63 Managing Complications after Breast Radiation Therapy
Summary
Radiation therapy has a well-defined role in breast cancer treatment, as neoadjuvant or adjuvant after mastectomy or conservative breast treatment. It has been used for about 80 years in the treatment of breast cancer with good results. After the article published by Veronesi, the radiotherapy started to be used more widely in conservative breast cancer treatment with very good results, which favored the advent of oncoplastic surgery. Historically, radiation therapy was associated with severe burns and tissue degeneration, and severe sequelae of the thoracic wall, axillary region, and upper limb. Because of technological development, the complications linked to breast radiotherapy have decreased in number. The complications encountered today in the acute period are edema, erythema, pain, and blisters with epithelial desquamation. Late complications are fat necrosis, radiation-induced calcifications, breast deformity and fibrosis, severe skin retraction, chronic skin ulcers, osteoradionecrosis, chronic infections, and irradiation-induced cancers. For the acute complications, the treatment is usually local, with creams and paraffin gauze dressings. For the local chronic complications, reconstructive surgery is usually required. In superficial ulcers and breast deformities, fat transfer can be used, and for deeper wounds and for osteoradionecrosis and chronic infections, wound debridement and flap reconstruction are indicated. In cases of irradiation-induced sarcomas, surgery and associated therapies are used. The goal of this chapter is to present radiation therapy complications and their treatment.
Key Teaching Points
Radiation therapy is an important adjuvant in the treatment of breast cancer either after mastectomy or in the case of conservative breast surgery.
Even though technology and protocols are evolving, there are still many side effects of radiation therapy that need to be addressed in the acute or chronic period.
The acute complications are usually self-limited and most often local, but they can interfere with treatment, causing treatment delays, which are associated with a poorer prognosis.
Chronic complications can be general or local, and they are more frequent with higher radiation doses received by the patient and they also vary with patients’ radiosensitivity.
