62 Oncoplastic Reconstruction by Tumor Location and Outcomes
Summary
Oncoplastic techniques involve a combination of breast reduction techniques and creative use of local breast flaps for reconstruction of a given lumpectomy defect. This chapter serves to outline the various techniques available for lumpectomies lying within the different quadrants of the breast.
Key Topics
Surgical approaches and choice of technique.
Volume replacement techniques.
Autoaugmentation techniques.
Volume displacement techniques.
Delayed revision of postirradiation deformities.
Fat injection for correction of lumpectomy deformities.
Key Teaching Points
The oncoplastic technique selected will depend on the region of the breast to be reconstructed.
Breast blood supply has to be respected when designing parenchymal flaps.
Standard breast reduction pedicles can be used for many defects.
Great care should be taken when approaching the upper inner quadrant of the breast due to the paucity of available tissue.
62.1 Outcomes
62.1.1 Surgical Approaches and Choice of Technique
Volume displacement (parenchymal remodeling, volume shrinkage):
Primary closure.
Mirror biopsy/excision.
Reduction mastopexy techniques.
Nipple–areolar centralization.
Volume replacement (adjacent or distant tissue transfer, volume preservation):
Implant augmentation (rare).
Local flaps:
Fasciocutaneous flaps.
Perforator flaps.
Latissimus dorsi musculocutaneous flap.
Distant flaps.
Operative Sequence
Team discussion: decision to proceed with the oncoplastic breast conservation:
Immediate.
Delayed-immediate.
Preoperative marking:
Wire placement in breast imaging, if necessary.
Another team discussion (ablative and reconstructive surgeons).
Tumor excision, with or without lymph node sampling.
Mammographic confirmation with frozen sections, if appropriate.
Separate cavity sampling.
Clipping of cavity for orientation.
Evaluation of the deformity: size and location.
Intraoperative goals:
Eliminate dead space.
Preserve nipple viability, if possible.
Reshape breast to preserve shape.
Perform contralateral procedure for symmetry, if necessary.
Tissue displacement or tissue replacement technique.
When determining the best method of partial breast reconstruction, the surgeon needs to take into consideration the breast size, defect size, and tumor location. The two main categories include
Rearranging breast tissue (volume displacement techniques).
Importing new tissue (volume replacement techniques).
62.1.2 Volume Displacement Techniques
These procedures typically shrink or close the defect through mobilization of adjacent breast tissue, absorbing the volume loss over a larger area and decreasing the risk that a localized defect will develop.
Primary Closure
Simple closures are performed in smaller defects by mobilizing the parenchyma from the underlying fascia, redistributing the breast tissue, and closing the cavity in layers. More complex defects require additional parenchymal remodeling (▶Fig. 62.1).
Mirror Biopsy Techniques
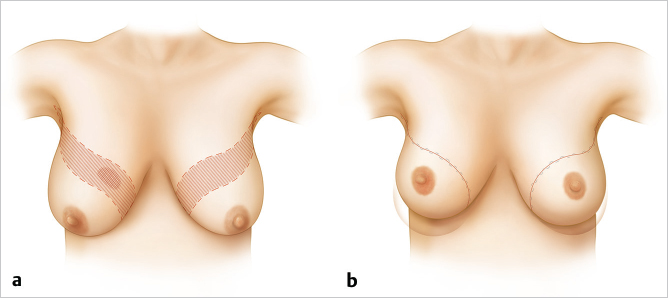
Mirror biopsy techniques are more commonly performed for larger quadrantectomy defects, especially in the upper pole, and allow symmetrical elevation of the breasts. Patients should be warned about the extensive scars associated with this procedure and their potential visibility when the mirror biopsy technique is used to correct upper pole defects (▶Fig. 62.2).
Mammaplasty
Oncoplastic reduction or mastopexy techniques are extremely versatile and are probably the most popular approach to managing partial mastectomy defects. In our practice, the vast majority of tumor defects can be reconstructed using this technique. Plastic surgeons are familiar with these techniques, making it easy to incorporate this approach into their reconstructive practices. In women with large or ptotic breasts, the numerous reduction patterns or pedicle designs allow remodeling of a defect in any location and size, as long as sufficient breast tissue and skin are available.
