting www.facialpalsy.org.uk.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