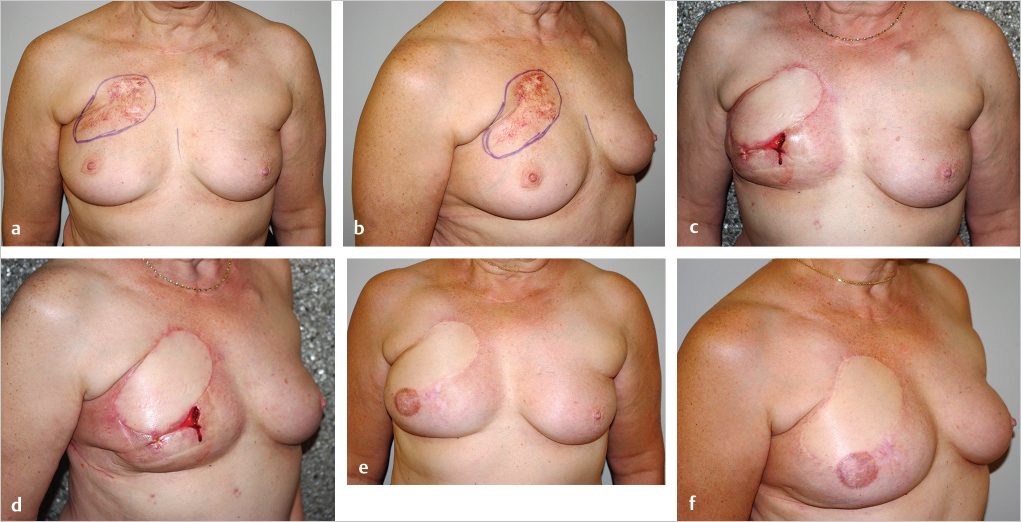
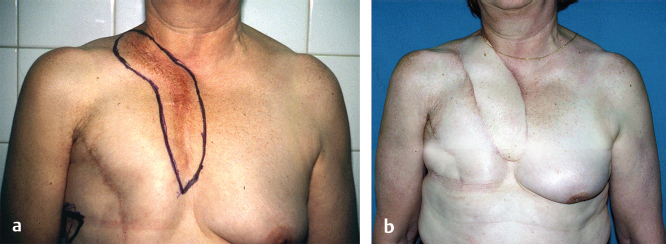
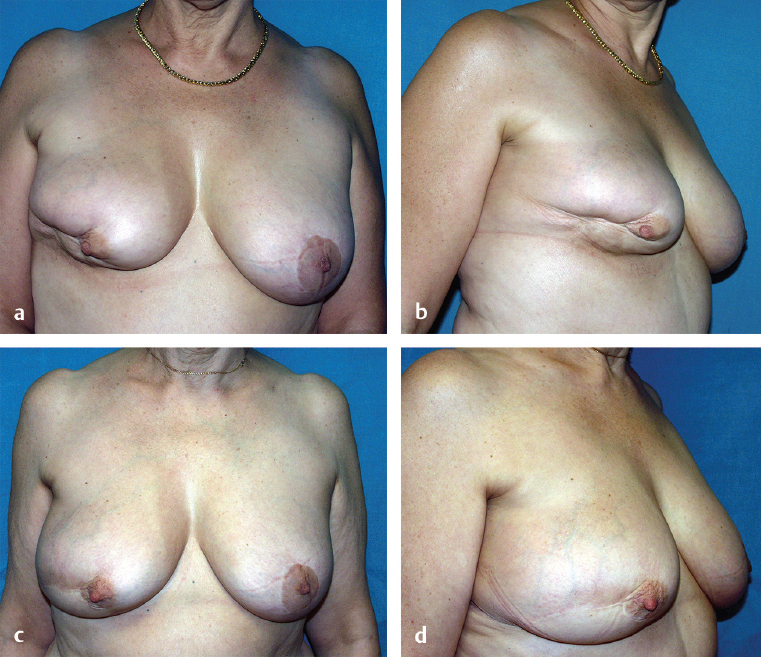
Local chronic complications have a great impact on the patients’quality of life and can be treated with different surgical interventions such as lipomodeling or flaps if they are physically impairing.
Radionecrosis, osteoradionecrosis, and radiation-induced sarcomas are severe complications of radiation therapy and their treatment is resection and flap reconstruction.
63.1 Introduction
Radiation therapy has been an adjuvant for breast cancer treatment for about 80 years and its use is continuously researched and developed to increase the beneficial effects and to reduce the undesired ones.
One of the first descriptions of the role of radiation therapy as an adjuvant to surgery or as a treatment for the inoperable breast cancer cases was that of Keynes in 1934. In 1959, Paterson tried to identify the role of radiotherapy as an adjuvant treatment after mastectomy. Palmer and Ribeiro published a 34-year follow-up study that started in 1949, and supported the role of radiotherapy in preventing or delaying local recurrences but with no impact on the survival rates. Later on, Veronesi and colleagues published a study that showed that women with small breast cancer can be treated with conservative breast surgery and, if associated with radiation therapy, the survival rates resemble those after radical mastectomy alone. Furthermore, this article opened the way for a new surgical approach in breast cancer surgery—the oncoplastic techniques (lumpectomy or quadrantectomy associated with breast reduction, mastopexy, or breast flaps remodeling and radiotherapy).
More recent articles published by Overgaard and Ragaz showed the role of radiation therapy in decreasing local recurrences and metastasis, and increasing survival rate in women with premenopausal high-risk breast cancer.
In the light of all these developments, adjuvant radiotherapy gained a more important role in breast cancer treatment.
Even if it proved its efficacy, radiation therapy has its inconveniences, well underlined by Robinson in his article of 1955: slow healing, infections, radionecrosis, osteonecrosis, chronic pain. Since then, the radiotherapy devices and protocols evolved, and the complications became less frequent and less severe, but they still occur.
