8 Alar Base Modification
Pearls
Modifications to the dorsum and nasal tip will affect the alar base width, as well as the deliberate creation of illusions, as a result of objective changes.
Alar base surgery should be performed as the final procedure in the rhinoplasty sequence.
Appropriate design, symmetry, and meticulous soft tissue handling are paramount in creating the desired outcome in alar base surgery.
The modified Weir excision is the most commonly employed design for East Asians, who typically need reduction of alar flaring, nostril size, and alar base width.
The use of a cinching suture to maintain a tensionfree skin closure is an important part of alar base surgery.
It is paramount that a curved portion of the nostril be preserved to avoid creating a teardrop nostril during the excision design.
Conservatism should be observed during resections, as correction of over-excision is very difficult.
Complications of alar base surgery include the creation of a teardrop nostril, asymmetry of the nostrils, and various scar-related complications, including vestibular stenosis with accompanying nasal obstruction.
Most complications are iatrogenic and can be avoided with good design and tissue handling.
The benefits of alar base surgery must be weighed against the potential for complications; this is especially true for East Asian peoples, whose skin is more prone to scar-related complications.
Introduction
The alar base describes the portion of the nose where the alar side wall attaches to the midface. Modification to this area changes the alar base width, the degree of alar flaring, and nostril shape and size. Ethnic variations in the alar base have been well described. The majority of East Asian noses (especially those of Southeast Asian origin) cannot conform to the ideal anatomic relationship described in Caucasians. The alar base of the East Asian nose is wider compared with the European nose, with a marked tendency to flare but not to as severe a degree as those found in Africans or Southeast Asians, including those of Filipino, Malaysian, Indonesian, and Vietnamese ethnicity.1
The shape and extent of alar flaring will depend on the shape and elasticity of the underlying nasal cartilage, the connection between the lateral crura and the face, and the prominence of the nasal tip. In addition to the flaring and wide alar base, other abnormalities such as alar rim hanging,2 retrusion of columella, wide columellar base, and excessively thick alar rim should also be considered. Techniques to change the alar shape are chosen after assessing all these parameters individually and judging comprehensively, considering harmony of the ala with the rest of the face.
Given these ethnic variations, it should not be surprising that alar base surgery is one of the most commonly requested procedures during consultation for East Asian rhinoplasty.
The potential indications for alar base surgery are (1) increased alar base width, (2) excessive flaring of the alar side walls, (3) large nostrils, (4) thick alar side walls, (5) hooded or hanging alar side walls, and (6) cleft nose or nostril asymmetry.
Patient Evaluation
A careful and detailed history should be taken during consultation to identify the patient’s concerns. Examination of the alar base should focus on the nostril shape, size, and symmetry; the degree of alar flaring; and the width of the nasal base. Any preexisting asymmetry of the nostrils should be noted and pointed out to the patient, and corrected whenever possible during surgery; this is also important to avoid any concerns that may have arisen iatrogenically after surgery.
Physical Examination
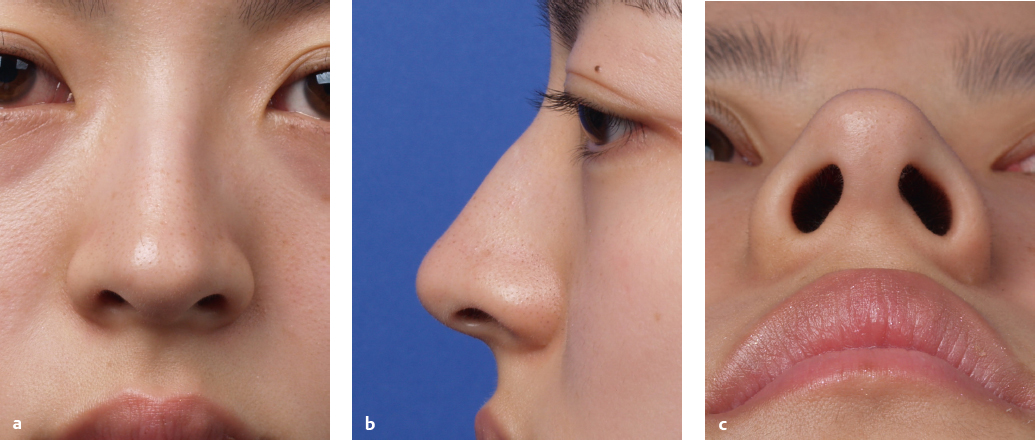
On frontal view, the alar rim should arc and end higher than the columella, giving a gull’s-wing-in-flight appearance. Exaggeration of the gull-in-flight curve implies retraction of the ala or dependency of the infratip lobule. On lateral view, the alar rim usually situates 2 to 3 mm above the nasal columella, creating a columellar show. The lateral view is also the best view for evaluating the alar-columellar relationship. When the columella is not seen, this may indicate a retracted columella or hanging ala. Normally, the width of the alar base is equal to the distance between the medial canthi. The thickness and flaring of the ala and the degree of recurvature of the alar base insertions should also be noted. Ideally, the nose as seen from basal view should be an isosceles triangle with a round apex, slightly bulging alar side walls, and nostrils tilted 30 to 45 degrees from the midline, with the appearance of a pear. The ratio of the columella and infratip lobule is 2:1, and the beginning of the flare of the medial crural footplates divides the alar base into halves (Fig. 8.1).