Creative mammaplasty designs can be made for complete removal of the lesion and reshaping of the mound. The mammaplasty markings are made preoperatively and the pedicle design is determined, depending on tumor location. Typically, if the pedicle points to or can be rotated into the defect, it can be used.
Communication with the resective surgeon is crucial to ensure that his or her approach is within the planned skin takeout pattern, if possible. If the tumor is located outside the proposed skin resection, it can be excised through a separate incision if it is superficially located, or through a remote incision within the reduction markings, as long as skin flap vascularity will not be compromised.
Occasionally, the planned pedicle or reduction technique is changed intraoperatively after evaluation of the deformity, which underscores the importance of having a backup plan. The cavity is inspected after the resection, with attention to the defect location in relation to the nipple, as well as the remaining breast tissue. Additional cavity samples are taken and the cavity is clipped. The nipple and dermatoglandular pedicle are dissected, and, if necessary, the remaining tissue is resected to complete the reduction. Occasionally, additional dermatoglandular or glandular pedicles can be created from tissue that might otherwise have been resected and rotated to autoaugment the defect if it is peripheral on the breast. The procedure is performed on the contralateral breast using a similar technique.
Technical Pearl
The ipsilateral side is typically kept about 10% larger to allow for radiation fibrosis.
If extensive nodal dissection is performed, drains are used.
62.1.3 Flap Selection with Parenchymal Autoaugmentation
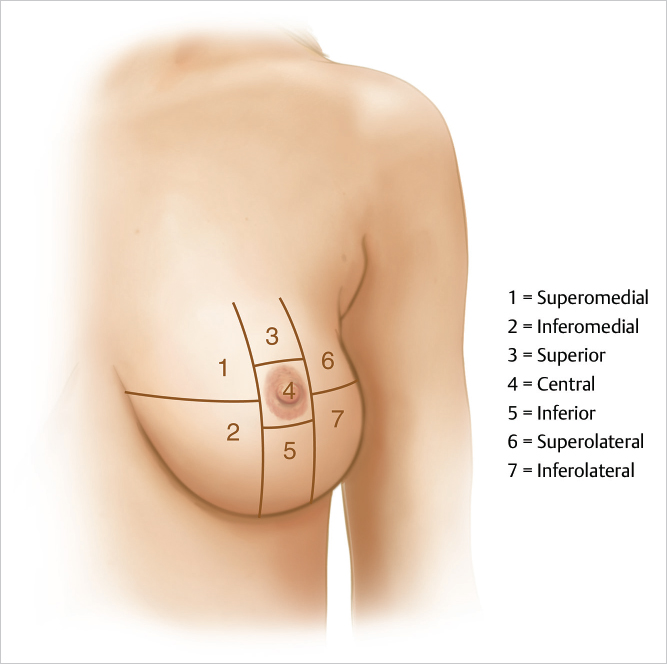
Pedicle selection to fill a given defect depends on the location of the tumor. Kronowitz describes seven areas or zones of the breast that can be used to determine pedicle location. The most difficult locations to treat are superomedial areas, where lack of adjacent breast volume tends to limit reconstructive options; women with large lower poles and cleavage are easier to manage in this area. High upper pole tumors can also be problematic unless a flap of breast tissue can be incorporated into an inferior pedicle as a pennant flap rotated up into the defect from below. However, vascularity can be an issue in this setting. These techniques essentially rebuild a smaller breast with the areola positioned in the center of the breast mound (▶Fig. 62.3; ▶Table 62.1)







Lower Quadrant Tumors
Women with larger breasts are ideal candidates for the oncoplastic approach. Quadrantectomy-type resections are possible, removing skin and parenchyma from this location, reshaping the breast using a superior or superomedial pedicle. Lower pole tumors in moderate-sized breasts can be excised along with skin as needed in the usual vertical pattern, using a superior pedicle followed by plication of the vertical pillars and vertical reduction on the contralateral side.