The purpose of this chapter is to present the effects of radiation therapy on the tissues, the indications in breast cancer, and the complications that may develop in different moments after radiation therapy and the available therapeutic arsenal.
63.2 Radiation Therapy and Its Effects
There are two types of radiation therapy that are used today: external beam radiotherapy and brachytherapy or internal radiotherapy.
63.2.1 External Beam Radiation Therapy
For the external beam radiation therapy, the X-rays are generated by a machine outside the patient’s body that is calibrated before treatment. In the classical approach, the radiation targets the breast area affected by the cancer and it takes 5 to 7 weeks. The classical approach is 25 sessions of radiation therapy summing up 50 Gy of radiation.
In order to decrease the treatment duration and local complications, new techniques have been developed, reunited under the name accelerated breast irradiation.
Hypofractionated Radiation Therapy
With this method, the radiation is given in larger doses and the duration of the treatment is limited to 15 or 16 daily treatments delivered over 3 weeks. The advantage is that this technique is less time consuming and improves the patient’s quality of life. The larger dose for treatment session might induce greater fibrosis and cosmetic deterioration in breast cancer conservative surgery.
Intraoperative Radiation Therapy
With intraoperative radiation therapy, a single large dose of radiation is given intraoperatively after tumor resection. It requires a special device. The advantages are that the patient completes the treatment during surgery and that the method has lower tissue toxicity than the standard therapy.
63.2.2 Brachytherapy
Brachytherapy is also known as local radiation therapy or curietherapy. It is performed by introducing tubes or catheters into the breast tissue surrounding the lumpectomy site that are filled with radioactive pellets (interstitial brachytherapy), or by introducing into the lumpectomy site a balloon that is going to be filled with radioactive product and removed after the end of treatment (intracavitary brachytherapy).
Brachytherapy is an alternative to external radiation therapy in conservative breast treatment for early-stage breast cancer and also as a solution for reirradiation in case of local recurrences after mastectomy.
63.2.3 Indications for Radiation Therapy in Breast Cancer
For conservative breast cancer treatment, radiation therapy is indicated in
Lumpectomy resection with positive margins (association of a boost dose of radiation), if the patient refuses further breast tissue resection or mastectomy.
Lumpectomy resection with negative margins.
For patients with mastectomy, radiation therapy is indicated in:
Patients with T1–T2 tumors with one to three positive lymph nodes and axillary lymph node dissection (to be discussed in the context of the tumor type and patient’s risk factors).
Patients with advanced local T3–T4 tumors independent of nodal status.
Patients with four or more involved lymph nodes.
Patients with involved resection margins.
63.2.4 Effects of Radiation Therapy on Tissues
The purpose of radiation therapy is to destroy cancer cells while doing minimal damage to the normal tissue. Radiation therapy acts by high-energy radiations to the cancer cells. It is believed that the ionizing radiation produced modifications to the DNA of the rapidly proliferating cells. Ionizing radiation produces DNA break and reactive oxygen species that increase the damage to the malignant cells’ DNA. These modifications induce cell death.
Radiation affects the normal tissues also and the injuries are dynamic and progressive and manifest as the side effects linked to radiation therapy.
Studies have shown that some patients are more sensitive to ionizing radiation, and this increased sensitivity appears partly due to genetic variations. The radiosensitivity manifests as tissue toxicity and this is why patients react differently to the same dose of radiation.
The effects of radiation therapy are classified as acute (they appear during the treatment or a few weeks later) and chronic (they appear months or years later).
Radiation Therapy Complications
After radiation therapy, the most common complications are skin related, but there can also appear general complications such as pulmonary, cardiovascular, lymphedema, chronic pain, brachial plexopathy, and shoulder mobility problems. During the acute phase of the radiation treatment, patients can describe fatigue, and in the long run, the chronic complications can have a major impact on the quality of life of breast cancer survivors.
The Radiation Therapy Oncology Group (RTOG) scale classifies the effects of radiation therapy on skin and subcutaneous tissue in five grades:
Grade 0: no skin reaction.
