Abstract
The aging face changes in multiple facets. Although surgery is the gold standard to treat laxity and attenuation of the retaining ligaments, resurfacing techniques can address textural and other surface changes related to aging and environmental damage. Dermabrasion is one highly effective, reliable, and low-cost method to facial resurfacing. It is particularly useful for vertical perioral rhytides.
61 Dermabrasion of the Face
Key Points
The perimeter of any area being treated should be “feathered” to minimize the creation of a transition zone between dermabraded and nondermabraded tissue.
The key to dermabrasion is to keep the skin on tension at all times.
The endpoint of dermabrasion is a combination of pinpoint bleeding and visualization of the rhytid effacement. The ideal goal is to completely efface the targeted rhytid before dermabrading too deep and damaging the melanocytes.
61.1 Preoperative Steps
Indications for dermabrasion are broad and can include desire to improve skin texture, reduce visible fine lines, or reduction in age spots (such as solar keratosis).
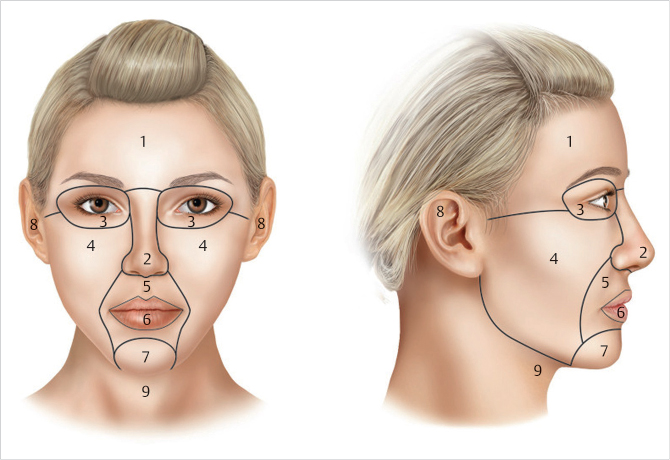
Dermabrasion can be performed on the entire face and neck, or can be isolated to specific aesthetic units such as the glabella or perioral region (Fig. 61.1).
Dermabrasion can be performed as a stand-alone procedure or in combination with facelift and necklift.
The primary consideration for preoperative planning is the patient’s skin tone. The more pigmentation in the skin, the higher the chance for postdermabrasion complications such as postinflammatory hyperpigmentation or areas of hypopigmentation.
Some providers choose to pretreat patients with a retinol or bleaching agent for 4 to 6 weeks prior to dermabrasion. The authors do not use pretreatment.
It is important to elicit a history of oral herpes so that these patients can be pretreated with antiviral medication (Fig. 61.2).

61.2 Operative Steps
61.2.1 Markings and Positioning
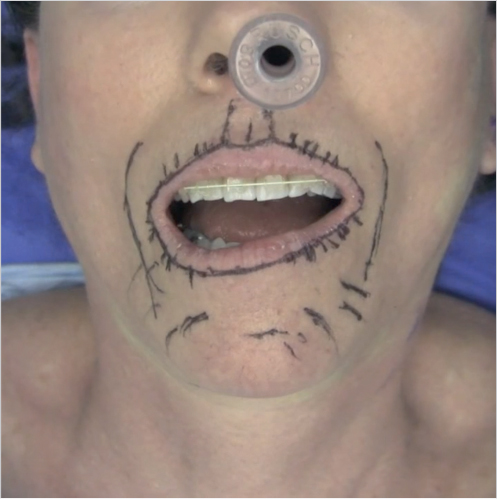
A marker is used preoperatively to stain the fine lines which the dermabrasion is targeting (Fig. 61.3).
The patient is supine on the procedure table.
Usually the head of bed is slightly elevated.
The provider should be sitting for maximum stability.
The approach can be accomplished using a variety of techniques that yield a controlled, reproducible distribution of mechanical resurfacing in the skin.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