Inferior Lesions: Zone 5
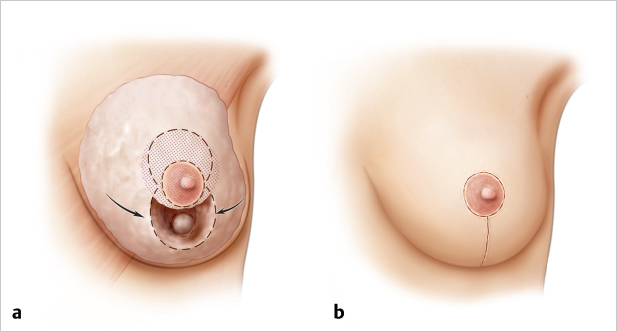
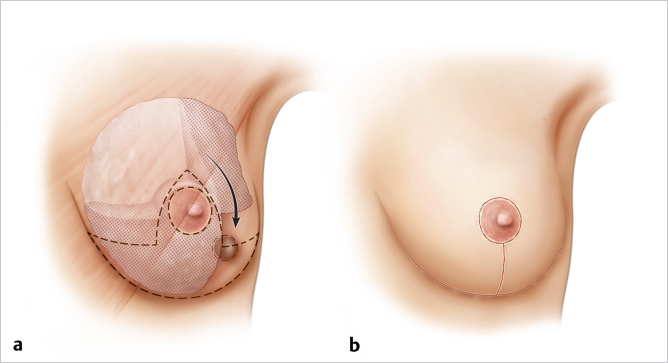
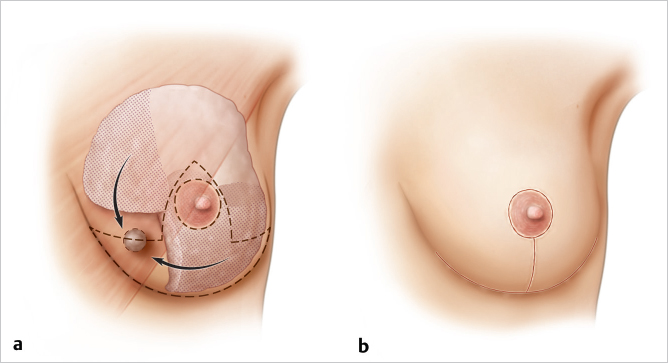
Inferior lesions in zone 5 are perhaps the easiest defects to fill, because they can be managed like a vertical Lassus or Lejour type of reduction closure. The tumor lies in the center of the lower pole and is resected much as in the standard breast resection of the Lassus procedure. This leaves medial and lateral pillars that are easily approximated, resulting in good coning of the final breast shape (▶Fig. 62.4)
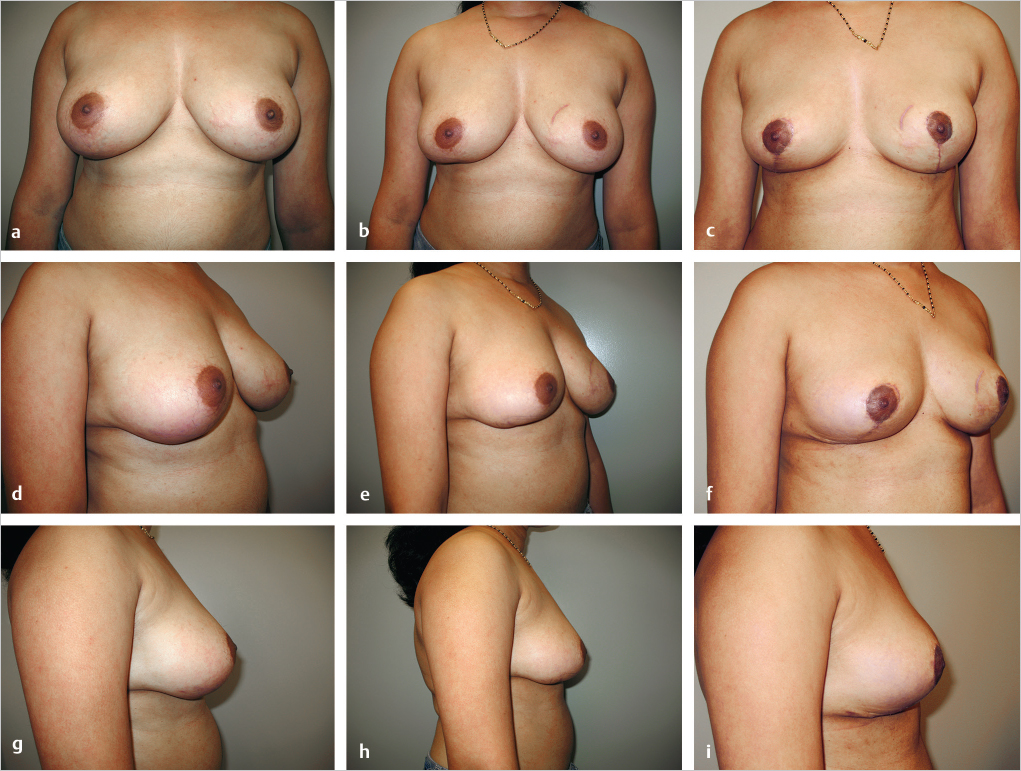
This 26-year-old woman presented with an aggressive phyllodes tumor of the right breast with high mitotic activity (▶Fig. 62.5). A lumpectomy resulted in a single positive margin laterally but several close margins; re-excision of the lower pole tumor was advised. The patient already had flattening of the lower pole of the breast as a consequence of her