Grade 1: slight hypo- or hyperpigmentation, mild pruritus, faint erythema, light desquamation, no pain, increased density on palpation.
Grade 2: atrophy of the skin and the subcutaneous tissue, complete hair loss, marked hypo- or hyperpigmentation, painful moderate erythema, skin and subcutaneous tissue induration with minimal or without retraction, intense pruritus, moist desquamation, moderate edema, moderate telangiectasia, superficial ulcerations less than 2 cm.
Grade 3: moderate to major burns, fibrosis is very marked with retraction and fixation to the thoracic wall, painful intense erythema, intense pruritus that interfere with daily activities, moist desquamation, ulcerative dermatitis, many confluent telangiectasia, ulcerations 2 cm or larger.
Grade 4: general exfoliative ulcerative or bullous dermatitis, full-thickness skin necrosis with spontaneous bleeding.
63.3 Management of Acute Complications after Radiation Therapy
Mild acute complications after or during radiation therapy are very common and they do not require stopping the therapy or performing complicated care. About 20% of the patients develop severe acute skin reactions due to radiation therapy that can interrupt and delay treatment. Interruption of radiotherapy more than 1 week has a negative impact on locoregional control of the disease and on overall patients’ survival.
The severe acute skin reactions after radiotherapy appear to be linked to the dose of radiations, a high body mass index, older age, and smoking.
The most common acute complications are
Erythema and edema with burning pain sensation (▶Fig. 63.1).
Dry desquamation.
Moist desquamation with vesicles.
One of the most common recommendations of preventing and minimizing skin lesions is to moisturize the irradiated area and clean it with water or water and mild soap. Also, there can be associated creams with corticosteroids, aloe vera gels, and vegetable oils with high concentrations of essential fatty acids.
Moist desquamation can be treated with hydrocolloid dressings that favor epithelization and diminish the bacterial contamination. If no infection occurs, the lesions heal within 3 to 6 weeks.
In cases of acute ulceration and acute skin necrosis, the radiotherapy is interrupted and a more complex treatment is needed. Serial surgical debridement and defect covering with skin grafts or with a flap is required.
In most cases, the radiodermatitis regresses within 10 to 15 days, but the irradiated areas remain hyperemic for 6 to 9 months. After this period, the skin recovers or remains hyperpigmented. Once the edema disappears in cases of conservative breast treatment, the breast can change the shape and become retracted and smaller.
63.4 Management of Chronic Complications after Radiation Therapy
Chronic complications are usually dose related, and when higher than 60 Gy, the complication incidence is much higher. Other causes can be miscalculation of the required dose, patient’s radiosensitivity, accidental overexposure, and field crossing when the patient has bilateral breast cancer.
Chronic complications after radiation therapy can be
General:
Actinic pneumonitis.
Lymphedema, shoulder immobility, and brachial plexopathy.
Cardiac complications.
Local:
Hyperpigmentation (▶Fig. 63.2).
Hypopigmentation.
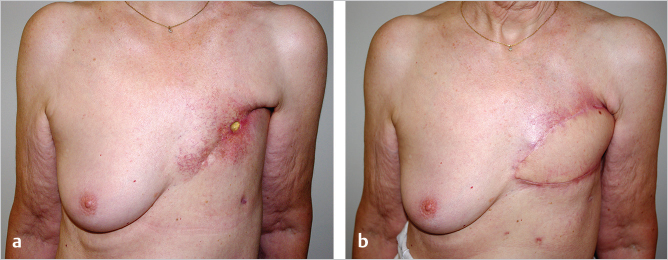
Telangiectasia (▶Fig. 63.3).
Hypoesthesia.
Skin dryness.
Chronic pain.