The Effect of Illusions on the Nasal Base
Although alar base surgery is frequently requested as an isolated procedure, the patient must be informed that the appearance of the alar base is affected by modification of the nasal tip and dorsum, and that surgery to this area cannot be considered in isolation. Increased nasal tip projection and dorsal augmentation will both create an illusion of decreased alar base width. Conversely, narrowing the alar base will create the illusion of a broader nasal tip. If surgeries in these areas are also required, the patient should be advised accordingly.
In certain cases, modification of the dorsum and tip alone may suffice to create the illusion of decreased alar base width and flaring, making alar base surgery unnecessary.
It is imperative that the patient be informed that modifications to these other areas influence the characteristics of the alar base, and may make alar base surgery unnecessary. In case of doubt, alar base excisions should also be performed as a staged procedure, after the patient has a chance to evaluate the effect that these other modifications may have on the alar base.
Quality of Skin
Alar base surgery is essentially a skin excision of the alar base region. The quality of the patient’s skin is an important determinant of the surgery’s outcome. The skin of the alar base region is naturally thick and sebaceous. In addition, East Asian skin is thicker and more pigmented than Caucasian skin. These factors predispose the East Asian patient to hypertrophic scarring, keloid formation, and post-inflammatory hyperpigmentation when undergoing alar base surgery.3
A patient with thick sebaceous skin who gives a history of scar-related complications should be warned of the possibility of these complications when planning alar base surgery. And meticulous postoperative care should be practiced to minimize such complications.
Function
Any static and dynamic collapse of the external nasal valve must be noted. Alar base surgery that reduces the size of the vestibular aperture can cause external valve stenosis. The patient should be asked to inspire through the nose rapidly, and any collapse of the alar side wall should be noted. Patients with small nostrils should have excision designs that do not further reduce the nostril aperture; patients with dynamic collapse should consider functional surgery to strengthen the lower lateral cartilages concomitantly, such as the use of batten grafts, together with alar base surgery if required.
Photographs
Proper photo documentation using a prime portrait lens and diffuse lighting is a clinical and medico-legal requirement for rhinoplasty. A frontal view, profile view, and basal view are used in evaluating for alar base surgery. Computer simulation can be particularly useful to illustrate the complex relationships between dorsal length, tip projection, tip bulbosity, and alar base width, with the patient’s decisions carefully documented.
From the frontal view photograph, the width of the nasal base can be evaluated; this should ideally lie just outside of the middle horizontal fifth of the face in Orientals. The base can appear wide from excessive flaring or from a large inter-alar distance. Excision targeting the right areas must be designed to address these problems.
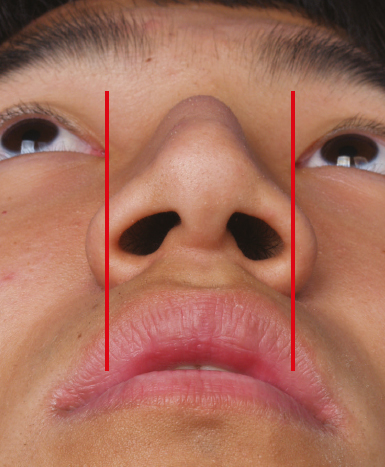
From the basal view the size of the nostrils and degree of flaring can be objectively assessed. Vertical lines passing through the alar facial groove can be drawn in the basal view. Excess alar side wall lateral to this line gives an objective measurement of the degree of alar flaring and aids in planning the excision design (Fig. 8.2).
From the lateral view, a line drawn through the long axis of the nostril allows the surgeon to evaluate the extent of hanging alar deformity and the amount of “lift” required to correct alar hooding.2
Surgical Techniques
Surgical Anatomy
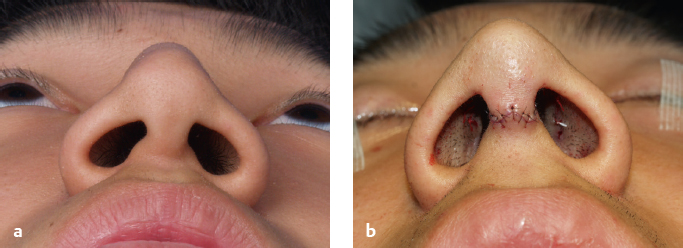
Alar base surgery is performed as the final procedure in the rhinoplasty sequence. This allows the surgeon to fully evaluate the effects from any modifications to the dorsum and tip on the alar base (Fig. 8.3). If an open rhinoplasty approach has been performed, the columella incision is closed with a few monofilament sutures to restore tension to the skin pocket. The need for alar base surgery is then assessed from the basal view, frontal view, and profile view as outlined earlier in the chapter.
The alar base region consists of thick sebaceous skin externally, hair-bearing vestibular skin internally, and fibro-fatty tissue in between. There are no cartilaginous structures found here. The junction of the alar side wall and lateral nasal sill form a natural curvature at the inferior lateral aspect of the nostril, which must be preserved during any alar base surgery to avoid creating a teardrop nostril.
The junction between the alar side wall and midface forms the alar facial groove, and whenever possible, this should be preserved. Leaving behind a 1-mm cuff of soft tissue above the alar facial groove when planning the inferior incision greatly facilitates closure and faster wound healing.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