initial transverse resection (▶Fig. 62.5b,e,h). A wider resection of the initial operative site was planned using a Lassus-type vertical reduction pattern. This permitted resection of a large area of skin formerly close to the tumor and allowed easy closure with excellent restoration of contour, although at the expense of a smaller breast volume. The patient is delighted with the outcome. Shape and symmetry are good, and nipple sensation has been preserved.
Inferolateral Tumors: Zone 7
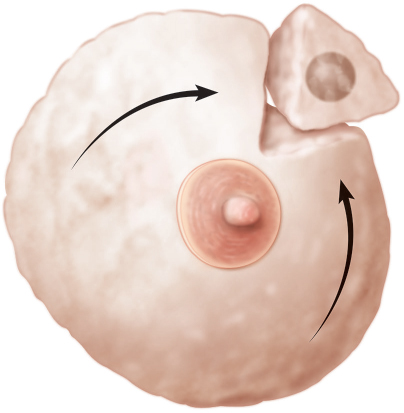
Inferolateral tumors of zone 7 are best closed with a superomedial pedicle incorporating an accessory flap of inferior central tissue to rotate into the lateral defect. The accessory pedicle should be broad based to maximize vascularity; it is rotated laterally for volume fill. Nipple–areolar displacement may be relatively minor with this procedure unless the patient wants a significant mastopexy or breast reduction (▶Fig. 62.6).