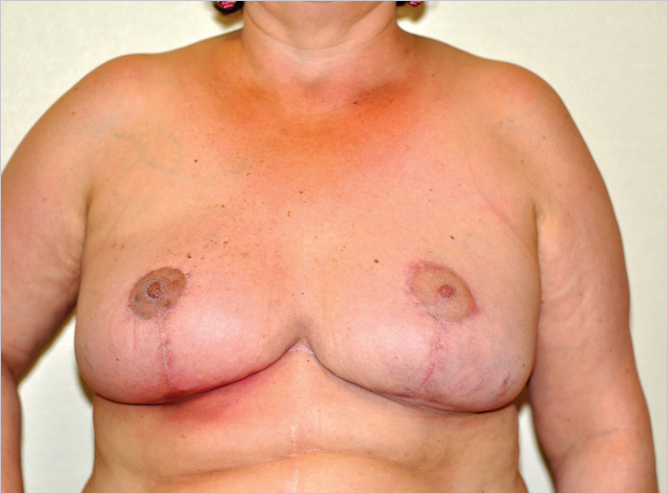
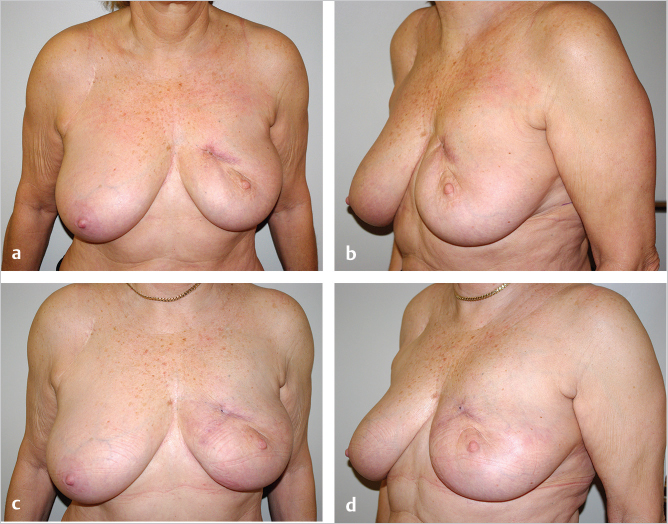
Fibrosis (▶Fig. 63.4; ▶Fig. 63.5).
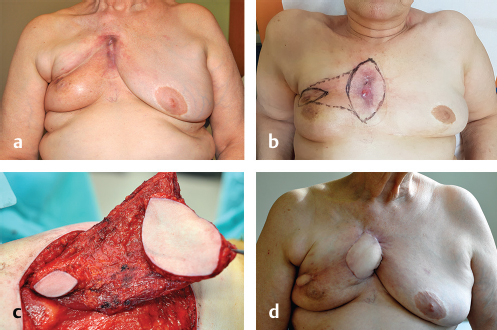
Breast retraction and shape distortion (▶Fig. 63.6; ▶Fig. 63.7).
Deformation of the reconstructed breast (▶Fig. 63.8).
Radionecrosis (▶Fig. 63.9; ▶Fig. 63.10).
Osteoradionecrosis (▶Fig. 63.11).
Radiation-induced tumors (▶Fig. 63.12).





63.4.1 Management of General Complications
Radiation Pneumonitis
Symptomatic radiation pneumonitis is less common when only the breast is irradiated as in the conservative treatment. The clinical symptoms appear 2 to 3 months after irradiation or even after 6 months, and they can be dyspnea, nonproductive cough, fever, shortness of breath, and radiologic changes. Symptoms can persist for several weeks and they are usually self-limiting. Radiologic lung injury is more common than symptomatic pneumonitis and can be identified using chest radiograph or a computed tomography (CT) scan. The incidence of radiation pneumonitis is about 1%. The incidence increases when chemotherapy, supplementary irradiated fields (supraclavicular), and tamoxifen medication are associated, and can reach up to 20%.
If the symptoms do not disappear and the discomfort is major, the radiation pneumonitis can be treated with prednisone 50 to 60 mg per day for 1 week, decreasing slowly by 10 mg/week.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