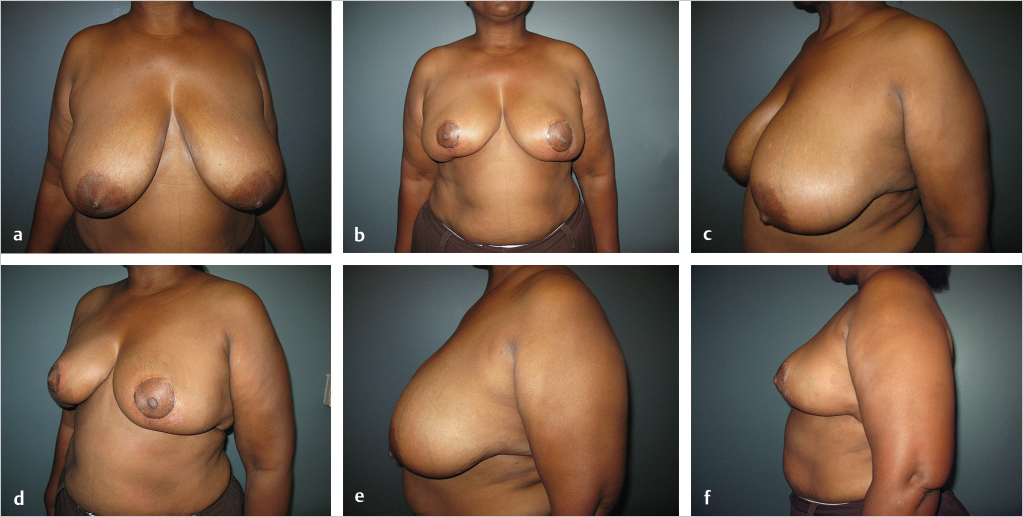
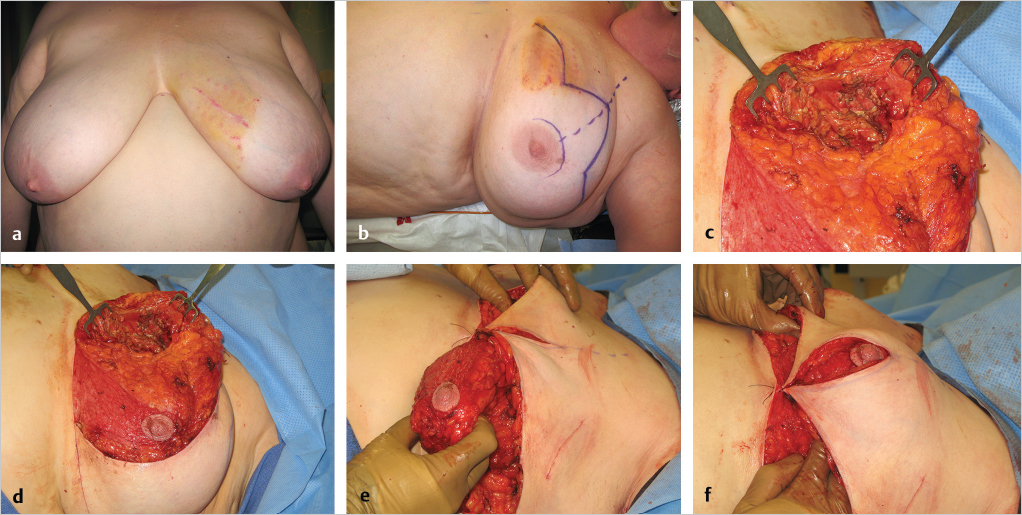
This 49-year-old woman had a grade 2 infiltrating ductal carcinoma in the inferolateral region of the left breast. She desired breast preservation; however, because of her large breasts and the tumor size and location, she was deemed a poor candidate for breast-conserving therapy (BCT) alone (▶Fig. 62.7).

The oncoplastic reduction approach was chosen to make her a better candidate for BCT and to minimize the risk of poor cosmetic results. She underwent a 400-g partial mastectomy; the margins were clear. After the cavity was clipped, her breast was reshaped using the reduction technique. A superomedial pedicle was chosen to preserve nipple viability, and an additional 200 g was removed. The remaining glandular tissue, along with the dermatoglandular pedicle, was used to fill the defect and reshape the breast mound. A similar contralateral reduction procedure was performed using the superomedial pedicle. A total of 650 g was resected from the right breast in anticipation of some breast fibrosis after radiation therapy (▶Fig. 62.8).

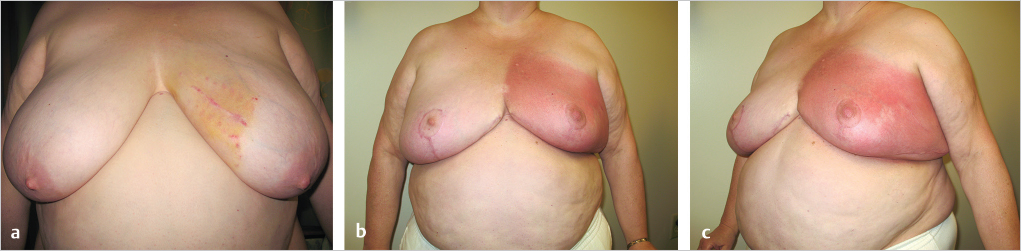
The patient’s early results are shown at 1 month postoperatively, just before radiation therapy was begun (▶Fig. 62.9).
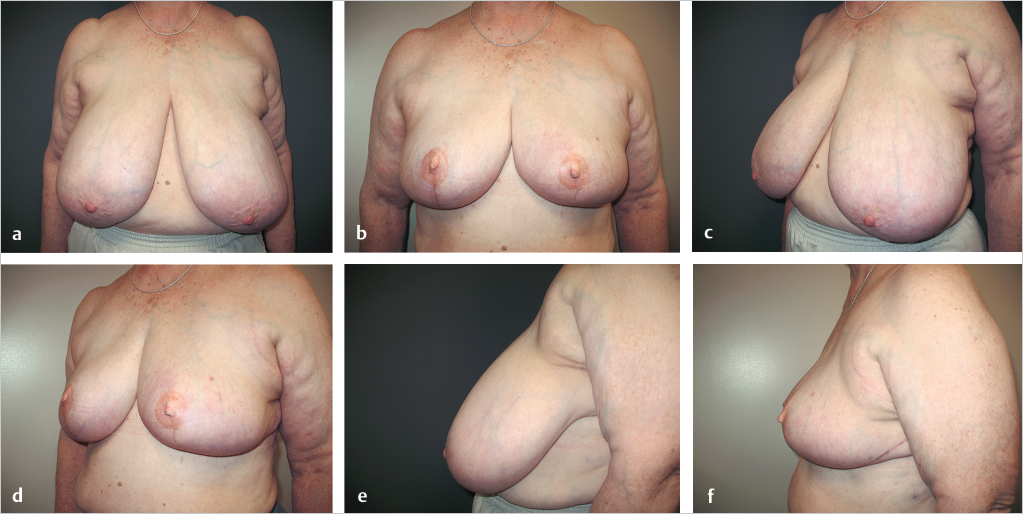
This 60-year-old woman had an inferolateral carcinoma of the left breast and was a candidate for BCT. Her breasts were extremely large and pendulous, with nipple-to-notch measurements of 41 cm and inframammary fold-to-nipple distances of 26 cm. Lower breast amputations with immediate nipple reconstruction were performed, because nipple grafts were considered risky in this obese smoker. She is shown 9 months postoperatively, with nipple–areolar reconstruction and tattooing. Her breasts remain soft, and symmetry is good (▶Fig. 62.10).
Inferomedial Tumors: Zone 2
The smaller the patient’s initial breast volume, the more difficult inferomedial defects are to reconstruct. Women with generous breast volumes de novo, particularly those with cleavage, have more tissue to transpose into the medial breast from the inferior central area. Small-breasted women may be too volume deficient to make breast conservation worthwhile. A tumor resection localized to the area of resection included in the standard inferior pedicle Wise pattern reduction will allow a very simple closure using standard breast reduction procedures, as shown above.
In smaller-breasted women, a parenchymal flap has to be advanced into the defect. This can be achieved using a superiorly based pedicle with an accessory block of inferior parenchyma from the lower pole. This may result in flattening of the lower pole if the patient does not have much inferior glandular ptosis with which to work (▶Fig. 62.11).
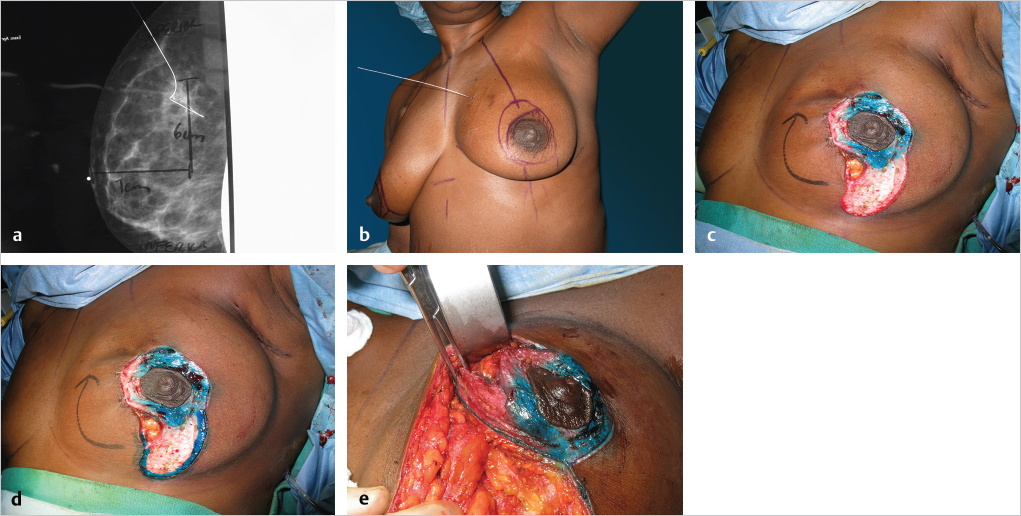
This 52-year-old woman with mammary hypertrophy and grade 3 ptosis presented with a 3.2-cm inferomedial tumor (zone 2). A lumpectomy was performed and 1 week later, after negative margins were confirmed, she underwent an inferior pedicle Wise pattern reduction with inferior displacement of upper medial breast fullness. Between this maneuver and positioning of the inferior pedicle, a 12 by 10 cm defect was completely filled, producing good breast shape and symmetry; 975 g was resected on the right and 734 g on the left (▶Fig. 62.12).
Postoperatively, she underwent 6 weeks of radiation therapy and is shown 3 weeks after completion of treatment. Shrinkage of the left breast is already apparent, and the skin flaps are tight and edematous (▶Fig. 62.13).
This 46-year-old woman had an infiltrating ductal carcinoma in the medial aspect of her left breast. She had minimal ptosis with relatively small breasts. Her mastectomy specimen weighed 40 g, leaving a defect in the medial breast, which is a cosmetically sensitive location. Her defect was filled with an extended superolateral dermatoglandular pedicle that was rotated medially; no additional tissue was removed. The inferior donor defect was closed in the usual vertical mastopexy fashion by plicating the medial and lateral pillars. In a similar procedure on the opposite breast, a small lower pole skin-glandular resection of 70 g was done (▶Fig. 62.14).
Autoaugmentation Techniques
Challenges were found using standard reduction techniques with certain tumor locations especially in women with smaller breasts. In order to reconstruct these defects, the use of autoaugmentation techniques has become more popular. The two main types are extending the primary nipple pedicle and rotating the extended pedicle into a remote tumor defect. The second type is to use a secondary dermatoglandular pedicle, which allows independent movement of the nipple and autoaugmentation pedicle. Upper or superior medial techniques can be filled using the extended superomedial or superolateral pedicle and rotating tissue from the lower pole to fill a defect above the nipple. As long as the blood supply to these flaps is respected and reconstructive principles are followed, the complication rate is no greater with additional autoaugmentation techniques.
Superior Quadrant Tumors: Zone 3
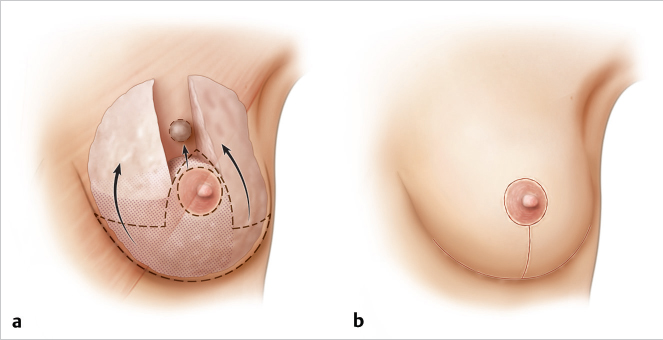
Tumor defects located between the 11 o’clock and 1 o’clock positions on the breast can be easily filled by advancing an inferior pedicle, particularly in larger-breasted women with ptosis. The correction is simple and involves little more than a conventional Wise pattern inferior pedicle approach. The higher the tumor on the chest wall and the thinner the patient, the more difficult this becomes. If there is a paucity of available tissue, glandular “wings” of parenchyma from the lateral and medial upper quadrants can be mobilized to help close the defect (▶Fig. 62.15).
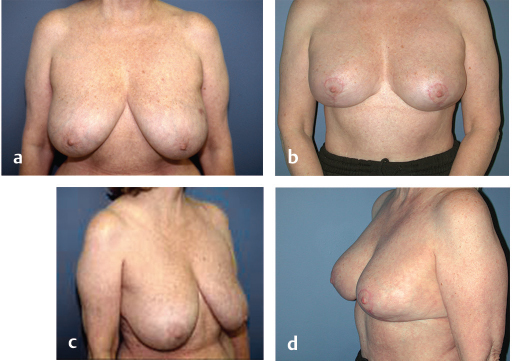
This 54-year-old woman presented with a 2-cm breast carcinoma at the 12 o’clock position above the nipple of her left breast. The lesion was 1.2 cm in diameter, and she opted for BCT. An inferior pedicle technique incorporating a Wise skin pattern was used. The superior translocation of the pedicle easily filled the lumpectomy defect, restoring excellent balance to the upper pole of her breast. She is shown 6 months after radiation therapy (▶Fig. 62.16).
This 39-year-old woman had a right breast upper pole tumor. She had relatively small ptotic breasts, with a significant potential for breast deformity after resection. The tumor required a 163-g resection, leaving a full-thickness defect lying above the location of the proposed nipple position. Insufficient glandular tissue was present above the nipple to fill the dead space using an inferior or central mound alone. This would have left a volume void above the nipple. We rotated glandular flaps from the medial and lateral breast mound to fill the volume void above the nipple (▶Fig. 62.17).
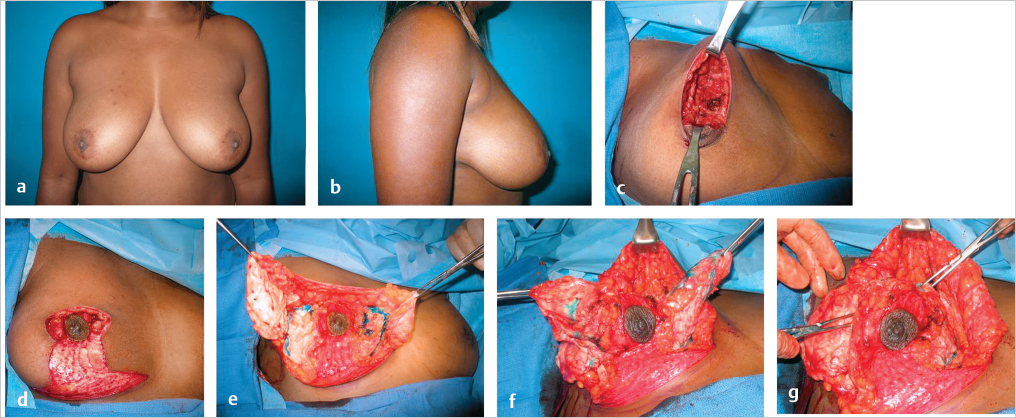
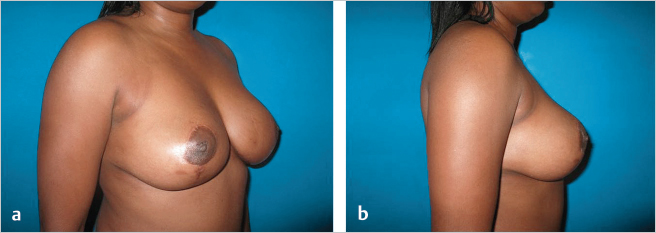
The skin was then redraped over the breast mound using the standard Wise technique. A contralateral mastopexy was performed using a central mound; 183 g was resected. Early results showed preservation of shape and symmetry (▶Fig. 62.18).

At 2-year follow-up, the upper pole contour was good (▶Fig. 62.19).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


